
Breast imaging during pregnancy demands heightened vigilance. Hormonal changes alter parenchymal appearance, masses can grow rapidly, and benign entities may closely mimic aggressive malignancies. Few examples illustrate this diagnostic tension better than the lactating adenoma, as Haydee Ojeda-Fournier, MD, explains during the ARRS Web Lecture “Breast Imaging: Special Patient Populations.”
Lactating adenomas are the second-most common mass encountered in pregnant and lactating patients. Imaging characteristics often mirror fibroadenomas and can be indistinguishable on both mammography and ultrasound. Therefore, definitive diagnosis typically depends on histology, rather than imaging alone.
These lesions are more frequently observed in the third trimester and often regress after delivery or once nursing begins—a reassuring natural history that supports conservative management when pathology confirms the diagnosis.
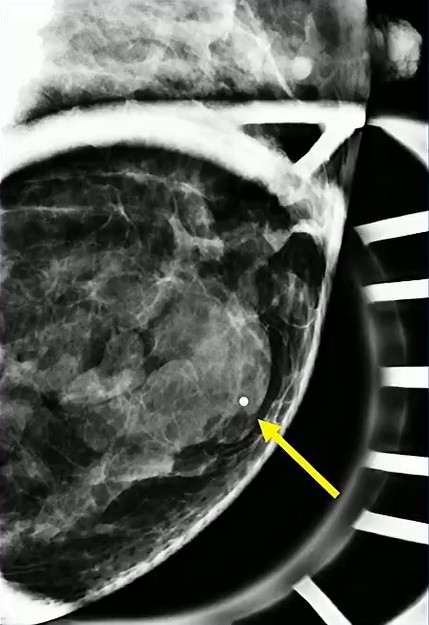
Solid Target: Physiologic lactational changes can introduce cystic elements, creating mixed solid–cystic morphology. When biopsy is indicated, precision matters: sampling the solid portion is essential to secure an accurate diagnosis and avoid false reassurance…as in the case of this 36-year-old postpartum patient (lump x 3 months) with biopsy-proved lactating adenoma.
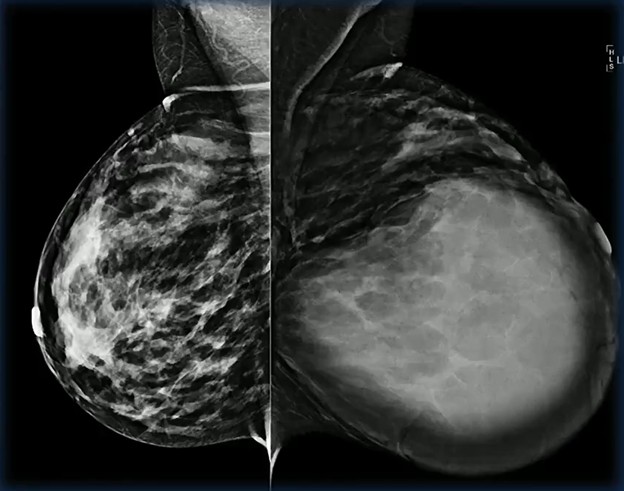
Growth Raises Concern: Rapid enlargement should never be dismissed as purely hormonal. The differential remains broad, including phyllodes tumor, abscess, and malignancy.
In this case involving a 29-year-old patient with a quickly enlarging mass, biopsy confirmed a lactating adenoma—reinforcing that benign lesions can behave dramatically during pregnancy.
Diagnostic Trap! Consider the following scenario: two patients, both 39, both pregnant, both presenting with a mixed solid and cystic mass. One proves to be a lactating adenoma.
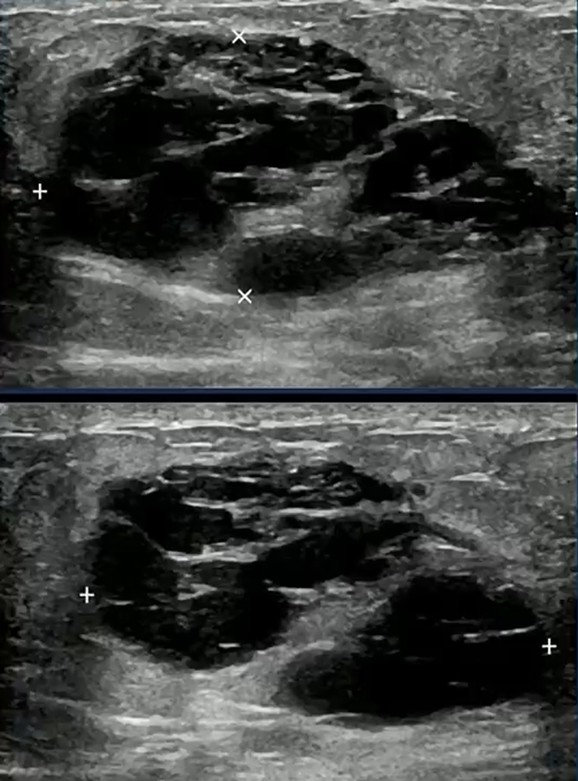
The other is triple-negative breast cancer. Imaging alone may not reliably separate the two.
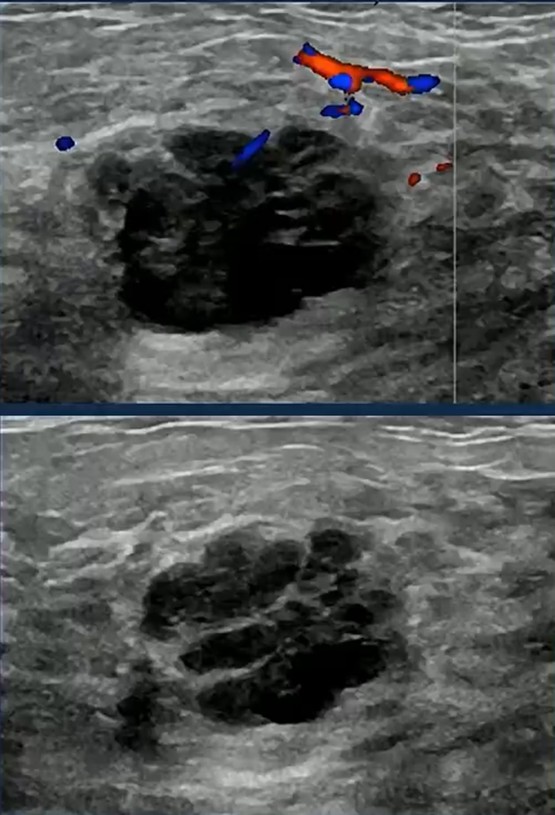
This is the core interpretive hazard in special populations; pattern recognition must be paired with disciplined skepticism.
Pattern → Constraint → Advantage: Lactating adenomas frequently resemble fibroadenomas on imaging. → Mixed morphology and rapid growth can overlap with aggressive cancers, limiting imaging specificity. → Thoughtful targeting for biopsy and early tissue diagnosis convert uncertainty into clarity.
Clinical Takeaway: Pregnancy should lower the threshold for diagnostic rigor. Not raise it! When imaging features and clinical behavior diverge, tissue sampling is the safest path forward.
Bottom Line: In pregnant and lactating patients, the most dangerous mistake is assuming a reassuring pattern guarantees a benign process. Histologic confirmation remains the anchor of confident breast imaging in this population.
Leave a Reply