
A benign-looking liver lesion turned out to be a hepatic artery pseudoaneurysm—all thanks to color Doppler.
The Big Picture
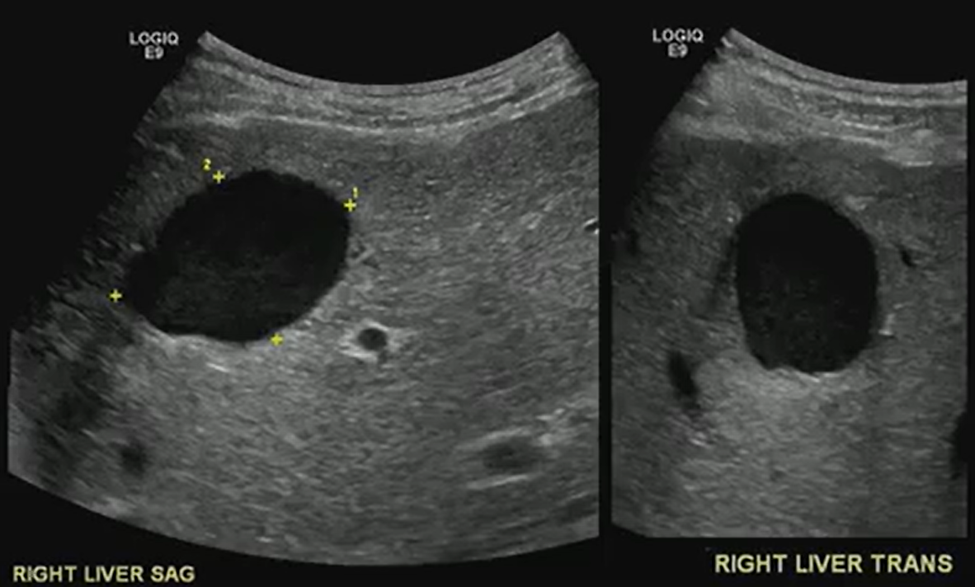
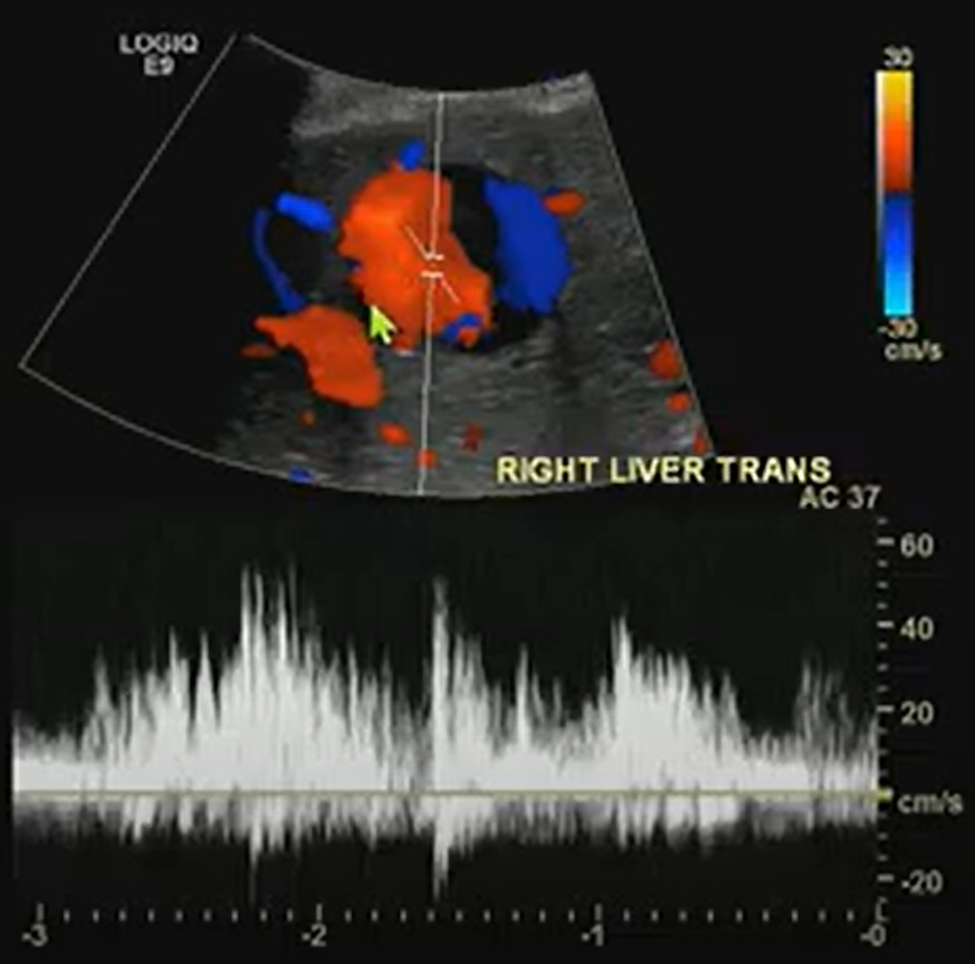
What looks like a simple hypoechoic cyst on ultrasound may hide a critical vascular pathology. In this ARRS Annual Meeting case from Kristin Rebik, DO, color Doppler proved essential for distinguishing cystic lesions from vascular anomalies like pseudoaneurysms.
Key Takeaways
- Always Doppler: Even cyst-like structures require Doppler evaluation to rule out vascular causes.
- Pepsi Sign: Swirling vascular flow within a lesion may signal a pseudoaneurysm.
- High stakes: Hepatic artery pseudoaneurysms can mimic benign lesions but require urgent recognition and intervention.
- Next steps: Interventional radiology embolization can be lifesaving.
Challenges Ahead
- Differentiating pseudoaneurysms from other vascular or cystic lesions remains tricky.
- Missing Doppler evaluation risks misdiagnosis and delayed treatment.
- Awareness of teaching signs like the “Pepsi sign” is uneven among trainees.
Bottom Line
Never skip Doppler. The “Pepsi sign” may be the clue that transforms a benign-looking lesion into a critical vascular diagnosis.
