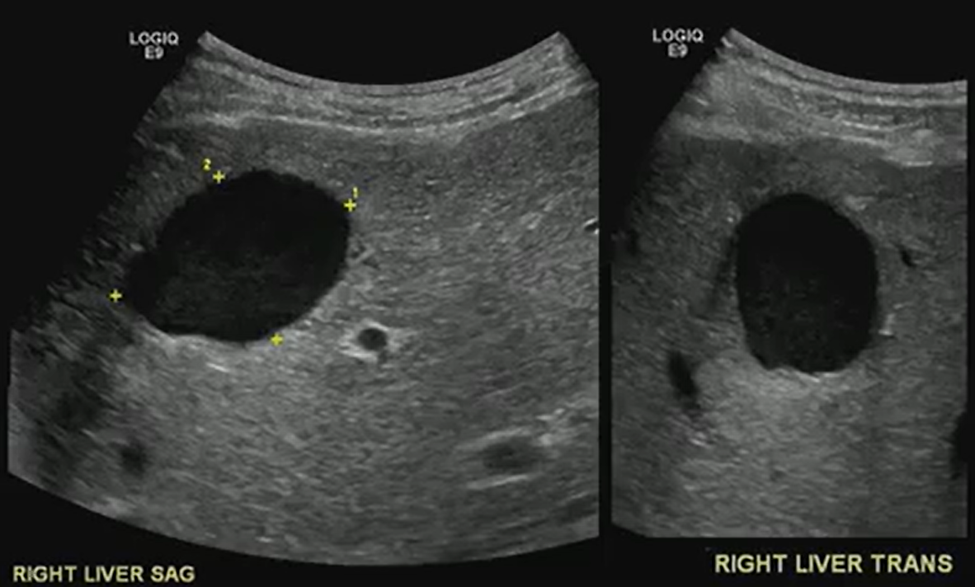
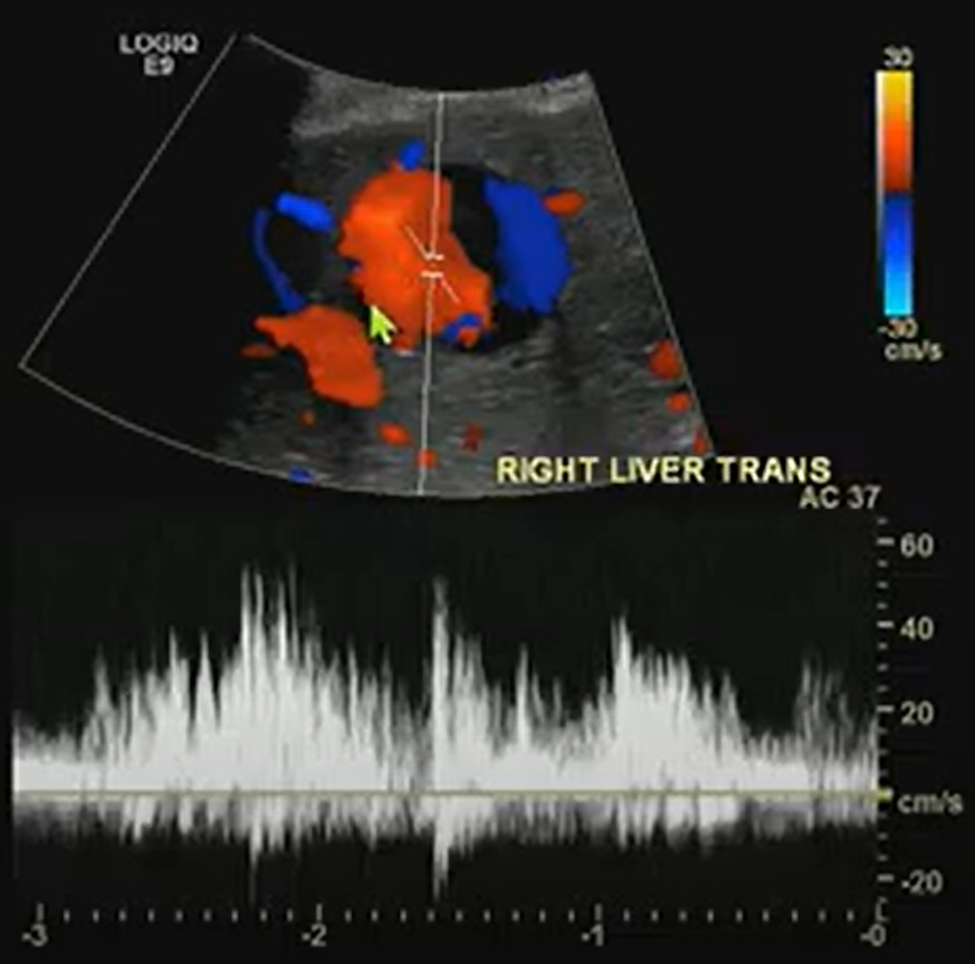
A benign-looking liver lesion turned out to be a hepatic artery pseudoaneurysm—all thanks to color Doppler.
The Big Picture
What looks like a simple hypoechoic cyst on ultrasound may hide a critical vascular pathology. In this ARRS Annual Meeting case from Kristin Rebik, DO, color Doppler proved essential for distinguishing cystic lesions from vascular anomalies like pseudoaneurysms.
Key Takeaways
Always Doppler: Even cyst-like structures require Doppler evaluation to rule out vascular causes.
Pepsi Sign: Swirling vascular flow within a lesion may signal a pseudoaneurysm.
High stakes: Hepatic artery pseudoaneurysms can mimic benign lesions but require urgent recognition and intervention.
Next steps: Interventional radiology embolization can be lifesaving.
Challenges Ahead
Differentiating pseudoaneurysms from other vascular or cystic lesions remains tricky.
Missing Doppler evaluation risks misdiagnosis and delayed treatment.
Awareness of teaching signs like the “Pepsi sign” is uneven among trainees.
Bottom Line
Never skip Doppler. The “Pepsi sign” may be the clue that transforms a benign-looking lesion into a critical vascular diagnosis.
When it comes to the cervical spine, cord integrity matters most. Even mild changes can spell trouble if the cord is compromised.
Big Picture: Cervical canal stenosis isn’t just about the degree of narrowing; it’s about whether the spinal cord, itself, is at risk, too. Even without measurable stenosis, cord flattening can cause myelopathy. Understanding Dr. Lea Alhilali’s fishbowl analogy from the ARRS Neuroradiology Longitudinal Course helps clarify how to distinguish mild, moderate, and severe cases.
Key Takeaways:
Cord first: Regardless of canal narrowing, deformity or signal changes in the cord point to a higher risk of myelopathy.
Not just static: Static imaging may underestimate the impact; dynamic forces, repetitive microtrauma, or microischemia may drive symptoms.
“Fishy” Analogies…
Mild stenosis: Either ventral or dorsal CSF is effaced, but the cord still has room to “swim.”
Moderate stenosis: Both ventral and dorsal CSF are lost, restricting cord movement.
Severe stenosis: No CSF remains—cord is compressed, “fish” crushed.
Challenges Ahead
Why cord flattening causes myelopathy without stenosis remains unclear, and mechanisms are still debated.
Dynamic assessment may offer better insight than static MRI but isn’t standardized.
Management depends on correlating imaging with clinical findings, which are often nuanced.
Bottom Line: Think of the cervical cord like a fish in a bowl: it needs space to move. Once the CSF “water” is gone, the cord, as well as the patient, suffers. Classifying stenosis by available space—not merely narrowing—sharpens diagnostic accuracy and clinical relevance.
Since its introduction nearly 20 years ago, score-based peer review has not been shown to have a meaningful impact on or be an accurate measurement of radiologist performance [1]. A new paradigm—peer learning—has emerged, which is a group activity where practicing professionals review each other’s work, actively give and receive feedback in a constructive manner, teach and learn from one another, and mutually commit to improving performance as individuals and as a group. As my colleague, coauthor, and present chair of ARRS’ Professional & Performance Improvement Committee, Nadja Kadom, MD, first noted here in the pages of InPractice back in 2019, peer learning is “a system that uses accuracy of interpretation as a surrogate marker for competency” [2].
Many radiology practices are beginning to transition from score-based peer review to peer learning, but these same practices face distinct challenges and multiple barriers to implementation, especially considering the variety of leadership styles Dr. Kadom has recently detailed [3]. Case in point: nearly half of the 742 members of ARRS who participated in our 2020 AJR Original Research article, “Current Status and Future Wish List of Peer Review: A National Questionnaire of U.S. Radiologists,” reported insufficient learning outcomes from peer review [4]. Clarifying a minimum number of cases that required monthly review, as well as how interpretive discrepancies would be communicated, were two big factors where some level of standardization was clearly needed.
Perhaps most importantly, the demographics of our survey respondents reflected the current composition of this country’s imaging workforce. A total 742 (4.2% response rate) ARRS members replied to our 21-question, multiple-choice questionnaire. Among those respondents, 547 (73.7%) were board-certified, practicing radiologists also participating in a form of peer review. As you can see, most responders were in private practice (51.7%, 283/547), while the next largest cohort was in academic practice (32.4%). The most common practice size was 11–50 radiologists (50.5%), followed by groups of up to 10 radiologists (21.2%). The majority of responders practiced in urban settings (61.6%), too.
Practice Characteristic
No. (%)
Type
Private
283 (51.7)
Academica
177 (32.4)
Hybridb
45 (8.2)
Government
42 (7.7)
No. of radiologists
0–10
116 (21.2)
11–50
276 (50.5)
51–100
85 (15.5)
>100
70 (12.8)
Setting
Urban
337 (61.6)
Suburban
158 (28.9)
Rural
52 (9.5)
aAcademic practices had medical school and radiology residency program. bHybrid practices had radiology residency program without a medical school.
Nonetheless, in this largest nationwide questionnaire to imaging professionals regarding the present state of and their future needs for peer review, most radiologists working in the United States felt a better system is not only necessary, but that said system could even be feasible in daily practice.
To our knowledge, “Updates for Your Peer Learning Activities: Pitfalls, Tips, and Accreditations” remains the only course of its kind. Presented live as a Featured Sunday Session during the 2023 ARRS Annual Meeting in Honolulu, HI, this course is now in its second revised and expanded iteration, packed with practical tips to clinical success, all taught by experts in the field. Summarizing the current status and practice gap in peer review in radiology, sessions will include three didactic lectures to showcase the best practices and challenges of peer learning programs at multiple institutions, including Emory, NYU, Stanford and Mayo Clinic. Esteemed faculty will highlight potential barriers to starting and sustaining peer learning activities in both academic and private practice settings, each instructor sharing their own “top 5 tips” for overcome these challenges. We will also address the latest updates from the American College of Radiology’s Quality and Safety Commission regarding new accreditation pathways for peer learning [5].
The evolution of peer learning is of universal importance for the continuing education of all radiologists—in practice, during fellowship or residency. However, the intersecting concepts of peer learning, just culture, etc. are evolving at a breakneck pace, with brand-new accreditation pathways opening up and multiple acceptable approaches to finding the “right answer” [6]. For imaging professionals already involved in peer learning, come share your experience with our expert panel, ensuring you are getting the most out of your program. For those new to peer learning, come learn how to fish for the pearls, avoid the pitfalls, and hit the ground running. We will conclude with an interactive panel discussion with the audience—there in Hawaii, virtually, or on demand.
References
Larson DB et al. Transitioning from peer review to peer learning: report of the 2020 Peer Learning Summit. J Am Coll Radiol 2020; 17:1499–1508
@OWeaverMD Department of Breast Imaging, Division of Diagnostic Imaging MD Anderson Cancer Center
Contrast-enhanced mammography (CEM) is a relatively new modality which is rapidly gaining acceptance in breast imaging. Many medical centers have already acquired the necessary equipment to implement CEM programs [1], thus creating an ever-increasing demand for trusted CEM educational resources.
At the same time, however, there remains a paucity of quality instructional materials for this emerging tool, a lack of structured, case-based training, and fundamental misconceptions regarding both the technical aspects and the operational/administrative knowledge needed for successful implementation of CEM.
On day one of the 2023 ARRS Annual Meeting, Sunday, April 16, live (and virtually, of course) from Honolulu on the enchanting island of Oahu, HI, Drs. Wendie Berg, Bhavika Patel, and I, will offer a two-hour introductory program on practical CEM for radiologists. Our Featured Sunday Session, “Contrast-Enhanced Mammography: The Essentials and Beyond,” will include interactive didactic and case-based lectures to educate and update practicing radiologists on the important foundational principles of CEM. The course will be supplemented with an optional short pre- and post-test survey to help the audience organize the information and evaluate their learning progress.
CEM Augments Mammography Capabilities in the Digital Era
The strength of CEM is its ability to provide both morphologic information on low-energy images, similar to a standard 2D mammogram, and functional information of contrast distribution on the “recombined” (subtracted and processed) images. This is achieved by software and hardware modifications to modern mammographic equipment and necessitates patient workflow adjustments in breast centers [2]. The course will present the basics of CEM technology, its strengths and limitations, as well as helpful tips on implementing this modality in clinical practice.
Additionally, the course will serve as a guide to CEM image interpretation with a special emphasis on utilization of the newly introduced Breast Imaging Reporting & Data System (BI-RADS®) CEM lexicon [3].
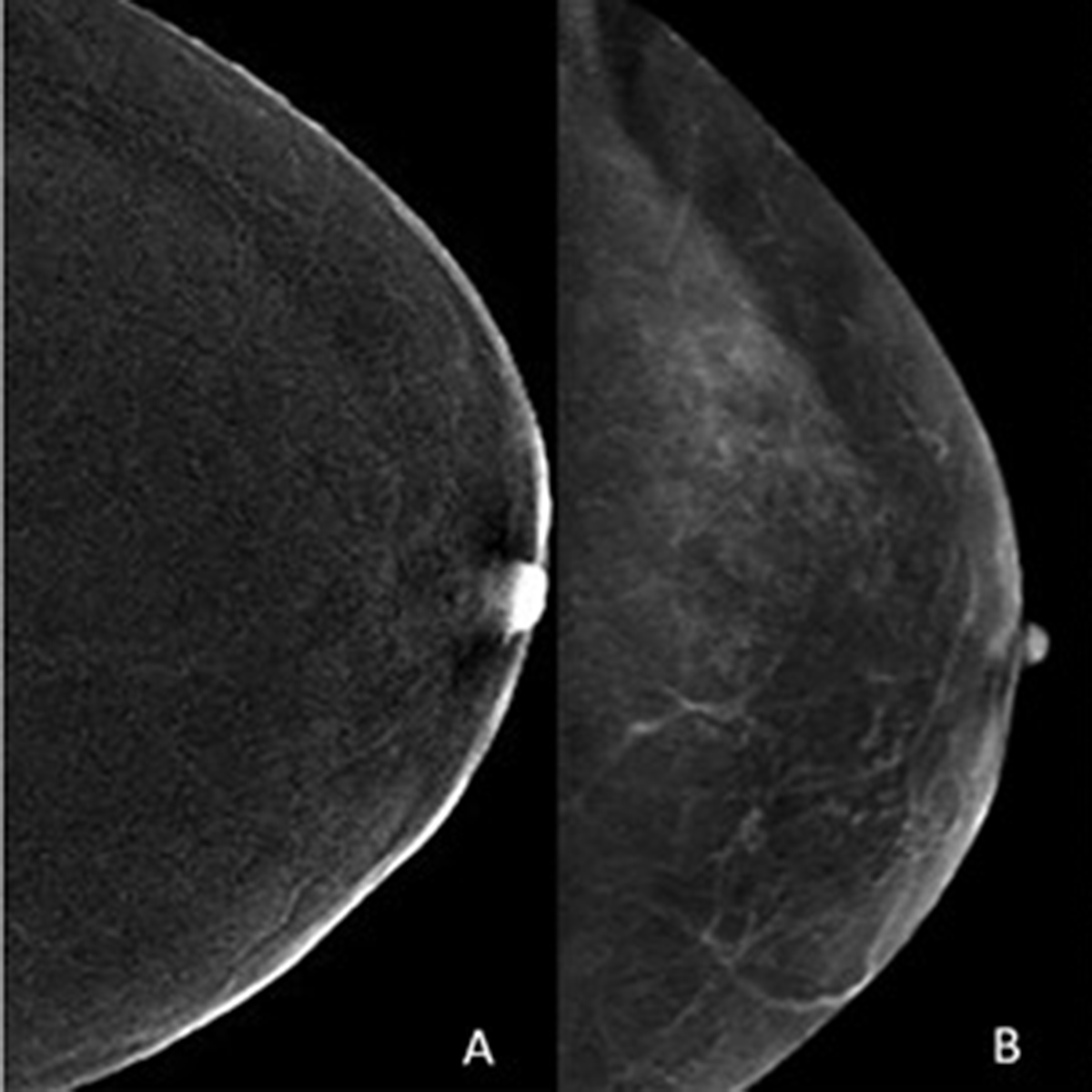
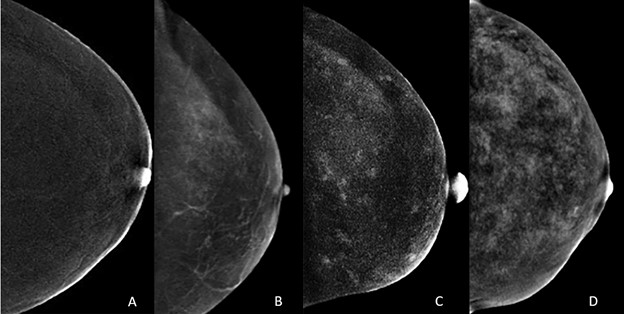
We will also discuss background parenchymal enhancement (BPE) in CEM image interpretation. Similar to breast tissue density of mammography, increased BPE may both mask and mimic cancer on CEM. As on MRI, there are four categories of BPE (Fig. 1), and multiple factors are associated with increased BPE [4]. We will present the audience with a range of appearances for normal BPE on CEM.
Fig. 1—Normal craniocaudal views of recombined images from CEM examination of four patients show different patterns of BPE: minimal (A), mild (B), moderate (C), and marked (D). All enhancement on images caused by normal BPE [4].
Drs. Berg, Patel, and myself will provide a case-based introduction to the most common artifacts and cancer mimics on CEM, too. This topic is continuously evolving. In the July issue of AJR, enhancing cherry hemangioma has been described as a common benign finding that may be misleading (Fig. 2) [5]. It is helpful for the technologist to make note of skin lesions, which can be marked to facilitate recognition.
Fig. 2—52-year-old woman with dense breasts and family history of breast cancer (estimated lifetime risk, 20.4% by Tyrer-Cuzick model version 8) undergoing high-risk screening CEM. 1A: Right craniocaudal (left) and mediolateral oblique (right) CEM obtained 2.5 minutes after IV injection of 125 mL of iopamidol (Isovue 370, Bracco) show superficial 3-mm focus (circle) with medium enhancement in superior aspect of breast approximately 5 cm from nipple. 1B: Clinical photograph shows 3-mm cherry hemangioma (circle) on skin of right breast at 10-o’clock position approximately 5 cm from nipple found clinically by radiologist performing ultrasound. Finding corresponds to enhancing focus in A [5].
CEM Screening and Diagnostic Applications
Chief among the topics discussed will be the role of CEM, alongside other legacy modalities, in today’s screening and diagnostic guidelines and society-endorsed consensus recommendations for breast cancer imaging. CEM is already recommended as an alternative to MRI in screening of women at high risk of breast cancer and in average-risk women with dense breasts [6]. An AJR article from 2021 demonstrated that CEM shows promise as a breast cancer screening examination in patients with a personal history of lobular neoplasia [7].
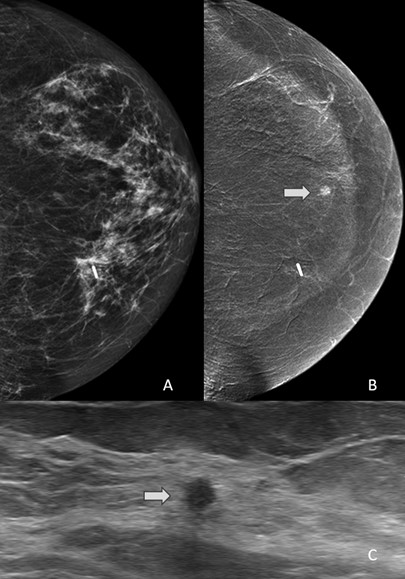
Of clinical importance is the fact that enhancing CEM-detected lesions that have an ultrasound correlate are more likely to be malignant. These data were also published by AJR in 2021 [8]. Among 153 enhancing lesions detected on CEM in 144 patients, the authors found ultrasound correlates in 47 (31%). Furthermore, this means that a substantial number of enhancing findings can potentially be sampled with ultrasound-guided biopsy (Fig. 3).
Fig. 3—57-year-old woman with history of left breast excision for lobular carcinoma in situ who underwent CEM. A: Low-energy mammogram shows no abnormality. B: Recombined mammogram shows enhancing 0.4-cm mass in 6-o’clock axis of left breast (arrow). Mass was evident only on recombined images. C: Image obtained during targeted ultrasound-guided core biopsy shows ultrasound correlate (arrow). Pathology result was invasive lobular carcinoma [8].
Diagnostic applications of CEM in breast imaging continue to evolve. In the July issue of AJR, CEM was compared with MRI for neoadjuvant therapy (NAT) response assessment [9, 10]. After NAT for breast cancer, CEM and MRI yielded similar assessments of lesion size (both slightly overestimated vs. pathology) and RECIST categories, and no significant difference in specificity for complete pathologic response. Duly noting that MRI had higher sensitivity for complete pathologic response, Bernardi et al. showed preliminary data suggesting that a delayed CEM acquisition 6 minutes after contrast injection could help detect residual ductal carcinoma in situ (DCIS) [10]. The authors concluded that while MRI remains the preferred test for NAT monitoring, the findings support CEM as a useful alternative when MRI is contraindicated or not tolerated [10, 11].
CEM may be a useful alternative to MRI in women with newly diagnosed breast cancer and breast augmentation. The findings of Carnahan et al. published in AJR last year suggest the plausibility of CEM for disease extent assessment in women with breast augmentation and contraindication or limited access to MRI [12].
The study evaluated 17 female breast cancer patients with breast implant augmentation, who underwent both CEM and MRI for staging. CEM and MRI were concordant for the index cancer in all 17 women. Six additional lesions were demonstrated by CEM and confirmed by MRI in 6 (35%) women: three multifocal, one multicentric, and two contralateral; two (33%) were malignant (one each invasive ductal and invasive lobular carcinoma). MRI did not identify any additional cancers not seen on CEM.
CEM-Guided Biopsy
Perhaps the largest unmet need for expertly curated CEM education surrounds CEM-guided biopsy. Case in point: recently FDA-approved—but not yet widely available—direct CEM-guided biopsy is often a necessary step in patient management. In the absence of CEM-guided biopsy capability, suspicious enhancing findings that have no definite correlate on low energy images, tomosynthesis, or ultrasound require possible MRI-guided biopsy for diagnosis. This increases cost and prolongs diagnostic workup. With the introduction of CEM-guided biopsy technology, this workflow is expected to become more streamlined and efficient. Our subspecialized presenters have personal experience with this technology and will deliver a comprehensive overview of the current state of knowledge and the future directions of CEM-guided biopsies.
CEM Essentials—and Beyond—at the ARRS Annual Meeting
Contemporary breast imagers must become more familiar with the range of indications and contraindications on CEM, such as normal variants, BPE, pathology, and artifacts. Focused sessions will also address interpretative skills in CEM—including appropriate use of the recently released BI-RADS CEM lexicon from the American College of Radiology—giving radiologists in private and academic practices alike applied insights from real-life cases.
Although the target audience for our course is predominantly medical imaging professionals considering or actively implementing CEM in practice, the curriculum presented live on Sunday, April 16 will also be relevant and valuable for recent residency or fellowship graduates, particularly those transitioning to imaging practices with established CEM services.
As the field moves forward, medical centers with established CEM programs will inevitably need to educate an incoming imaging workforce and new trainees who have not experienced enough clinical exposure to this modality in their previous practices or training programs. Apropos, “Contrast-Enhanced Mammography: The Essentials and Beyond” will also offer participants a unique opportunity to test and evaluate a newly developed online teaching module for CEM, purposefully designed to train the radiologists of today and tomorrow in clinical implementation of CEM in their own practices.
Perry H, Phillips J, Dialani V, Slanetz PJ, Fein-Zachary VJ, Karimova EJ, et al. Contrast-Enhanced Mammography: A Systematic Guide to Interpretation and Reporting. AJR 2019; 212:222–223
Breast Imaging Reporting & Data System (BI-RADS®) Contrast Enhanced Mammography (CEM) Supplement. ACR website. www.acr.org/-/media/ACR/Files/RADS/BI-RADS/BIRADS_CEM_2022.pdf. Published 2022. Accessed September 12, 2022
Karimi Z, Phillips J, Slanetz P, Lotfi P, Dialani V, Karimova J, et al. Factors Associated With Background Parenchymal Enhancement on Contrast-Enhanced Mammography. AJR 2020; 216:340–348
Lu AH, Zuley ML, Berg WA. Enhancing Cherry Hemangioma: A Mimic for Breast Cancer on Contrast-Enhanced Mammography. American Journal of Roentgenology. 2022;219(1):160-1.
The ACR Appropriateness Criteria® American College of Radiology Appropriateness Criteria. Supplemental Breast Cancer Screening Based on Breast Density. ACR website. acsearch.acr.org/docs/3158166/Narrative. Published 2021. Accessed September 12, 2022.
Hogan MP, Amir T, Sevilimedu V, Sung J, Morris EA, Jochelson MS. Contrast-Enhanced Digital Mammography Screening for Intermediate-Risk Women With a History of Lobular Neoplasia. AJR 2021; 216:1486–1491
Coffey K, Sung J, Comstock C, Askin G, Jochelson MS, Morris EA, et al. Utility of Targeted Ultrasound to Predict Malignancy Among Lesions Detected on Contrast-Enhanced Digital Mammography. AJR 2021; 217:595–604
Woodard S. Editorial comment: evidence supporting contrast-enhanced mammography (CEM) for monitoring neoadjuvant chemotherapy response and showing the potential of delayed CEM. AJR 2022;11
Bernardi D. et al. Contrast-enhanced mammography versus MRI in the evaluation of neoadjuvant therapy response in patients with breast cancer: a prospective study. AJR 2022; 14:1–11
Carnahan MB et al. Contrast-enhanced mammography for newly diagnosed breast cancer in women with breast augmentation: preliminary findings. AJR 2021; 217:855–856
Division of Pediatric Neuroradiology Orlando Health—Arnold Palmer Hospital for Children
Avery Wright, DO
Division of Pediatric Neuro-Oncology Orlando Health—Arnold Palmer Hospital for Children
Mohit Agarwal, MD
Division of Neuroradiology Medical College of Wisconsin
Lily Wang, MBBS, MPH
Division of Neuroradiology University of Cincinnati Medical Center
Karen L. Salzman, MD
Division of Neuroradiology University of Utah Medical Center
Primary brain tumors are the most common solid tumors in children, second only to leukemia in terms of cancer incidence, and are the leading cause of childhood cancer-related mortality [1, 2]. Tumors may present across all pediatric age groups, including infants, children, adolescents, and young adults, with the majority of cases presenting in the first decade of life. Clinical presentations vary, based upon the type of tumor, location, and patient age; however, the most common presenting symptoms include headaches, nausea and vomiting, and gait abnormalities [3]. In infants and very young children, obstructive hydrocephalus results in macrocephaly with bulging fontanelle [4]. Brainstem tumors commonly have symptoms associated with involved tracts and cranial nerves.
Imaging plays a crucial role in the initial workup, management, and post-treatment follow-up of primary pediatric posterior fossa tumors. Treatment options vary, based upon the tumor type, location, and patient age, and are beyond the scope of this InPractice review. The most common primary posterior fossa tumors in children that we will discuss and illustrate during our 2023 ARRS Annual Meeting Categorical Course session include (in descending order of frequency): medulloblastoma, pilocytic astrocytoma, ependymoma, diffuse midline glioma, and atypical teratoid-rhabdoid tumor.
Medulloblastoma
Medulloblastomas are high-grade (WHO grade 4) embryonal tumors and represent the most common malignant and the most common primary posterior fossa brain tumors in children [5]. Various subcategories of medulloblastomas have been described and used in the past; however, the latest molecular classification lists the following subtypes: wingless/integrated (WNT)—activated, sonic hedgehog (SHH)—activated, and non-WNT/non-SHH (also known as groups 3 and group 4), with additional subcategories for SHH-activated and non-WNT/non-SHH variants [6]. Classically, medulloblastomas were thought of as midline cerebellar tumors, but certain subtypes have a propensity for off-midline presentations.
General Imaging Features
Imaging characteristics for the various subtypes of medulloblastoma are overall similar, reflecting that of densely packed, highly cellular tumors. Masses tend to be spherical in shape and displace adjacent structures, as opposed to the more pliable appearance of ependymomas. Increased density on CT and diffusion restriction on MRI are characteristic of medulloblastomas, reflective of their high cellularity. T2 signal intensity is variable, typically having areas of both increased and decreased T2 signal compared to cerebellar parenchyma. Small intralesional cysts are common, while intralesional hemorrhage and calcification are uncommon, though may occasionally be seen. Enhancement ranges from patchy to more robust solid enhancement [7, 8] (Fig. 1).
Fig. 1—8-year-old boy with progressive nighttime headache, nausea, vomiting. Surgical pathology confirmed medulloblastoma. Top, left to right: Axial CT image in brain window shows circumscribed hyperdense midline posterior fossa mass (black arrow) with dilatation of temporal horns of lateral ventricles secondary to obstructive hydrocephalus (white arrows); axial T2-weighted image shows mass (arrow) has signal intensity predominantly similar to gray matter, with additional small internal cystic components; axial T1-weighted postcontrast image shows avid enhancement of solid components of mass (arrow). Bottom, left and right: Characteristic restricted diffusion (arrows) is seen as increased signal intensity on DW image and decreased signal intensity on ADC map.
On MR spectroscopy, a high-grade tumoral spectrum is evident with increased choline and decreased N-acetyl aspartate peaks. A taurine peak just to the left of the choline peak may be a specific marker for medulloblastoma in the posterior fossa [9].
The frequency of metastatic disease varies depending upon the molecular subtype, ranging from approximately 10% to up to 45% at the time of initial presentation [5]. It is therefore important to image the spine prior to surgical resection and with subsequent surveillance imaging to evaluate for disseminated disease.
WNT-Activated Medulloblastoma
WNT-activated medulloblastomas are the least common subset and have the best overall prognosis. These tumors commonly present in older children and adolescents and may occur midline or laterally around the foramen of Luschka, cerebellar peduncle, and cerebellopontine angle [6, 7, 10].
SHH-Activated Medulloblastoma
SHH-activated medulloblastomas are a more heterogeneous subset than WNT-activated, with an overall intermediate prognosis. Tumors tend to be located laterally in the cerebellar hemispheres, since they are thought to arise from precursors in the external granule-cell layer of the cerebellum, but they may occur in the midline as well [6, 11]. There is a bimodal presentation, occurring most commonly in infants and then young adults, though they may also occur in children. The infantile variant tends to have extensive nodularity on histology and more frequently metastasizes [11, 12]. Nearly all nodular or desmoplastic variants fall into this category. SHH-activated medulloblastomas are stratified based on their TP53 status as either TP53-wildtype or TP53-mutant, with TP53-mutant portending a worse prognosis [6].
Non-WNT/Non-SHH Medulloblastoma, Groups 3 and 4
Non-WNT/non-SHH medulloblastomas are the most common molecular subsets, have an increased incidence in boys, present as midline vermian tumors, and often have classic or large cell anaplastic features on histology. Group 3 tumors tend to occur in infants and young children, have a higher incidence of metastases, and have the worst overall prognosis of any medulloblastoma tumor subset. Group 4 tumors are the most common subset, occur in older children and adolescents, and have an intermediate prognosis [6, 11]. In terms of distinguishing imaging features, group 3 tumors often have avid enhancement, while hypoenhancement is preferentially seen with group 4 tumors [13].
Pilocytic Astrocytoma
Pilocytic astrocytomas are the most common primary brain tumor in children, accounting for approximately one-third of all gliomas, and the second most common primary posterior fossa tumor in children after medulloblastomas. They are low-grade, WHO grade 1, tumors with an excellent prognosis in the setting of gross total surgical resection. Pilocytic astrocytomas result from MAPK pathway alterations, often with BRAF fusion or BRAF V600E point mutations. BRAF fusion is common in posterior fossa pilocytic astrocytomas and is associated with improved outcomes [14]. BRAF V600E point mutations, on the other hand, tend to be associated with poorer outcomes [15]. Increased frequency of pilocytic astrocytomas is seen in patients with neurofibromatosis type 1 (NF1), most commonly involving the optic pathways, though they may occur nearly anywhere with NF1 [16].
Posterior fossa pilocytic astrocytomas most often arise within the cerebellar hemispheres and are therefore lateral in location. Less commonly, they may be midline, arising from the cerebellar vermis. The classic imaging appearance is a large cystic mass with a peripheral solid nodule. More heterogeneous presentations, including a multicystic mass, predominantly solid mass with central cystic changes, or partially hemorrhagic mass, are less common [7, 17].
On MRI, the cystic component of the tumor is often similar to CSF signal intensity on T1 and T2 sequences, with the T2-FLAIR signal being more variable, based upon internal proteinaceous content. Solid portions of the mass avidly enhance, and there may also be enhancement along the margins of the cyst wall. A helpful distinguishing feature of a pilocytic astrocytoma, compared to other posterior fossa tumors, is the lack of diffusion restriction within the solid components of the tumor [18, 19] (Fig. 2).
Fig. 2—5-year-old boy with ataxia, nausea, vomiting. Surgical pathology revealed pilocytic astrocytoma. Left to right: Axial T2-weighted image shows off-midline cystic and solid posterior fossa mass (arrow) centered within left cerebellar hemisphere and subtle surrounding edema; coronal T1-weighted postcontrast image shows diffuse enhancement of peripheral solid nodular component of mass (arrow); axial DW shows no diffusion restriction.
Ependymoma
Ependymomas are the third most common primary posterior brain tumors, after medulloblastomas and pilocytic astrocytomas. The majority are classic, WHO grade 2, ependymomas, with more aggressive anaplastic ependymomas being WHO grade 3. Ependymomas are soft, pliable tumors that originate in or near the fourth ventricle and squeeze through the outlet foramina into adjacent spaces and cisterns. Because of their pliability, they often surround or encase neurovascular structures.
There are two subgroups of posterior fossa ependymomas: posterior fossa group A (PFA) and posterior fossa group B (PFB) [20]. PFA variants occur most often in infants, are lateral in location, and have a relatively poor prognosis. Because of the lateral location and common extension into the prepontine cistern, gross total resection is often difficult, and radiation therapy is typically avoided in infants because of the potential for morbidity. PFB variants occur in older children and adolescents, tend to arise from the floor of the fourth ventricle, and have a better overall prognosis than PFA variants [16, 21].
On MRI, ependymomas tend to be heterogeneously T2 hyperintense with variable enhancement. Cystic change and calcifications are common, with calcifications occurring in up to 50% of cases, much more common than is seen with medulloblastomas [7]. Given the relative pliability of the tumor, extension through fourth ventricular outlet foramina is characteristic. The presence of reduced or restricted diffusion is variable, but typically less than is seen with highly cellular medulloblastomas. The exception is with anaplastic ependymomas, which may have areas of restricted diffusion that are similar to medulloblastomas. Anaplastic ependymomas tend to have a higher frequency of disseminated metastatic disease and disease recurrence, with a poorer prognosis compared to lower-grade ependymomas [22]. The frequency of disseminated metastatic disease for ependymomas is less than that for medulloblastomas.
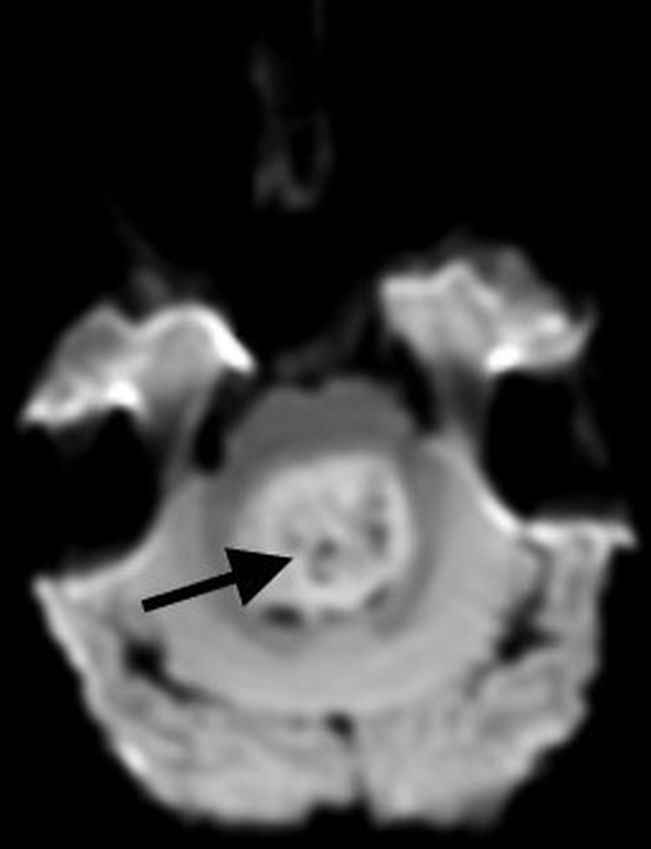
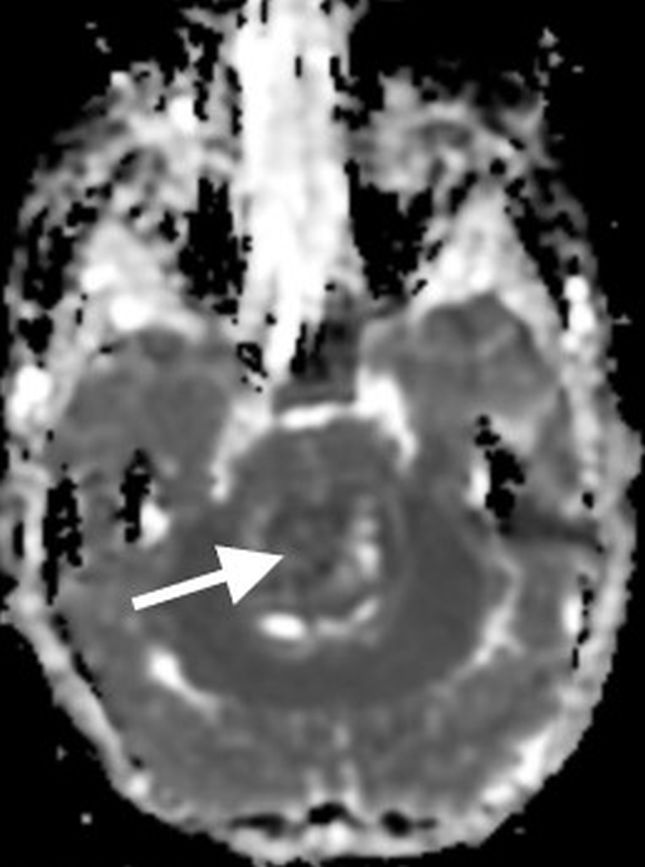
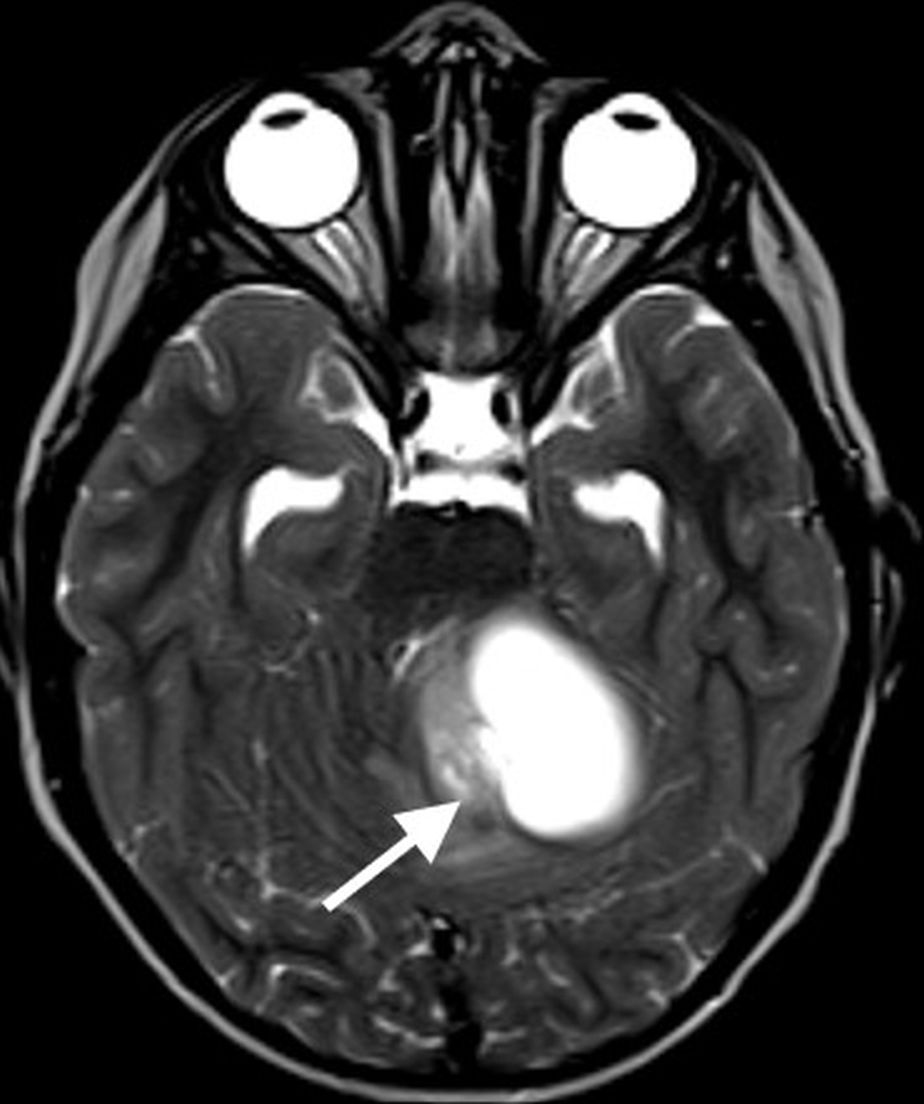
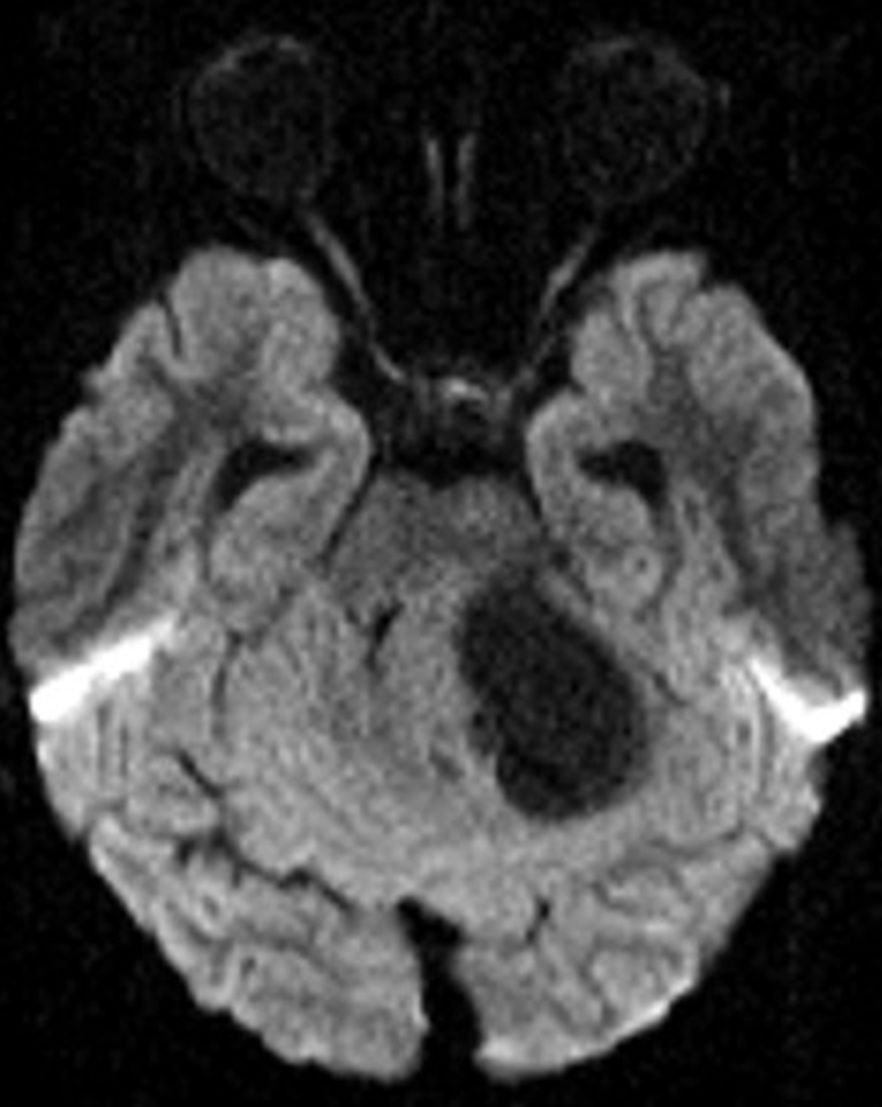
Diffuse Midline Glioma
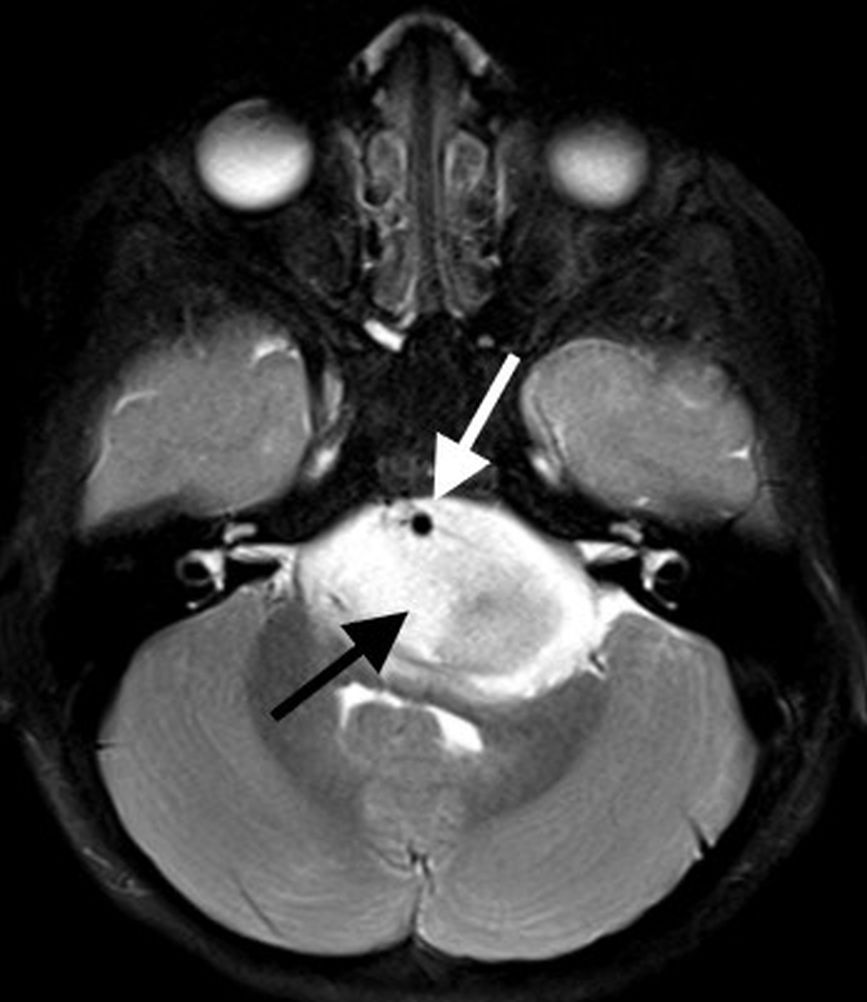
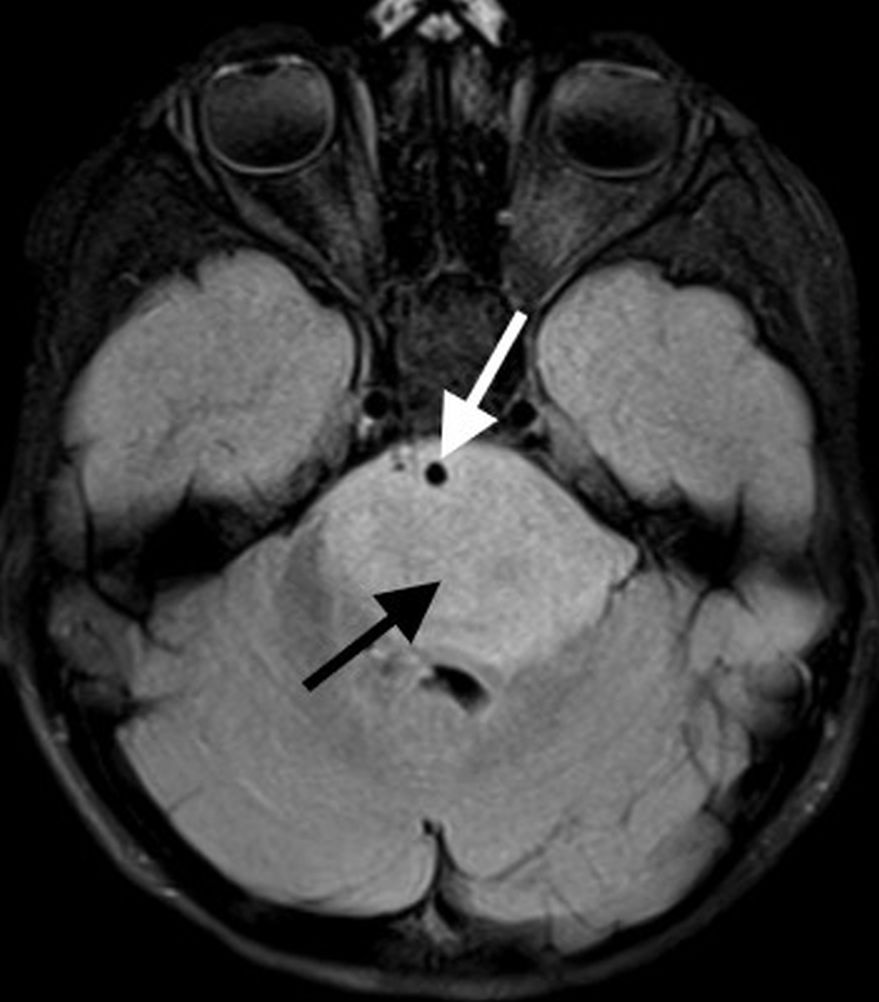
Diffuse midline gliomas (DMGs) “H3K27-altered” are highly aggressive pediatric brain tumors (WHO grade 4) that encompass the majority of lesions previously referred to as diffuse intrinsic pontine gliomas (DIPGs). Prognosis is dismal with a median survival of approximately 11 months from diagnosis [23]. Given the brainstem location, the most common clinical presentations include cranial nerve palsies, pyramidal tract signs (paresis, hyperreflexia, or positive Babinski reflex), and cerebellar signs (dysmetria, ataxia, dysarthria, or nystagmus) [23]. DMGs tend to occur in younger children, with median age at presentation around 6 years [24].
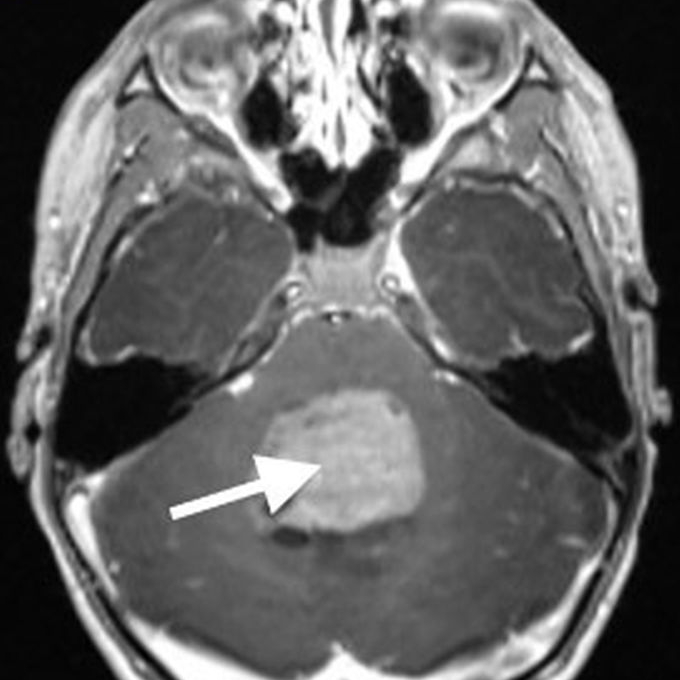
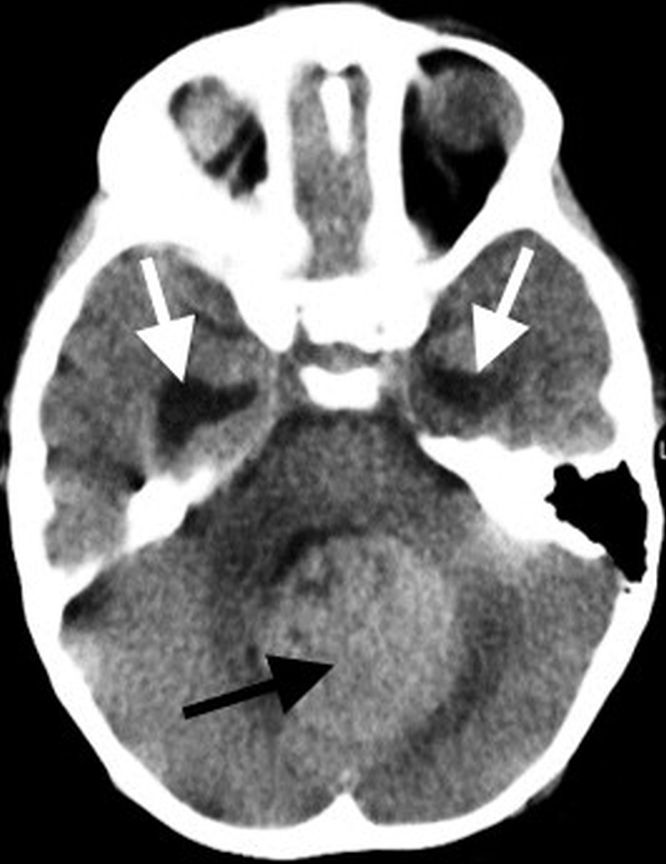
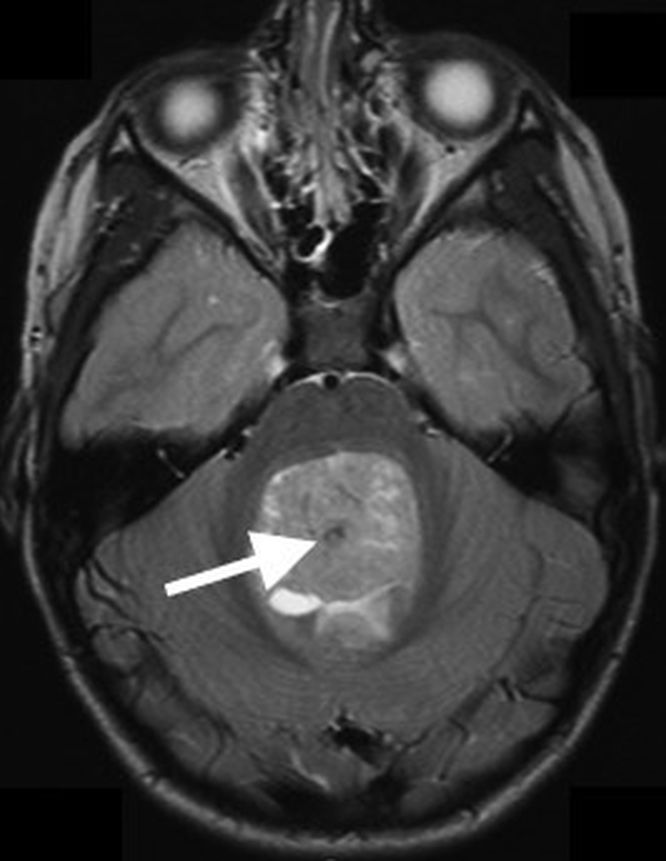
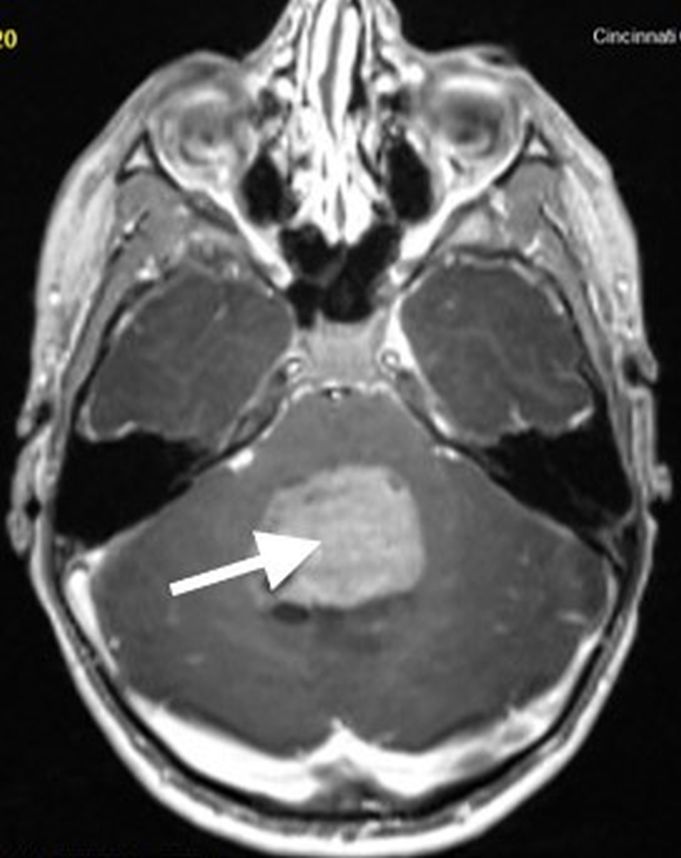
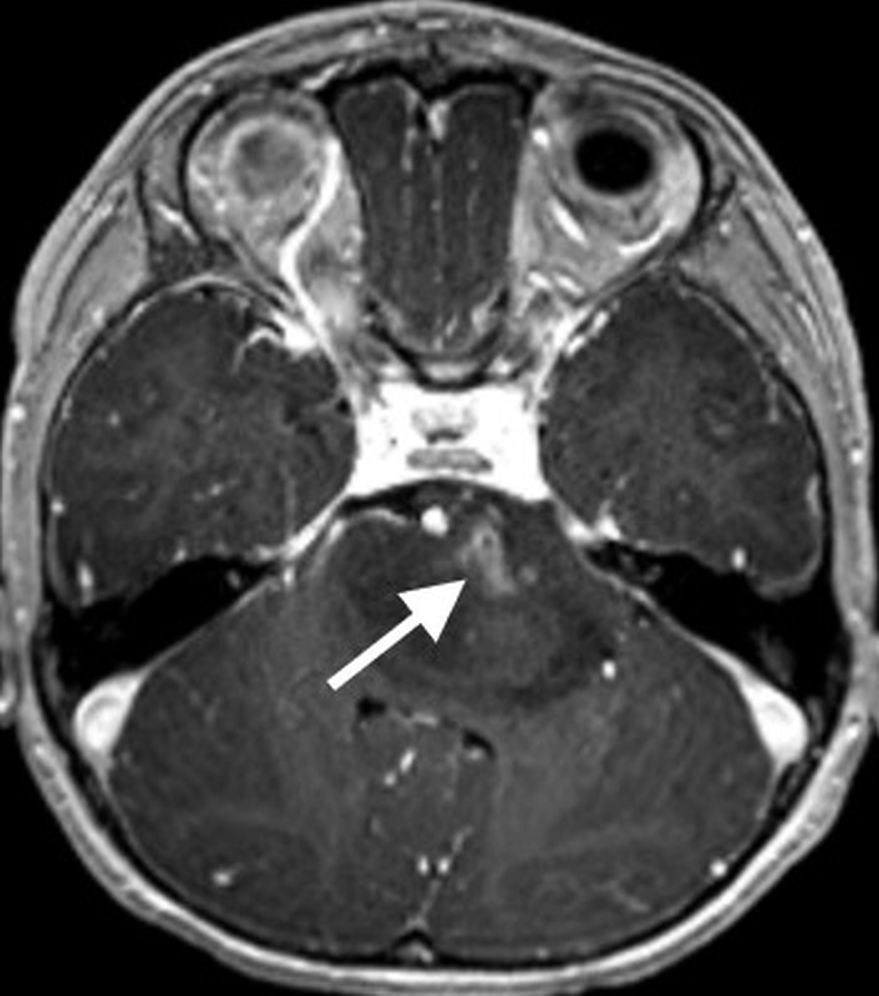
On MR imaging, DMGs present as a diffuse, ill-defined, T2 hyperintense, expansile masses centered within the pons. The degree of enhancement is variable, often absent at initial presentation and typically patchy when present (Fig. 3).
Fig. 3—7-year-old girl with ataxia, nystagmus, torticollis. Patient presumptively treated for DMG. Left and center: Axial T2-weighted and FLAIR images demonstrate infiltrative, expansile brainstem mass (black arrows) centered within pons and extending into brachium pontis on left. Exophytic components engulf basilar artery (white arrows) anteriorly and partially efface fourth ventricle posteriorly. Right: Axial T1-weighted postcontrast image shows mild patchy enhancement along ventral aspect of mass (arrow) on left.
Peripheral enhancement commonly occurs along margins of central necrosis, which occurs more frequently after radiation therapy [25]. Intralesional hemorrhage is uncommon, but areas of hemosiderin deposition may be seen on susceptibility-weighted sequences. Focal areas of restricted diffusion develop in the majority of cases. The presence of central necrosis, diffusion restriction, or enhancement at the time of initial diagnosis has been shown to portend a worse prognosis [24].
Extrapontine spread is common throughout the brainstem, into the thalami and adjacent structures, through the cerebellar peduncles, and into the cerebellar hemispheres. Exophytic components engulf the basilar artery anteriorly and efface the fourth ventricle posteriorly. Disseminated metastatic disease is uncommon, though may be seen occasionally.
Historically, DMGs have been treated presumptively when characteristic imaging features are present, reserving biopsy for cases with nonclassic imaging features or when tissue sampling is required for a clinical trial eligibility. However, more centers are now performing biopsies prior to treatment to confirm molecular classification and histology, shed light on potential prognosis, and help advance investigation of future adjuvant therapies. When biopsy is performed, the posterolateral portion of signal abnormality is typically targeted to minimize potential morbidity. If focal areas of diffusion restriction are present, these areas tend to have the highest diagnostic yield, if they can be safely accessed and sampled [26].
Atypical Teratoid-Rhabdoid Tumor
Atypical teratoid-rhabdoid tumors (ATRTs) are rare and highly aggressive (WHO grade 4) embryonal tumors that tend to occur in infants and young children, with the majority of cases presenting under 3 years of age. As with medulloblastomas, posterior fossa ATRTs may be midline or off-midline and are highly cellular with areas of diffusion restriction. Imaging features significantly overlap with medulloblastoma; therefore, patient age is one of the key features in suggesting ATRT versus medulloblastoma. Compared to medulloblastomas, ATRTs tends to have a more heterogeneous imaging appearance, with a higher incidence of intralesional hemorrhage and calcification, as well as a higher incidence of disease dissemination at the time of presentation [27, 28].
For most cases of primary posterior fossa tumors in children, the correct diagnosis can be suggested based upon distinguishing imaging features, with remaining cases requiring a thoughtful differential diagnosis in the setting of overlapping or nonspecific imaging findings. Our Categorical Course session will focus on recognizing characteristic imaging features for the most common primary pediatric posterior fossa tumors.
References
1. Pollack IF, Agnihotri S, Broniscer A. Childhood brain tumors: current management, biological insights, and future directions. J Neurosurg Pediatr 2019; 23:261–273
2. Pollack IF. Brain tumors in children. N Engl J Med 1994; 331:1500–1507
3. Prasad KSV, Ravi D, Pallikonda V, Raman BV. Clinicopathological study of pediatric posterior fossa tumors. J Pediatr Neurosci 2017; 12:245–250
4. Picariello S, Spennato P, Roth J, et al. Posterior fossa tumours in the first year of life: a two-centre retrospective study. Diagnostics (Basel) 2022; 12:1–12
6. Cohen AR. Brain tumors in children. N Engl J Med 2022; 386:1922–1931
7. Jaju A, Yeom KW, Ryan ME. MR imaging of pediatric brain tumors. Diagnostics (Basel) 2022; 12:1–24
8. Shih RY, Koeller KK. Embryonal tumors of the central nervous system. RadioGraphics 2018; 38:525–541
9. Panigrahy A, Krieger MD, Gonzalez-Gomez I, et al. Quantitative short echo time 1H-MR spectroscopy of untreated pediatric brain tumors: preoperative diagnosis and characterization. AJNR 2006; 27:560–572
10. Patay Z, DeSain LA, Hwang SN, et al. MR imaging characteristics of wingless-type-subgroup pediatric medulloblastoma. AJNR 2015; 36:2386–2393
11. Juraschka K, Taylor MD. Medulloblastoma in the age of molecular subgroups: a review. J Neurosurg Pediatr 2019; 24:353–363
12. Cavalli FMG, Remke M, Rampasek L, et al. Intertumoral heterogeneity within medulloblastoma subgroups. Cancer Cell 2017; 31:737–754.e6
13. Perreault S, Ramaswamy V, Achrol A, et al. MRI surrogates for molecular subgroups of medulloblastoma. AJNR 2014; 35:1263–1269
14. Becker AP, Scapulatempo-Neto C, Carloni AC, et al. KIAA1549: BRAF gene fusion and FGFR1 hotspot mutations are prognostic factors in pilocytic astrocytomas. J Neuropathol Exp Neurol 2015; 74:743–754
15. Nobre L, Zapotocky M, Ramaswamy V, et al. Outcomes of BRAF V600E pediatric gliomas treated with targeted BRAF inhibition. JCO Precis Oncol 2020; 4:561–571
16. AlRayahi J, Zapotocky M, Ramaswamy V, et al. Pediatric brain tumor genetics: what radiologists need to know. RadioGraphics 2018; 38:2102–2122
17. O’Brien WT. Imaging of Primary posterior fossa brain tumors in children. J Am Osteopath Coll Radiol 2013; 2:2–12
18. Novak J, Zarinabad N, Rose H, et al. Classifcation of paediatric brain tumours by diffusion weighted imaging and machine learning. Sci Rep 2021; 11:2987
19. Koral K, Alford R, Choudhury N, et al. Applicability of apparent diffusion coefficient ratios in preoperative diagnosis of common pediatric cerebellar tumors across two institutions. Neuroradiology 2014; 56:781–788
20. Louis DN, Perry A, Wesseling P, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol 2021; 23:1231–1251
21. Wu J, Armstrong TS, Gilbert MR. Biology and management of ependymomas. Neuro Oncol 2016; 18:902–913
22. Yuh EL, Barkovich AJ, Gupta N. Imaging of ependymomas: MRI and CT. Childs Nerv Syst 2009; 25:1203–1213
23. Hoffman LM, Veldhuijzen van Zanten SEM, Colditz N, et al. Clinical, radiologic, pathologic, and molecular characteristics of long-term survivors of diffuse intrinsic pontine glioma (DIPG): a collaborative report from the International and European Society for Pediatric Oncology DIPG Registries. J Clin Oncol 2018; 36:1963–1972
24. Leach JL, Roebker J, Schafer A, et al. MR imaging features of diffuse intrinsic pontine glioma and relationship to overall survival: Report from the International DIPG Registry. Neuro Oncol 2020; 22:1647–1657
25. Aboian MS, Solomon DA, Felton E, et al. Imaging characteristics of pediatric diffuse midline gliomas with histone H3 K27M mutation. AJNR 2017; 38:795–800
26. Biery MC, Noll A, Myers C, et al. A protocol for the generation of treatment-naïve biopsy-derived diffuse intrinsic pontine glioma and diffuse midline glioma models. J Exp Neurol 2020; 1:158–167
27. Arslanoglu A, Aygun N, Tekhtani D, et al. Imaging findings of CNS atypical teratoid/rhabdoid tumors. AJNR 2004; 25:476–480
28. Jin B, Feng XY. MRI features of atypical teratoid/rhabdoid tumors in children. Pediatr Radiol 2013; 43:1001–1008