-
Penile Prosthesis Imaging
As the prevalence of erectile dysfunction rises, so, too, do penile prostheses. For rads, accurately identifying normal device anatomy versus critical complications is essential for guiding patient care.
-

Better Billing: IR Tips for Reimbursement
In our declining reimbursement era, accurate documentation is really the only way to ensure your practice remains sustainable. Coders can only bill for what you, the rad, explicitly reports. And if it isn’t there, you aren’t getting paid for it.
-

BI-RADS v2025 Update: Glandular Tissue Component on Ultrasound
Ultimately, GTC transforms breast US from a tool used primarily for lesion characterization into a quantitative framework for personalized risk stratification vis-à-vis improved multidisciplinary communication.
-

Hepatic Vascular Trauma—Say What?
With DR basics forever in your own heart, do allow your head to consider alternatives—even, perhaps especially, in the middle of a trauma workup.
-
GLP-1s & FDG PET/CT: No Time for Adjustment
The Best Oral Presentation Abstract in Nuclear Medicine at ARRS 2026 indicates that these therapies do not significantly interfere with standard quantitative parameters.
-
Closing the Loop: Rads and Referring Physicians
By understanding the hospitalist’s workflow and providing clear, structured, and confident recommendations, rads provide a value-added benefit that directly improves patient outcomes.
-

Abdominal Fungal Infections: Malignant Mimics
Fungal granulomatous infections like histoplasmosis and coccidioidomycosis often masquerade as malignancy, making travel history and clinical context central to the DDx.
-

Insurance for Imagers—What You’ll Need (and What You Won’t!)
For rads, the goal is to balance the cost of premiums against the frequency and liability of potential risks.
-
Radiology’s Human-AI Equilibrium
Rads are always navigating two powerful psychological forces: automation bias (trusting AI too much because it’s quantitative) and algorithm aversion (dismissing AI in favor of human expertise).
-
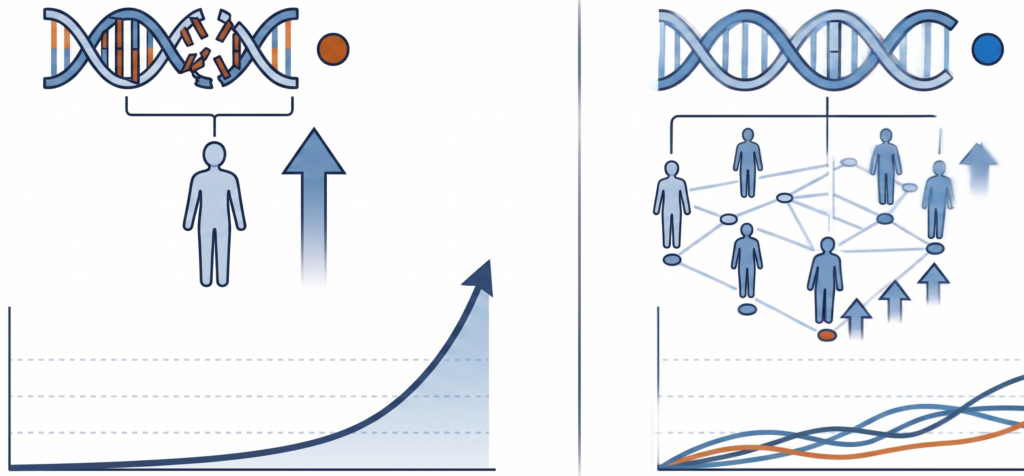
BRCA vs. SNP—Risk Evolution
Tis a true distinction between rare, high-risk hereditary mutation and much more common genetic variation.
