Department of Radiology Boston Children’s Hospital, Harvard Medical School
Ricardo Restrepo
Department of Radiology Nicklaus Children’s Hospital, Florida International University
Edward Y. Lee
Department of Radiology Boston Children’s Hospital, Harvard Medical School
Since the publication of our initial AJR article, “Pediatric SARS, H1N1, MERS, EVALI, and Now Coronavirus Disease (COVID-19) Pneumonia: What Radiologists Need to Know”, the coronavirus disease (COVID-19) pandemic has continued to grow—more than 15.7 million cases and 640,000 deaths worldwide, as of July 26, 2020. During this time, understanding of the imaging manifestations related to pediatric COVID-19 pneumonia, and the more newly defined COVID-19-related entity multisystem inflammatory syndrome in children (MIS-C), has continued to increase; however, substantial uncertainty regarding the imaging findings of pediatric COVID-19 and MIS-C still exist. Our article highlights a few key points regarding what is currently known about the imaging findings of pediatric COVID-19 and MIS-C for practicing radiologists.
What is Typical Pediatric COVID-19?
A recent meta-analysis of 7,780 pediatric patients positive for COVID-19 found that the mean age of patients was 8.9 years with a slight male predominance (55.6%). Underlying comorbid medical conditions were identified in 35.6% of patients. Overall, pediatric patients demonstrated a more mild clinical course than adults with 19.3% of patients completely asymptomatic, 3.3% requiring intensive care, and only 7 reported deaths (0.09%). The most commonly observed clinical complaints among symptomatic patients were cough and fever, and elevated inflammatory markers such as C-reactive protein, procalcitonin, and interleukin-6 were frequent.
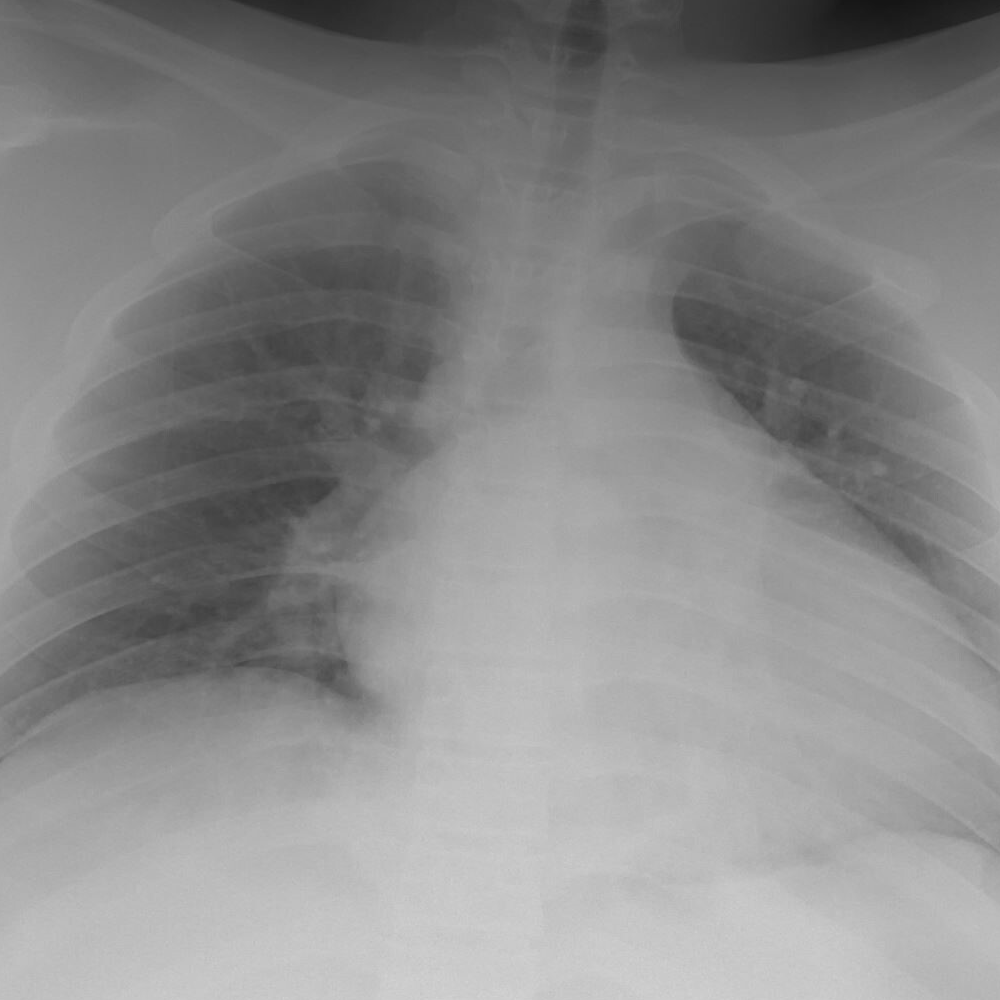
Radiographically, typical imaging findings of pediatric COVID-19 pneumonia have been characterized as bilateral peripheral and/or subpleural ground-glass opacities and/or consolidation in a lower-lobe predominant distribution.
Fig. 1—13-year-old female with obesity and positive COVID-19 reverse transcription–polymerase chain reaction test who presented with fever and severe shortness of breath. (A) Frontal chest radiograph shows bilateral lower lung zone-predominant consolidation and ground-glass opacities, which are typical chest radiographic findings of pediatric COVID-19 pneumonia. (B) Axial lung window CT image demonstrates diffuse peripheral predominant ground-glass opacities in both lungs.
Although a unilateral or bilateral distribution of parenchymal abnormality may be observed in pediatric COVID-19 pneumonia, the differential for unilateral disease is somewhat broader. Thus, a unilateral distribution has been defined as indeterminant. The halo sign, a rounded consolidation surrounded by a rim of ground-glass opacity, can be seen during the early phase of pediatric COVID-19. Therefore, the halo sign is also considered typical when present in an immunocompetent patient, as it has a narrow differential. Additional important considerations for radiologists are atypical imaging findings that raise concern for alternative diagnosis, including centrilobular nodules, focal segmental/lobar consolidation, cavitary lesions, pleural effusion, and lymphadenopathy.
What is Multisystem Inflammatory Syndrome in Children (MIS-C)?
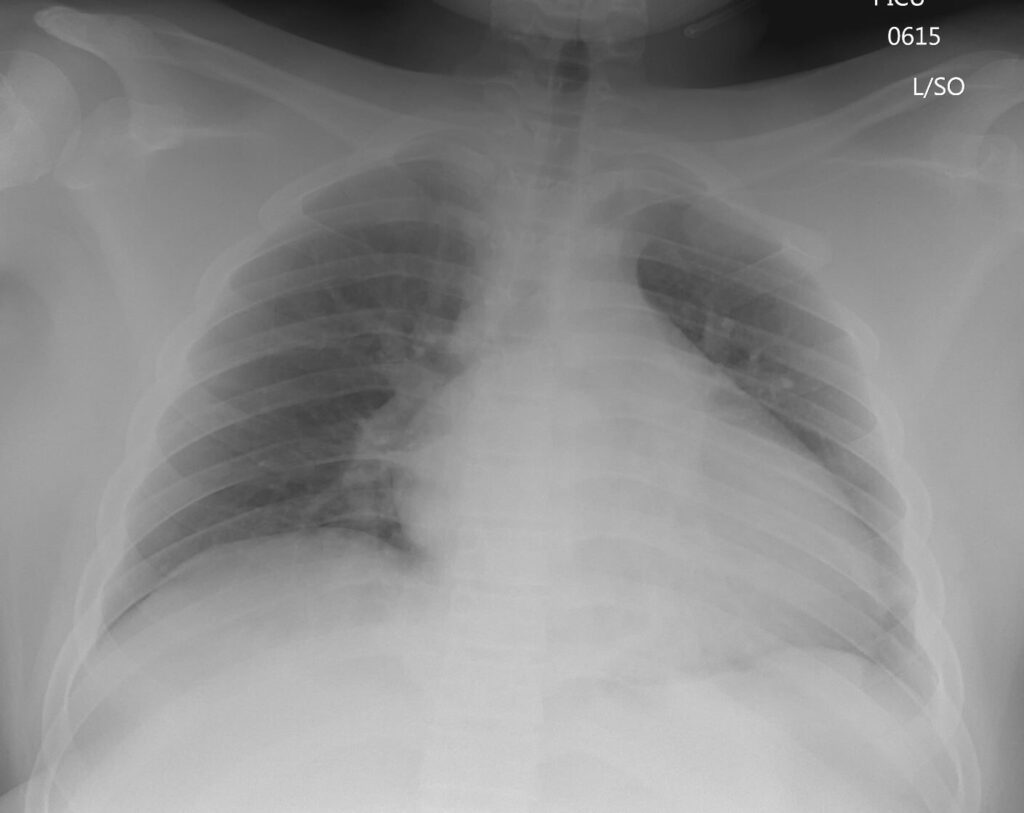
Fig. 2—15-year-old male, reverse transcription–polymerase chain reaction test positive for COVID-19, who presented with MIS-C associated with COVID-19, with symptoms including fever, vomiting, and diarrhea. Frontal chest radiograph shows cardiomegaly. Subsequently obtained echocardiogram demonstrated dilated left ventricle and moderate systolic dysfunction.
Whereas typical COVID-19 pneumonia presents with bilateral peripheral and lower-lobe predominant ground-glass opacities and consolidation, the distribution of pulmonary parenchymal abnormality in MIS-C tends to be central and perihilar in distribution and more frequently presents as increased pulmonary vascularity, although airspace consolidation may be seen in advanced stages of cardiac failure. Additionally, cardiomegaly and pleural/pericardial effusions are often observed in MIS-C, but they are rare in pediatric COVID-19 pneumonia.
Extra-thoracic Findings
Extra-thoracic manifestations are not generally observed in pediatric COVID-19 pneumonia. However, as may be expected in an inflammatory disorder involving multiple organ systems, extra-thoracic findings are not uncommon in MIS-C—especially in the abdomen. Reported intra-abdominal abnormalities in MIS-C include bowel wall thickening, ascites, right lower quadrant fat stranding and/or lymphadenopathy, hepatomegaly, gallbladder sludge and/or pericholicystic fluid, and increased renal cortical echogenicity.
Fig. 3—7-year-old girl, reverse transcription–polymerase chain reaction test positive for COVID-19, who presented with MIS-C associated with COVID-19, with symptoms including fever, vomiting, abdominal pain, and hypotension. Transverse grayscale ultrasound image of the right lower quadrant shows thickened bowel loops (arrows) and ascites (asterisk).
Five Take-Home Points for Diagnostic Radiologists
“Typical” pediatric COVID-19 pneumonia presents as bilateral peripheral and lower-lobe predominant ground-glass opacities/consolidation + halo sign.
Centrilobular nodules, parenchymal cavitation, focal lobar/segmental consolidation, pleural effusion, and lymphadenopathy are atypical in pediatric COVID-19 pneumonia.
MIS-C has a more severe clinical course than pediatric COVID-19 pneumonia, often involving > 4 organ systems, with up to 85% of patients requiring intensive care.
Thoracic imaging findings observed in MIS-C, including cardiomegaly, pleural/pericardial effusion, coronary artery dilation, or pulmonary embolism, differ from typical findings in pediatric COVID-19 pneumonia.
Extra-thoracic manifestations are not uncommon in MIS-C and generally are a manifestation of inflammatory change (bowel wall thickening, lymphadenopathy, fat stranding, pericholicystic fluid, ascites) and/or organ dysfunction (hepatomegaly, increased renal cortical echogenicity).
As our understanding of pediatric COVID-19-related disease continues to grow, it is essential for practicing radiologists to be aware of the imaging findings in this patient population. Additionally, as the imaging features are quite different, awareness of the differences between pediatric COVID-19 pneumonia and MIS-C are critical to accurate diagnosis and optimal management of pediatric patients.
Professor of Radiology NYU School of Medicine Center for Advanced Imaging Innovation and Research Laura and Isaac Perlmutter Cancer Center
Published June 22, 2020
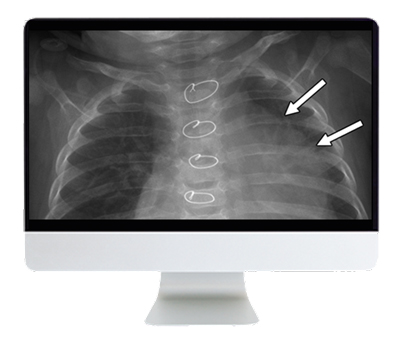
Breast cancer is the most common cancer in women worldwide with approximately 2 million cases diagnosed each year. In the United States, breast cancer is the second leading cause of cancer-related mortality among women. Multiple studies showed that regular screening mammography reduced breast cancer mortality by 40% or more. However, this year, we learned that men at high risk of developing breast cancer may benefit from mammography.
Screening of Men at High Risk for Breast Cancer
Researchers at NYU School of Medicine conducted the largest review in the United States of the medical records of men who have had a screening mammogram. The study involved 1,869 men, ages 18 to 96, who had a mammogram between 2005 and 2017. Some men sought testing because they felt a mass in their breast, while others had no symptoms and wanted to be screened because a family member had recently received a breast cancer diagnosis. In total, 41 men were found to have breast cancer, as confirmed by breast tissue biopsy. Among the 271 men who had screening exams, 5 had the disease. All those with breast cancer had surgery (mastectomy) to remove their tumor. A key finding was that mammography was more effective at detecting cancer in men with high risk than is the norm for women with average risk of breast cancer. For every 1,000 exams in these men, 18 had breast cancer. By contrast, the detection rate for women is roughly 5 for every 1,000 exams.
Among the study’s other main findings was that men who had already had breast cancer were 84 times more likely to get it again than men who had no personal history of the disease. Men with an immediate relative who had breast cancer, such as a sister or mother, were three times more likely to develop the disease. Other men with elevated risk of breast cancer included those of Ashkenazi descent, an ethnic group widely known for high rates of some cancers (who were 13 times more likely to get breast cancer than non-Ashkenazi men) and those who had genetic mutations, such as BRCA1 or BRCA2 (up to 7 times more likely than men with no genetic risk). Current National Comprehensive Cancer Network Guidelines only recommend checking for breast cancer as part of annual physical exams, not using more sensitive imaging tests like a mammogram, for men age 35 and older with BRCA mutations. The take-home point is that men need to be more aware of their risk factors for breast cancer and that they, too, can develop the disease.
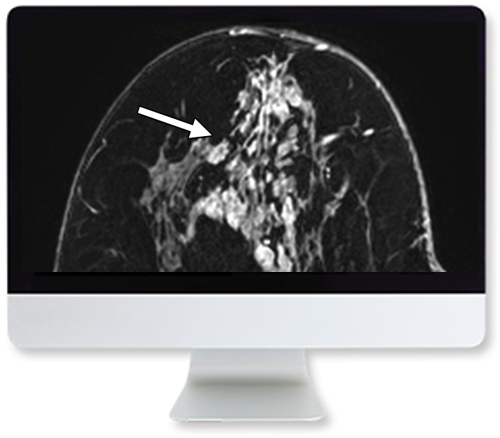
Contrast Enhanced Spectral Mammography
Another exciting development is that the armamentarium that radiologists have to detect breast cancer continues to expand. The latest imaging tools focus on functional imaging tests that reveal physiological activities within the breasts. Functional imaging includes measuring changes in metabolism (e.g., PET/CT or PET/ MRI), changes in the tumor cellularity (diffusion weighted imaging on MRI), regional chemical composition (MR spectroscopy, sodium MRI) and changes in blood flow. The increase in the number of blood vessels (neoangiogenesis) and the increased permeability of blood vessels that feed a tumor are the two main factors that account for uptake of gadolinium that leads to the enhancement of breast cancers on MRI. But MRI is expensive, and we know that iodine based contrast may also be used to detect breast cancer. As a result, contrast enhanced spectral mammography (CESM) is being used in both the screening and diagnostic setting. Similar to breast MRI, CESM identifies the increased blood flow associated with breast cancer and is largely independent of breast density.
Compared with MRI, clinical implementation of CESM is much easier and at much lower costs. CESM requires an intravenous injection of iodinated contrast (dose 1.5 ml/kg) and a dual energy mammography system. A “low-energy” acquisition image resembles a normal mammogram, whereas a “high-energy” image, using a keV above the k-edge of iodine, will enhance with the contrast agent signal. Images are performed in the standard craniocaudal and mediolateral mammographic views. The postprocessing, recombined iodine-only mammograms will identify enhancing lesions. Studies show that CESM has good diagnostic accuracy when used to evaluate the extent of disease in women newly diagnosed with breast cancer. Like breast MRI, CESM outperforms combined mammography and ultrasound in the detection of additional disease and in assessment of tumor size, compared with pathology. The literature reports that CESM has a small reduction of sensitivity, while providing a higher specificity compared with breast MRI in the evaluation of tumor extent.
In addition, CESM works well as a screening exam with an additional cancer detection rate 6.6 – 13.1/1,000 over conventional mammography. Therefore, it may be feasible to screen a larger population of women (e.g., women at moderately increased risk for breast cancer), and it may be advantageous to use CESM over breast MRI in this subset of women. Overall, CESM is a safe technique with a modest increase in the radiation dose compared to conventional mammography. Also, serious adverse contrast reactions are infrequent. Currently, the lack of a CESM-compatible biopsy device for lesions exclusively seen on CESM is a limitation of this new technique.
Abbreviated Breast MRI and Ultrafast MRI
Recently, many authors have evaluated the potential of an abbreviated breast MRI to increase the accessibility of breast MRI, especially for the screening of women at above-average risk for breast cancer. The conventional breast MRI exam is a 30-minute examination that is expensive and not well tolerated by some patients. These factors, along with the limited availability of MRI scanners, preclude population-wide screening with breast MRI. Abbreviated MRI, with shorter image acquisition and interpretation times, may increase the availability of breast MRI and reduce the costs. The basic abbreviated breast MRI protocol includes a pre-contrast and one post-contrast T1-weighted imaging, along with subtraction images and maximum intensity projection images. Multiple variations on this basic protocol have been evaluated. These protocols exploit the high sensitivity of MRI, while reducing acquisition and interpretation times. A recent review of 21 studies on abbreviated breast MRI, performed in eight different countries and in over 4,500 women, confirmed the diagnostic accuracy was similar to the full breast MRI protocol.
With stronger magnets and improvements in breast coils and MRI software, ultrafast sequences have been developed to measure the rapid arterial perfusion and the rapid venous drainage of breast cancers. The temporal resolution of ultrafast protocol is typically less than 10 seconds/frame and may be incorporated into abbreviated or full breast MRI protocols. The hope is that imaging faster may allow radiologists to better distinguish between benign enhancing lesions and background parenchymal enhancement from breast cancers. Ideally, ultrafast MRI sequences may allow for increasing the specificity of abbreviated breast MRI, without increasing the scan time.
Artificial Intelligence
Without a doubt, artificial intelligence (AI) is the most talked about new diagnostic development in the field of radiology. Breast imaging is at the forefront of this research because we have decades of experience using computer-aided detection (CAD). Further, similar to chest radiography, large numbers of screening mammograms are available to be converted into datasets to train these AI algorithms. These new deep learning–based CAD models are proliferating due to recent breakthroughs in computer technology, data science, and algorithm development. Computer processing speed and memory have increased exponentially, owing to faster graphics processing units and parallel processing. Simultaneously, there have been mathematical advances that enabled the use of complex and multilayered neural networks, which led to a markedly improved performance of machine interpretation of highly standardized imaging tasks (e.g., predictions of cancer or no cancer).
New CAD platforms will differ from traditional CAD in several important ways. Some of these deep learning models no longer require manual feature design and minimize training with humans (i.e., radiologists). These AI algorithms learn discerning features that are best predictive of outcomes independently and may identify novel imaging features that are imperceptible to the human eye. The capacity for continuous feedback and learning will allow deep learning–based CAD to improve over time. In theory, deep learning algorithms can be trained for pattern recognition of image data (pixel-related information), correlate that data to tumor registry data (the truth), and assess risk when it recognizes a similar pattern (predict likelihood of cancer). Further feedback into the AI algorithm of whether that prediction is correct and truth-based will improve its performance in the future. New CAD systems may eventually be able to identify novel features associated with more relevant cancers by incorporating patient- and tumor-level variables—a task that is now performed in small groups of patients, usually in the research setting. This design has the potential to maximize the mortality benefit of breast cancer screening and to address the issues of overdiagnosis and overtreatment. Therefore, there is hope that these deep learning algorithms may hold real potential to improve clinical care.
Clinical Case-Based Review of Breast Imaging
Focus on honing your breast imaging diagnostic skills. This special course combines didactic lectures and rapid fire case review sessions to provide deeper insights into breast imaging.
The literature on these AI algorithms for mammography shows that their performance for lesion detection and classification are approaching that of radiologists. A preliminary study showed a similar diagnostic accuracy for an AI algorithm that evaluated screening digital breast tomosynthesis exams. It is anticipated that these AI algorithms will play a major role in screening in the near future, both to improve the quality of the screening programs and to assist with the increasing workload of interpreting screening mammograms. Furthermore, early studies suggest that when AI models predict a very low likelihood of malignancy, these mammograms may be triaged and interpreted by the algorithm alone, saving time and resources.
Other potential applications for screening mammography deep learning models beyond lesion detection and classification include assessment of mammographic breast density. This quantitative analysis of breast density is important because supplemental screening is recommended in women with mammographically dense breasts. A more recent development is utilizing these AI algorithms to predict a woman’s risk for developing breast cancer in the future by incorporating the normal mammographic parenchymal pattern (density, texture, etc.). Risk assessment may be further personalized when information from the electronic health record is included in deep learning risk models. The addition of radiogenomics, which combines radiologic phenotypes with underlying genetic signatures, has the potential to add relevant tumor and patient predictive and prognostic information using information extracted from images.
Although there is a lot of excitement about AI, many experts urge caution because these AI tools haven’t been evaluated in a wide variety of clinical settings. Most studies on AI and breast imaging are retrospective enriched reader studies. To increase the generalizability of the results, prospective studies in different patient populations should be performed.
It is clear that the “one size fits all” approach may no longer be relevant. Instead, the standard mammograms, ultrasounds, and breast MRI exams are being tailored for specific clinical indications, often augmented with AI tools.
On Thursday, March 19, the governor of California issued a mandate for state citizens to stay at home and not congregate, except for essential and emergency needs. I manage the radiology department at the University of California-San Diego, and needless to say, this mandate was therefore of particular and great interest to me. At the time, I saw this as a brave and decisive move on the governor’s part. Given the lack of other governors showing the wisdom of consensus in such an action, I also felt this instance of decisiveness demonstrated a high degree of confidence in his advisors and his own perspective. Many of us were paying attention to a number of news stories that suggested our lives were about to be significantly disrupted.
Ever since December 2019, as with many of my acquaintances and family members, I had been following at a distance and with one eye the epidemic in Wuhan. My attention and interest increased exponentially as December proceeded and Wuhan locked down tighter and tighter, then as December turned to January with mounting casualties, and more so as various reports regarding the impact of the epidemic and control measures on citizens came to light. Perhaps many of us even preceding this pandemic have a personal story regarding the invisible erstwhile masters of the universe, or something related. I certainly did. My personal story dealt with the swine flu vaccination of 1976. I was very close to my maternal grandparents. My maternal grandfather was on a ventilator for two weeks, and at one point, he could only blink due to Guillain-Barré syndrome. We held our own breaths as he very slowly improved. It took him two long years to fully recover. As a consequence, I was fascinated by virology in medical school as a result of my grandfather’s misadventure, which regrettably was about 34 years in the past. Perhaps I paid just a little more attention to epidemics and cures than the average citizen.
Somehow, seeing two hospitals erected in one week—the first with 1,000 beds and the second with 1,300 beds—was a firm nudge in the ribs for me. Firstly, I felt that was an impossibility for any of the environments that I have worked, meaning if we ever had to add a thousand hospital beds in a week, we couldn’t possibly do it. Second, it underscored the seriousness of the situation and that the epidemic may well be headed to our shores.
So, I read up on the popular culture sounding boards dealing with the 1918 influenza epidemic, SARS in 2002, H1N1 in 2009, and MERS in 2012. Naturally, I also went back to the bubonic plague. Reading did not build up my confidence.
As the shelter edict was issued in California, immediate and rapid changes in our delivery of health care took place. These changes influenced and affected our faculty, our residents and trainees, our patients, our clinical operations, our research, and our staff. Research came to a near grinding halt, and clinical volume dropped by 75% overnight, levelling off at 45% down. We wrestled with a span of consequences, from “how do we teach remotely?” to “what do we do with idle staff?”
Dr. Norbash explains how The Roentgen Fund® supports innovation in the radiology field.
Our elective cases nearly instantaneously and precipitously dropped in number as patients sheltered at home, and we realized how much of our volume was truly nonurgent and nonemergent. Our residents and technologists and faculty bravely and selflessly provided the same exceptional level of service they had always provided, only now with the understanding and belief that there is increased risk of harm to self. We watched the calendar and counted the days, preparing to the best of our abilities for the inevitable tsunami to hit. Our leadership assembled emergency plans with exceptional sophistication and creativity, doubling our ICU beds and creating standard operating procedures overnight in droves. Nearly three weeks later, the tsunami hasn’t hit us. We have, however, watched closely and day by day as our worst nightmares unfolded across the country, in New York City, where unparalleled compassion, ingenuity, and creativity have been demonstrated by our remarkable colleagues. The rest of us are petrified that what New York City is experiencing could be our future, and we convince ourselves that our lesser population density and lack of success with mass transit somehow protects us.
We really don’t know when and how this is going to end. Maybe, by the time you read this, the whole thing is over and solved. Maybe we are seeing multiple tsunamis scattered across the country battering us on a daily basis. As I write this, we certainly don’t know if San Diego is relegated to a gentle slope for an infinity, necessitating masks and social distancing forever, rather than a bump or a tsunami with an implied and potential resolution of sorts. In the meantime, we are relieved to have been spared massive carnage up until now, although there still are lost lives with the accompanying scarring, sorrow, and regret one would expect. In the meantime, we are trying to understand how to provide our faculty and staff some semblance of a paycheck when revenue is down by 40%, giving them a heightened sense of purpose with a sprint that is turning into a marathon, which will be progressively more difficult if and as this crisis stretches into the summer, fall, and possibly beyond. Not knowing is the most difficult part. We need to salvage the critical, scientific, and teaching missions that distinguish us, in preventing irreparable damage to what keeps us distinct and gives us unique value: teaching and discovery.
Many predict that the lockdown will be extended to the end of May, and some predict the end of June. Just today, a newsfeed quoted an extremely influential billionaire stating we won’t be over COVID-19 until Fall 2021. There’s much discussion regarding how much unemployment and financial instability we collectively will tolerate. We, as a people, are not in all instances risk averse. After all, we have states where motorcycle riders can ride without helmets, and legions of humans still smoke cigarettes. We also have too many people who suspect the value of immunizations. There is also much discussion regarding how we will deal with multiple recurrent waves of COVID-19 rising proportionately with our inevitable societal lapses in vigilance and awareness, if COVID-19 becomes an annual affair.
In the moment, I am inspired by my colleagues throughout the health system. My fellow radiologists are optimistic and creative, perpetually showing their innovative and flexible spirit. Every day there are new solutions and new approaches percolating among them, as they do their best to ensure optimal deployment of our tripartite mission. All this in graceful partnership with technologists, nurses, front desk staff, and trainees. Our brilliant departmental resident AI scientists have even deployed an intelligent tool in our PACS that will catch pneumonias, which may be too subtle for the naked eye to see. In the middle of this crisis, there are blinking flashes of creativity going off like lightbulbs. Everywhere under this roof, radiologists as tinkerers and creative spirits who are solving problems, as we elevate and illuminate each other’s vision.
I can’t imagine a better group of compatriots to have in my lifeboat.
Associate Professor of Radiology and Biomedical Informatics,
Division of Cardiothoracic Imaging, Nuclear Medicine and Molecular Imaging
Department of Radiology and Imaging Sciences, Emory University
Dr. De Cecco is a consultant for/receives institutional research support from Siemens.
Published April 22, 2020
On January 30, 2020, the 2019 novel coronavirus disease (COVID-19) was declared to be a global health emergency by the World Health Organization. Four months later, the virus is still spreading all over the globe—more than 3.3 million confirmed cases and 235,000 deaths worldwide—with the United States the most affected nation, numbering more than 1.1 million cases and over 65,000 deaths. Dramatic containment measures have been put into place to halt the diffusion of the virus, yet worldwide health care systems are still struggling with the massive influx of COVID-19 patients.
Currently, reverse transcription–polymerase chain reaction (RT-PCR) serves as the gold standard for the diagnosis of COVID-19. However, chest radiography and CT play an important role in the management of patients affected by COVID-19 from diagnosis to treatment response assessment, depending on the clinical situation and particularly in the early days of the outbreak and in specific geographic areas where RT-PCR tests are not readily available. In these situations, chest radiography as first-line imaging and chest CT in complex cases can provide assistance to clinicians by identifying suspicious findings for COVID-19.Xu Z, Shi L, Wang Y, et al. Case report pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir 2020; 8:420–422
Wong HYF, Lam HYS, Fong AH-T, et al. Frequency and distribution of chest radiographic findings in COVID-19 positive patients. Radiology 2019; 27:201160
Zhong B-L, Luo W, Li H-MH, et al. Sensitivity of chest CT for COVID-19: comparison to RT-PCR. Lancet 2020; 395:A1–A2
Lee YP, Jin Y, Fangfang Y, et al. Imaging profile of the COVID-19 infection: radiologic findings and literature review. Radiology 2020 Feb 13 [Epub ahead of print] Besides diagnosis, these images can be used to analyze or predict disease progression and severity. In the long term, chest CT imaging will likely play a role in the follow-up of patients with COVID-19, with possible development of long-term sequela, such as pulmonary fibrosis.
Artificial intelligence (AI) algorithms applied to patients with confirmed COVID-19 or subjects under investigation offer the potential to develop a more accurate automated approach for early detection and prognostication using the combination of clinical and imaging data. At the moment, several AI solutions are being developed for application in different stages of the COVID-19 diagnostic workflow, from diagnosis to prognosis.
AI for Classification of COVID-19 Pneumonia
In the early COVID-19 outbreak, radiographic and CT evaluations have been extensively utilized for diagnostic purposes due to their fast acquisition times. AI can be applied to develop algorithms that quickly learn COVID-19 pulmonary patterns from large datasets, as well as using similar manifestations from other types of pneumonia.
Radiography-Based AI Classification
Chest radiography is often used as an initial imaging test. Although generally considered less sensitive than chest CT, chest radiography can provide important information about the pulmonary status of COVID-19 patients, especially in more severe cases. A study by Wong et al. reported that abnormal chest radiographic examinations were found in 69% of patients at admission and 80% of patients at a later time during hospitalizationWong HYF, Lam HYS, Fong AH-T, et al. Frequency and distribution of chest radiographic findings in COVID-19 positive patients. Radiology 2019; 27:201160. COVID-19 presents itself mainly as airspace opacities, ground-glass opacity (GGO), and consolidation at a later stage. Bilateral, peripheral, and lower-zone involvement is observed in 90% of cases, while pleural effusion is rarely described. There are a few AI studies using radiographic images to detect and diagnose COVID-19-related pneumonia from other types of pneumonia and healthy subjects. Wang et al. proposed a deep convolutional network to classify COVID-19-related pneumonia using the largest COVID-19-related database so far, including radiographic examinations in 1,203 healthy patients, 660 patients with viral pneumonia, and 45 patients with COVID-19 Wang L, Wong A. COVID-Net: a tailored deep convolutional neural network design for detection of COVID-19 cases from chest x-ray images. arXiv website. arxiv.org/abs/2003.09871. Published Mar 22, 2020. Updated Apr 15, 2020. Accessed May 7, 2020 . They achieved an overall accuracy of 83.5%. Ghoshal et al. reported the use of a Bayesian convolutional neural COVID-19 classification using 70 chest radiographic images of patients with COVID-19, obtained from an online COVID-19 dataset, and images of patients without COVID-19 obtained from Kaggle’s Pneumonia Chest X-Ray Challenge Ghoshal B, Tucker A. Estimating uncertainty and interpretability in deep learning for coronavirus (COVID-19) detection. arXiv website. arxiv.org/abs/2003.10769. Published Mar 22, 2020. Updated Mar 27, 2020. Accessed May 7, 2020. This study showed heat maps to visualize the locations used by the network to classify COVID-19-related pneumonia, increasing the transparency of the AI process, and they obtained a 92.9% accuracy for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) detection.
From a recent review paper, the overall accuracy of AI-based radiographic algorithms for the classification of COVID-19-related pneumonia was pretty good, ranging between 83.5% and 98% Shi F, Wang J, Shi J, et al. Review of artificial intelligence techniques in imaging data acquisition, segmentation and diagnosis for COVID-19. IEEE Rev Biomed Eng 2020 Apr 16 [Epub ahead of print].
CT-Based AI Classification
Chest CT images are considered more sensitive for the visualization of COVID-19-related pulmonary manifestations. Several studies have described radiological chest CT patterns, characterizing different stages of the disease. Early signs of the disease are ground-glass nodules, especially subpleural in the lower lobes, which can be found both unilaterally and bilaterally. In the following stages, diffuse ground-glass nodules, “crazy-paving” pattern, and even consolidation can be found, often bilaterally in distribution encompassing multiple lobes Lee YP, Jin Y, Fangfang Y, et al. Imaging profile of the COVID-19 infection: radiologic findings and literature review. Radiology 2020 Feb 13 [Epub ahead of print]
Pan F, Ye T, Sun P, et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology 2020 Feb 13 [Epub ahead of print]
Bernheim A, Mei X, Huang M, et al. Chest CT findings in coronavirus disease-19 (COVID-19): relationship to duration of infection. Radiology 2020 Feb 20 [Epub ahead of print]. At the most severe stage, dense consolidations become more prevalent. At the recovery stage, consolidation patterns are gradually resolved, while GGOs are still present for a longer time.
Studies on the AI-based classification of COVID-19-related pulmonary manifestations on chest CT are more prevalent than the ones on radiographic images. One of the largest studies performed by Shi et al. Shi F, Xia L, Shan F, et al. Large-scale screening of COVID-19 from community acquired pneumonia using infection size-aware classification. arXiv website. arxiv.org/abs/2003.09860. Published Mar 22, 2020. Accessed May 7, 2020 used chest CT images of 2,685 patients, of which 1,658 patients tested positive for COVID-19, while 1,027 images represented patients with non-COVID-19-related pneumonia. A Size Aware Random Forest method (iSARF) was used to train the algorithm to not only classify the different pneumonia causes, but also segment the image to calculate the involved lung volume. With an accuracy of 87.9%, additionally, their results showed that small volumes have a lower sensitivity for detection. Another large study performed by Li et al. Li L, Qin L, Xu Z, et al. Artificial intelligence distinguishes COVID-19 from community acquired pneumonia on Chest CT. Radiology 2020 Mar 19 [Epub ahead of print] of 4,356 chest CT images (1,296 COVID-19, 1,735 community-acquired pneumonia, and 1,325 non-pneumonia) using a pre-trained deep convolutional network (ResNet50) showed an excellent accuracy rate of 96% for the classification of COVID-19-related pneumonia.
AI Prediction of Disease Severity and Progression
With increasing laboratory test availability for COVID-19 diagnosis, the focus of medical imaging is shifting to the assessment of disease severity and disease progression, which can be used for treatment planning optimization and treatment efficiency evaluation Pan F, Ye T, Sun P, et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology 2020 Feb 13 [Epub ahead of print]
Bernheim A, Mei X, Huang M, et al. Chest CT findings in coronavirus disease-19 (COVID-19): relationship to duration of infection. Radiology 2020 Feb 20 [Epub ahead of print]
Zhao W, Zhong Z, Xie X, Yu Q, Liu J. Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: a multicenter study. AJR 2020 Feb 19 [Epub ahead of print]
Li K, Wu J, Wu F, et al. The clinical and chest CT features associated with severe and critical COVID-19 pneumonia. Invest Radiol 2020; 55:1
Li M, Lei P, Zeng B, et al. Coronavirus disease (COVID-19): spectrum of CT findings and temporal progression of the disease. Acad Radiol 2020; 27:603-608. Specific manifestations and affected lung volumes can be used as an indication of disease severity. Tang et al. Tang Z, Zhao W, Xie X, et al. (2020) Severity assessment of coronavirus disease 2019 (COVID-19) using quantitative features from chest CT images. arXiv website. arxiv.org/abs/2003.11988. Published Mar 26, 2020. Accessed May 7, 2020 proposed a random forest model to quantify disease severity using chest CT images of 176 patients with confirmed COVID-19. They reported an accuracy of 87.5% with 0.91 AUC. More interestingly, they showed that specific quantitative features, such as the volume of GGO and its ratio with respect to the whole lung volume, are good indicators of the severity of COVID-19.
A study by Huang et al. Huang L, Han R, Ai T, et al. Serial quantitative chest CT assessment of COVID-19: deep-learning approach. Radiol Cardiothorac Imaging 2020 Mar 30 [Epub ahead of print] used a deep learning algorithm to automatically quantify CT lung opacification percentage, evaluating longitudinal changes of these quantitative parameters in sequential examinations and taking into account the clinical parameters and disease severity. A total of 126 patients were included, representing mild (6), moderate (94), severe (20), and critical (6) cases. They showed that the opacification progression was mainly present between baseline and first follow up, but not in later stages, and they observed that the opacification percentage increased with worsening disease severity.
Emory AI Project: The PREDICTION Study
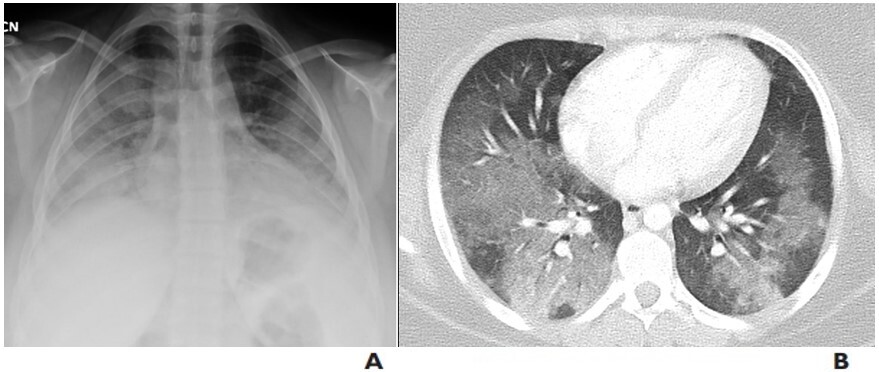
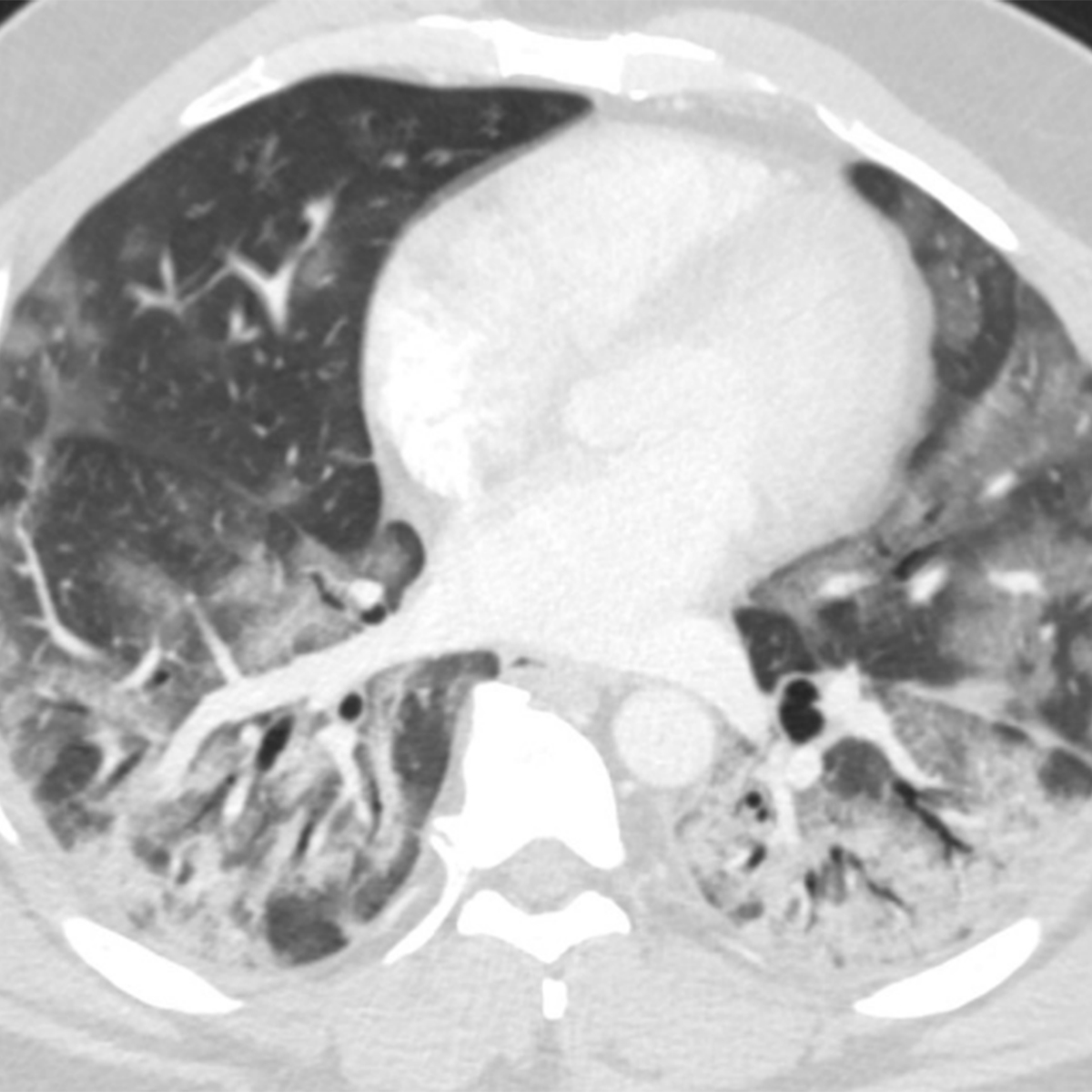
At Emory University, in collaboration with the Georgia Institute of Technology, we have started an AI project on COVID-19, entitled “Predictive Model of COVID-19 Outcome Using a Convolutional Neural Network Applied to Chest Imaging and Clinical Parameters: Early Detection and Prognostication for Optimal Resource Allocation (COVID-19 PREDICTION Study)” (Fig. 1).
We have two objectives:
Use supervised learning methods to build a predictive model that can distinguish COVID-19 pneumonia from other common lung pathologies using chest imaging and clinical parameters.
Monitor the disease progression over time detecting different evolution patterns, ideally finding imaging and clinical parameters that can predict the evolution to the most severe cases of COVID-19, which result in intensive care unit admission and the need for respiratory assistance.
With this project, we hope that an AI-powered solution for COVID-19 early detection and prognostication will have a major impact on patient outcome and optimization of the resource allocation, in particular in areas with limited medical resources and access to ventilators.
Fig. 1—Chest radiographic (A) and CT (B) images utilized for training the AI algorithm at Emory University.
Future Developments and Perspective
In the near future, more AI-based solutions will be developed and applied for the evaluation of COVID-19 using medical imaging. Whereas the first AI approaches were mostly focused on COVID-19 diagnosis, we now see more algorithms focusing on disease severity and progression quantification. The first step for the development and training of these AI algorithms is the creation of large, representative databases, followed by proper algorithm validation. At the moment, there are several worldwide initiatives for the creation of open-source databases for both radiographic and chest CT images Zhao J, Zhang Y, He X, Xie P. COVID-CT-dataset: a CT scan dataset about COVID-19. arXiv website. arxiv.org/abs/2003.13865. Published Mar 30, 2020. Accessed May 7, 2020
Cohen JP, Morrison P, Dao L. COVID-19 Image Data Collection. arXiv website. arxiv.org/abs/2003.11597. Published Mar 25, 2020. Accessed May 7, 2020. Recently, the Radiology Society for North America announced a call to develop an open-data repository for international COVID-19 imaging research and education efforts. Creating open-source databases and sharing AI algorithms online offer powerful tools for clinical validation. In the long term, we expect that AI will also play a role in the follow-up of COVID-19, predicting which patients will have permanent damage and assessing the disease evolution.
The COVID-19 pandemic presents an exceptional challenge for the international health care community. The social impact has been dramatic and will be lasting. Although no country was fully prepared at the beginning of this pandemic, we can now use the lessons learned—together with the large volume of generated clinical data and developing AI techniques—to prepare more efficient global response strategies.
Senior Faculty, Icahn School of Medicine Mount Sinai Hospital
Leonie Gordon
Vice Chair of Education Professor of Radiology and Nuclear Medicine Medical University of South Carolina
Don C. Yoo
Professor of Diagnostic Imaging, Clinician Educator, Warren Alpert Medical School of Brown University Director of Nuclear Medicine, Miriam Hospital
Esma Akin
Associate Professor of Radiology, Chief of Division of Nuclear Medicine George Washington University Medical Center
Katherine Zukotynski
Departments of Medicine and Radiology McMaster University
Published March 23, 2020
Theranostics is an exciting, emerging field where imaging and therapy are intimately tied together, as the same chemical molecule is used for imaging and therapy with a different radionuclide. Theranostics is a relatively new word, but radioiodine ablation with Iodine-131 (I-131) for imaging and treatment of thyroid cancer is one of the earliest examples of theranostics. Although radioactive iodine (RAI) has been used in clinical practice since the second world war, advances in imaging, therapeutic agents, and our understanding of the molecular basis of disease has slowly led to change. Developing a standardized approach to the management of thyroid cancer has been challenging and controversial. The American Thyroid Association (ATA) and the National Comprehensive Cancer Network (NCCN) guidelines for the management of thyroid cancer have undergone several iterations, some of which have been controversial, as conclusive data on the use of imaging and management strategies is often limited. Recently, however, discussion has led to the publication of the Martinique principles—setting the stage for increased interdisciplinary communication in an attempt to establish a set of recommendations based on the existing data and our wealth of accumulated experience.
Today, when a patient is diagnosed with thyroid cancer, they are assessed clinically and stratified as low, intermediate, or high risk. This is commonly done using the ATA or NCCN risk stratification system for recurrence, and the American Joint Committee on Cancer staging system predictions for long-term outcomes. Based on the risk stratification, a management plan is devised. Often, this includes pre-therapy imaging, therapy, and post-therapy imaging. There is a host of imaging that may be performed before and after therapy. Most commonly, ultrasound, CT, and planar imaging using RAI are performed with a gamma camera; however, SPECT and SPECT combined with CT may improve the sensitivity and specificity for the detection of disease compared with planar imaging alone. PET either with CT or MRI has a role for patients suspected of having thyroid cancer recurrence with rising thyroglobulin and negative diagnostic thyroid scans. There are several radioactive agents to choose from for imaging purposes. Although I-131 is typically less expensive and may be used for both imaging and therapy, Iodine-123 (I-123) has better imaging characteristics and is often used for diagnostic scans, especially in low- or intermediate-risk patients; however, I-123 cannot be used for therapy. Additionally, I-124 (although not routinely clinically used) and 18F-FDG may be helpful in certain situations, but they require access to PET.
ARRS Quick Bytes is a member-exclusive benefit that provides 20-minute videos on emerging topics in radiology for CME on the go.
There are several controversies regarding imaging and therapy of patients with thyroid cancer. For example, there is significant debate about the need for imaging before and after therapy using radioactive iodine vs other modalities, such as ultrasound and CT. Also, whereas RAI therapy has been a mainstay in thyroid cancer treatment for years, there have been recent changes in how this therapy is done. Historically, the amount of RAI to give for the purposes of therapy was based on disease extent, so those patients with distant metastases received a higher empiric amount of RAI than those with localized disease. Furthermore, pediatric patients were treated similarly to adults. Recently, however, we have tried to lower the amount of RAI administered based on the patient’s risk stratification and age to improve long term outcome and minimize radiation exposure, where possible. There is also a recognition that pediatric patients have some different clinical issues; thus, their approach to RAI has some key differences compared to adults.
While the use of and approach to theranostics in thyroid cancer is evolving, a few constants remain. Specifi cally, the experience and expertise of the multidisciplinary care team, as well as the desires of the patient, all need to be considered when making decisions about how to proceed. Imagers must recognize which information they can glean from their scans will best assist in determining the optimal course for treatment. When deciding on therapy, the amount and type of therapy to be given is based not only on pathology, but also on the medical team and patient’s wishes for short- and long-term follow up. Ultimately, as physicians who are intimately involved with both imaging and therapy, our insight can offer a lot to the overall care of the patient with thyroid cancer.