For radiologists especially, artificial intelligence (AI) is no longer just over the horizon; it’s in the reading room, right now. This practical immediacy is precisely the premise behind the 2026 ARRS Annual Meeting Categorical Course, Clinical Artificial Intelligence in Radiology. Presented live and virtually from the David L. Lawrence Convention Center in Pittsburgh, PA, this two-day ARRS Categorical Course continues our 125-year-old legacy of forward-looking education by arming radiologists with a robust understanding of how AI is reshaping the specialty.
Dr. Shandong Wu | Cat Course Codirector
Clinical Artificial Intelligence in Radiology brings together more than 20 distinguished faculty from leading institutions across the globe, all led by Shandong Wu, PhD, founding director of the University of Pittsburgh’s Center for AI Innovation in Medical Imaging, a cross-campus initiative including more than 130 researcher and clinician members. Also a professor of radiology, biomedical informatics, bioengineering, intelligent systems, clinical and translational science, one of Dr. Wu’s ARRS Cat Course codirectors is an abdominal radiologist and director of diagnostic AI at the University of Washington, Yee Seng Ng, MD.
Dr. Shandong Wu | Cat Course Codirector
Alongside codirector and 2024 AJR Lee F. Rogers International Fellow in Radiology Journalism Hyun Soo Ko, MD (Peter MacCallum Cancer Centre, Australia), the trio is curating a curriculum of more than two dozen lectures and panels across seven thematic sections, giving registrants a comprehensive view of AI’s current and future roles in everyday practice.
SUN, APRIL 12—From Concept to Clinic: Building AI Literacy
Day one of Clinical Artificial Intelligence in Radiology kicks off with “Getting to Know AI,” a primer tailored for all levels of experience. Tessa Cook, MD, PhD (University of Pennsylvania), provides an overview of radiological progress in AI, while Dr. Ko demystifies essential concepts, such as machine learning, deep learning, radiomics, as well as generative and agentic AI.
Dr. Linda Moy | Vice Chair of AI, NYU Radiology
Up next, inaugural vice chair of AI at New York University’s radiology department, Linda Moy, MD, will provide an invaluable look into leveraging AI to improve workflow efficacy and effectiveness alike. Dr. Wu himself closes the Cat Course’s first session. The leader of Pittsburgh’s Intelligent Computing for Clinical Imaging lab will explore and explain how AI is enhancing imaging interpretation for computational insights—from screening and triage to diagnosis and prediction.
Clinical Implementation: From Regulation to Real-World Deployment
Section two of Clinical Artificial Intelligence in Radiology, “AI Clinical Implementation,” addresses legal, regulatory, and operational frameworks essential for radiologists seeking to implement or evaluate AI tools in practice. Didactic highlights will include guidance on U.S. Food and Drug Administration (FDA) regulations and performance monitoring by Melissa Davis, MD, MBA (Yale), as well as insights into distinguishing high-quality AI models from market hype.
In a uniquely insightful presentation, Julian Rivera, JD (University of Pittsburgh), will tackle the legion of legal considerations accompanying AI adoption: liabilities, ethical perspectives on signing contracts, collaborative business modes with AI companies, etc. Dr. Cook returns to share her expertise on evaluating local versus commercial solutions when measuring ROI, while a panel moderated by Dr. Moy will outline best practices and common pitfalls.
Beyond the Pixel: Multimodality and Multidimensional AI
The promise of any good AI expands significantly when paired with non-image data. The “Going Beyond Images to Multimodality” session explores emerging applications that leverage large language models, vision-language models, and foundation models. Presenters Heather Whitney, PhD (University of Chicago), and Lifeng Yu, PhD (Mayo Clinic), will delve into data curation, federated learning, and the physics of AI model performance. With Christian Bluethgen, MD (University Hospital of Zurich), having assessed multimodal data methodologies in his presentation, a panel discussion on tackling technical challenges to find opportunities rounds out day one of this ARRS Cat Course.
MON, APRIL 13—Practical Impact Across Subspecialties
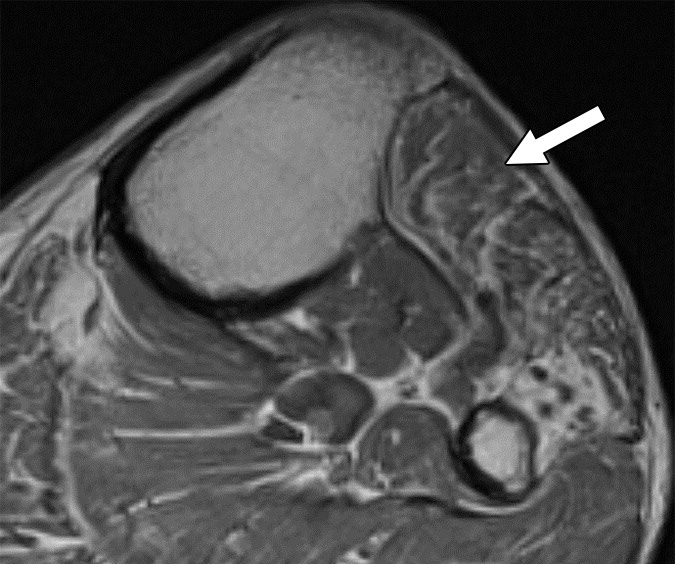
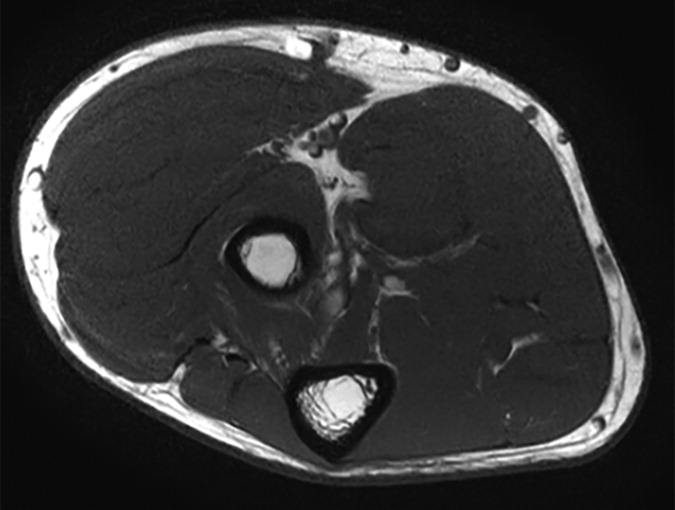
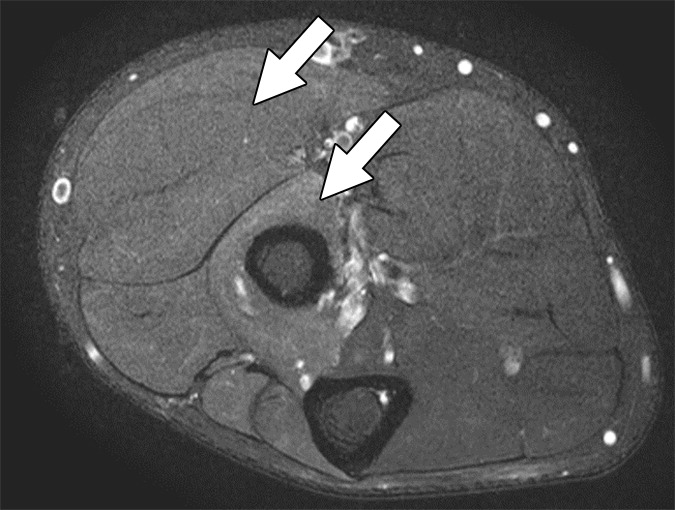
AI’s reach across subspecialties is the focus on Monday. Presenters including Constance Lehman, MD, PhD (Harvard), Ali Guermazi, MD, PhD (Boston University), and 2022 ARRS Gold Medalist Edward Y. Lee, MD, MPH (Harvard) will detail AI tools in breast, musculoskeletal, pediatric imaging, respectively. Dr. Ng’s highly anticipated survey of AI and abdominal imaging will be followed by a lecture from neuroradiologist Paulo De Aguiar Kuriki, MD (UT Southwestern).
Dr. Edward Y. Lee | ARRS Gold Medalist
That’s not all either. Real-world cardiothoracic, interventional, and nuclear medicine cases will further demonstrate how AI is already reflowing imaging workloads, improving diagnostic accuracy, and personalizing care across organ systems and patient populations.
Shaping Tomorrow: Research, Education, and Ethical Engagement
Day two of Clinical Artificial Intelligence in Radiology continues with “AI Research and Education,” including a model development demonstration by Dooman Arefan, PhD (University of Pittsburgh), and an exploration of MD–PhD collaboration opportunities from Dr. Wu. Justin Peacock, MD, PhD (Uniformed Services University), will discuss educational roadmaps and training resources, addressing a key concern for attendees seeking to build or deepen their AI competencies.
This 2026 ARRS Annual Meeting Categorial Course concludes with “Humanity and AI,” a thought-provoking session covering radiologist–AI collaboration, fairness and bias, and imaging’s ever-evolving role in AI-powered services. Florence Doo, MD (University of Maryland) will help us find a foothold in our present human–AI ecosystem, followed by a warning for all the disparities AI run amok could actually exacerbate care of Judy Gichoya, MD, MS (Emory). Eduardo Mortani-Barbosa, MD, MBA (University of Pennsylvania), will then detail specific skill sets that AI-forward radiologists will need to hone in their practices and in their communities. Finally, ARRS Scholar and Gold Medalist and editor of Radiology: Artificial Intelligence Charles E. Kahn, MD (University of Pennsylvania), joins to facilitate a panel discussion on action items and what to do next.
Dr. Charles E. Kahn | Editor, Radiology: Artificial Intelligence
With each live lecture accompanied by an e-book chapter, Clinical Artificial Intelligence in Radiology will provide strategic context and tactical guidance for imagers of each practice type and at every level of training.
And as Dr. Wu tells InPractice, “AI in radiology is not just a technical shift—it’s a cultural one. This ARRS Categorical Course is about empowering radiologists to shape that future, not just react to it.”
With content spanning conceptual foundations to the most practical of pearls, the curriculum curated by Wu, Ng, Ko and colleagues this April is poised to be an essential learning experience for working radiologists looking to engage with AI at the frontlines of medical imaging care.
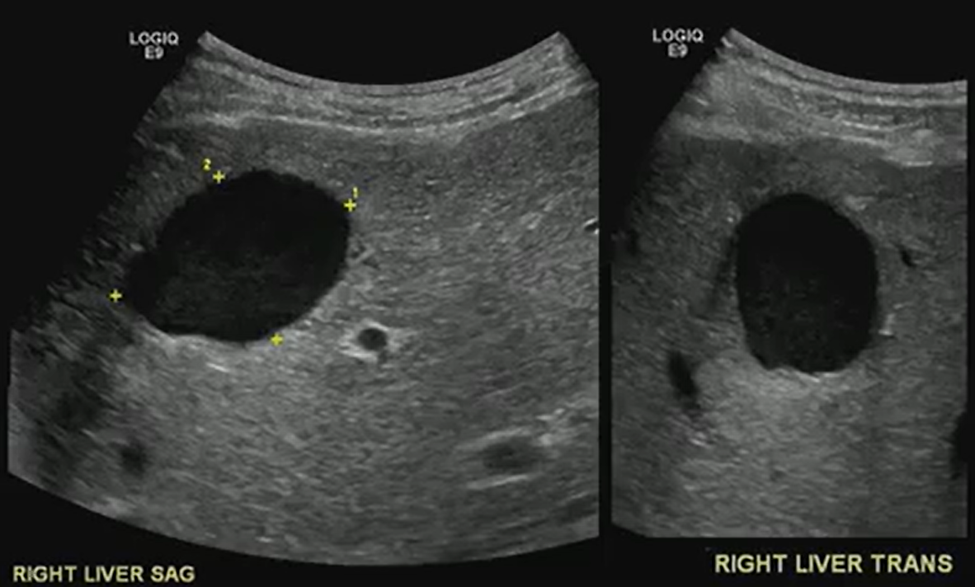
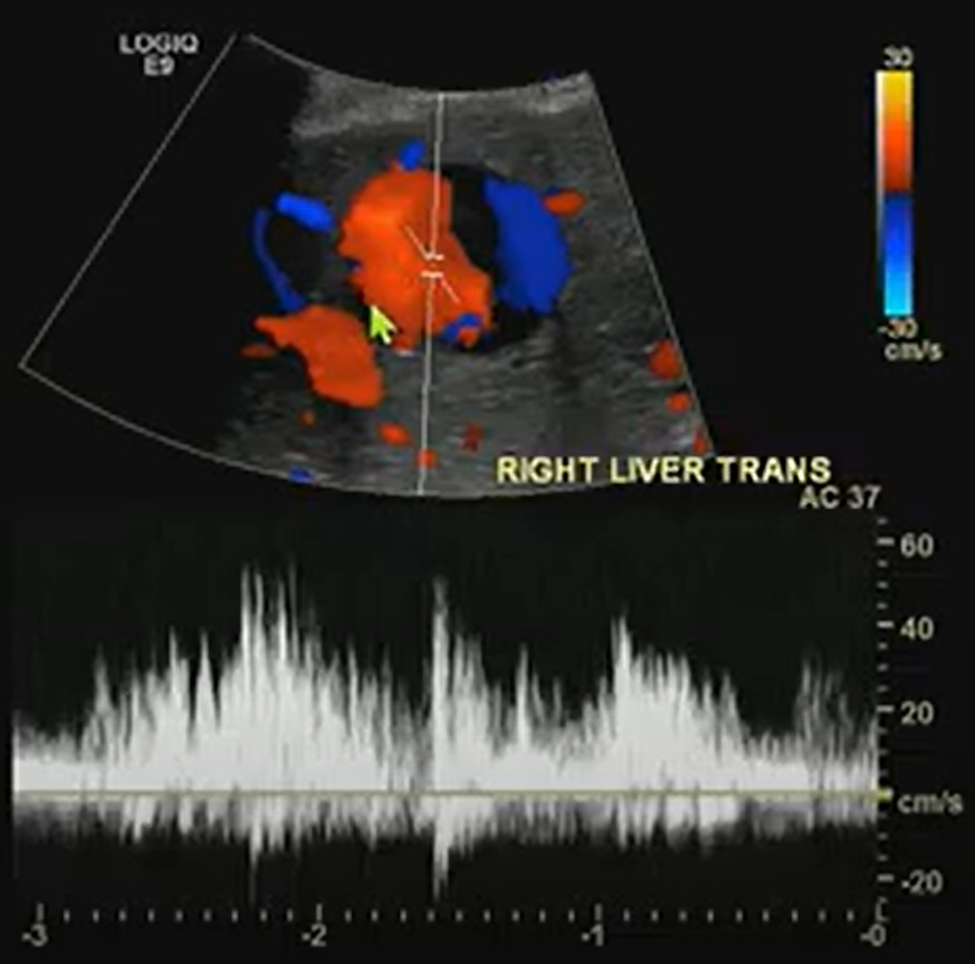
A benign-looking liver lesion turned out to be a hepatic artery pseudoaneurysm—all thanks to color Doppler.
The Big Picture
What looks like a simple hypoechoic cyst on ultrasound may hide a critical vascular pathology. In this ARRS Annual Meeting case from Kristin Rebik, DO, color Doppler proved essential for distinguishing cystic lesions from vascular anomalies like pseudoaneurysms.
Key Takeaways
Always Doppler: Even cyst-like structures require Doppler evaluation to rule out vascular causes.
Pepsi Sign: Swirling vascular flow within a lesion may signal a pseudoaneurysm.
High stakes: Hepatic artery pseudoaneurysms can mimic benign lesions but require urgent recognition and intervention.
Next steps: Interventional radiology embolization can be lifesaving.
Challenges Ahead
Differentiating pseudoaneurysms from other vascular or cystic lesions remains tricky.
Missing Doppler evaluation risks misdiagnosis and delayed treatment.
Awareness of teaching signs like the “Pepsi sign” is uneven among trainees.
Bottom Line
Never skip Doppler. The “Pepsi sign” may be the clue that transforms a benign-looking lesion into a critical vascular diagnosis.
An intersocietal panel of experts in CT convened by the American Association of Physicists in Medicine (AAPM)—with representation from clinical practice, academia, and industry input from Siemens Healthineers and Canon—examined a new performance measure in the quality-based payment programs of the Centers for Medicare & Medicaid Services (CMS). Publishing their findings in the American Journal of Roentgenology [1], the panel identified 20 important issues and ambiguities with the new measure, which became effective this year.
Collectively, these issues reflect unclear definitions, opaque methodologies, technical and legal barriers, and potential misalignment with clinical realities—posing significant obstacles to consistent, equitable, and scientifically valid implementation across diverse care settings.
Ambiguity surrounds where reporting is required versus optional and exactly which adult study types qualify, compounded by difficulties in consistent inpatient versus outpatient categorization. Terminology inconsistencies and unclear mapping of studies to dose and image quality categories add to the confusion. Meanwhile, patient size assessment methodology and calculation of size-adjusted dose diverge from established standards, while noise measurement lacks a recognized protocol. Criteria for excluding studies and handling combination studies remain undefined.
Then, there are the tech queries: is HL7 EHR connectivity mandatory, are alternative data transfer mechanisms even feasible, what potential IT burdens and/or security liabilities will radiology practices have to shoulder? Also, performance expectations for compliance thresholds are unspecified, as are methods for comparing diverse protocols under a single set of thresholds. Identical thresholds across different categories raise additional questions.
“Transparency and stakeholder engagement are essential for effective quality initiatives in medicine,” said Mahadevappa Mahesh, MS, PhD, president of AAPM.
Dr. Mahesh | President, AAPM
“We wrote this paper to call attention to issues and ambiguities with the CMS measure, and we look forward to working with CMS to address these issues and continue the culture of quality and safety that has developed in CT imaging over the past two decades.”
Balancing Image Quality and Patient Safety
One of the benefits to patients that will come from “The New CMS Measure of Excessive Radiation Dose or Inadequate Image Quality in CT: Issues and Ambiguities—Perspectives from an AAPM-Commissioned Panel” in AJR is that the expertise of the entire imaging community will be used to develop quality improvement initiatives that will keep radiation doses as low as possible while maintaining the quality of medically essential CT imaging. From physicians and physicists to technologists, regulators, and business leaders, “we’re confident that we can get this right by working together,” said Dr. Mahesh.
Technology Has Already Lowered Doses
A lifesaving technology used to diagnose disease and guide treatment, CT is the first-line imaging technique in many cases, especially in emergency departments and cancer centers. Concerns have been raised about the increased utilization of CT in medicine because the modality uses ionizing radiation, which at very high doses is known to increase a patient’s risk for developing cancer. However, at the low doses of radiation utilized in medical imaging, including in CT, the risk is extremely small—perhaps negligible.
Over the past two decades, imaging and allied health professionals have collectively worked to reduce CT doses. New scanner technologies have played a starring role in decreasing doses, including features that automatically measure the size of the patient and adjust the radiation dose to the right value. This is especially important for children, who require lower doses than adults due to their smaller size.
Dr. McCollough | Prior President, AAPM
“Some authors multiply the very small potential risk of a CT scan by the millions of patients who receive one and predict that we will see an increase in cancer,” said Cynthia McCollough, PhD, past president of AAPM.
“This can lead to alarmist stories and patients who really need a CT refusing to get one. Further, at the low doses we are talking about, it is debated whether the risk is even real. CT has been around for over 50 years and the predicted increases in cancer just aren’t being seen.”
Editorials Stress Ticking Clock, Call for Clarity
In her accompanying AJR editorial, Stephanie Leon, PhD, of the University of Florida in Gainesville, noted that “quality-based payment programs will be impacted starting in January 2027,” which means that imaging has two years and counting to figure all of this out [2].
CMS Quality Reporting Program
CMS Payment System
Reporting Requirement
Timeline
Hospital IQR Program
HIPPS
Optional. Hospitals are required to report three eCQMs self-selected from a list and three eCQMs mandated by CMS. The measure will be available on the self-selection list and thus its reporting is optional.
Reporting will begin in CY 2025; CY 2025 results will impact FY 2027 payments.
Hospital OQR Program
HOPPS
Required. Once the measure is fully implemented, hospitals will be required to report the measure.
Reporting will be voluntary in CY 2025 and mandatory in CY 2027; CY 2027 performance will impact CY 2029 payments.
MIPSᵃ
MPFS
Optional. Participants are required to report six MIPS quality measures, including at least one outcome measure, that are self-selected from a list (possibly a specialty-defined measure set depending on the reporting mechanism). If more than six measures are available, then reporting the measure is optional.
Reporting will begin in CY 2025; CY 2025 results will impact FY 2027 payments.
Another AJR editorial written by Kishore Rajendran, PhD, of the Mayo Clinic in Rochester, MN, and chair of the working group on the physics of quantitative imaging at AAPM, called for improved transparency, too. “A nonproprietary, community-based approach is imperative to ensure full transparency, achieve consensus among CT stakeholders, and provide reliable clinical diagnoses at the lowest radiation dose possible,” wrote Dr. Rajendran [3].
Watch as AJR senior author Ehsan Samei, PhD, and first author Jered R. Wells, PhD, call for a fundamental shift toward open-source, open-access, consensus-based, and community-owned strategies and resources to ensure quality and safety of CT: YouTube.com/@AJR_Radiology
References:
Wells JR, Christianson O, Gress D, et al. The new CMS measure of excessive radiation dose or inadequate image quality in CT: issues and ambiguities—perspectives from an AAPM-commissioned panel. AJR 2025 May. doi: 10.2214/AJR.24.32458
Leon, SM. CMS measure on CT dose and image quality: good intentions, but not quite ready for prime time. AJR 2025 May. doi: 10.2214/AJR.25.32908.
Rajendran K. Transparency and stakeholder engagement as cornerstones for effective quality initiatives in medical imaging. AJR May. doi: 10.2214/AJR.25.32859
When it comes to the cervical spine, cord integrity matters most. Even mild changes can spell trouble if the cord is compromised.
Big Picture: Cervical canal stenosis isn’t just about the degree of narrowing; it’s about whether the spinal cord, itself, is at risk, too. Even without measurable stenosis, cord flattening can cause myelopathy. Understanding Dr. Lea Alhilali’s fishbowl analogy from the ARRS Neuroradiology Longitudinal Course helps clarify how to distinguish mild, moderate, and severe cases.
Key Takeaways:
Cord first: Regardless of canal narrowing, deformity or signal changes in the cord point to a higher risk of myelopathy.
Not just static: Static imaging may underestimate the impact; dynamic forces, repetitive microtrauma, or microischemia may drive symptoms.
“Fishy” Analogies…
Mild stenosis: Either ventral or dorsal CSF is effaced, but the cord still has room to “swim.”
Moderate stenosis: Both ventral and dorsal CSF are lost, restricting cord movement.
Severe stenosis: No CSF remains—cord is compressed, “fish” crushed.
Challenges Ahead
Why cord flattening causes myelopathy without stenosis remains unclear, and mechanisms are still debated.
Dynamic assessment may offer better insight than static MRI but isn’t standardized.
Management depends on correlating imaging with clinical findings, which are often nuanced.
Bottom Line: Think of the cervical cord like a fish in a bowl: it needs space to move. Once the CSF “water” is gone, the cord, as well as the patient, suffers. Classifying stenosis by available space—not merely narrowing—sharpens diagnostic accuracy and clinical relevance.
Reiterating, the house of radiology’s influence in shaping our nation’s health care policy writ large, the American Medical Association (AMA) House of Delegates (HOD) advanced several measures with significant implications for American Roentgen Ray Society (ARRS) members during its own annual meeting in Chicago this June.
In short: expect DICOM mandates to simplify imaging transfers, elevated oversight of AI, and more rigorous validation for CT-based calcium scoring [1].
Finally, Federally Interoperable DICOM
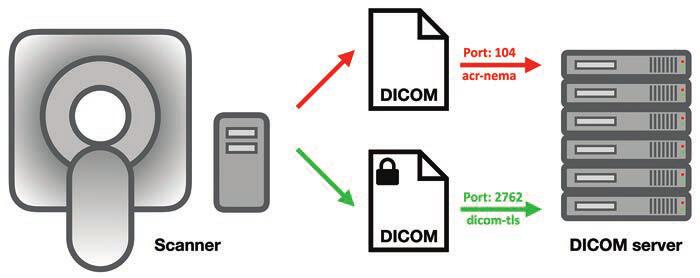
The HOD passed a pivotal resolution calling on AMA advocacy for federal health IT interoperability standards to include the DICOM format, a critical “missing link” that delegates have long championed. Despite over two decades of EHR development and federal mandates, DICOM has been excluded from formal interoperability frameworks. As a result, radiological images frequently cannot travel seamlessly through EHR systems, frustrating patients and providers alike. For one example, patients arriving for mammograms at new facilities are often dumbfounded that previous studies cannot be accessed digitally from elsewhere. The absence of interoperable imaging standards contributes to delayed care, redundant exams, unnecessary radiation exposure, and burdens for patients. And the security risks are legion (Fig. 1).
Fig. 1—Schematic shows DICOM server, computers that can exchange and store DICOM objects. Server offers DICOM service, which is software that can send and receive DICOM messages, running via specific computer ports (i.e., communications channels). Secured DICOM service is known as dicom-tls (port 2762), which uses transport layer security for negotiations, authentication, and encryption. A service that cannot be queried by hackers because it uses strong authentication mechanisms, this service sends and receives encrypted DICOM messages that cannot be read by hackers either. However, this is only true for manufacturers that have chosen to implement its strong authentication and encryption features. Arrows show direction of data transmission.
Spearheaded by neurology and orthopedic associations, this resolution urges inclusion of DICOM in the U.S. Core Data for Interoperability (USCDI) and seeks regulatory action requiring EHR and imaging archive vendors to support secure, efficient exchange of DICOM data. Testimony also highlighted policy fissures stemming from the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009, which exempted radiologists—alas, not viewed as patient-facing—from certain data-sharing requirements, thereby keeping imaging outside USCDI [2]. A significant win for medical imagers across the country, delegates did have to amend the resolution to get it passed, but this is meaningful progress toward closing the interoperability gap that hampers timely, coordinated, and secure care.
More Oversight and Transparency for AI
With AI digging even deeper into the specialty—at last count, over 75% of the more than 1,000 algorithms cleared by the Food and Drug Administration target radiology [3]—the HOD continued sounding the alarm on the “black box” nature of so many machine-learning, deep-learning, and radiomic systems. Resolution 519, though not adopted thanks to too much overlap with AMA’s existing AI policies, successfully highlighted acute issues of explainability, advocating for evidence-based, transparent AI within a deliberately structured framework [4]. Aligning with AMA’s stance that the physician’s expertise remains central to clinical decision-making, everyone in Chicago agreed that today’s radiologists must be able to comprehend and articulate how generative AI, agentic AI, or some future proprietary amalgam of the two arrives at any given verdict. All too often, seemingly slight updates to vendor hardware, scanning protocol, or patient demographics end up altering algorithmic performance, further underscoring the need for responsible vetting and robust monitoring of AI.
No LDCT for Coronary Calcium, Yet
AMA also tabled a resolution regarding expanded promotion and usage of low-dose CT (LDCT) to screen both lung cancer and coronary artery disease via coronary calcium scoring. Emphasizing the modality’s value as a public health tool for high-risk individuals, particularly those with pack-year history of smoking, LDCT delivers far less radiation than standard CT and can detect small lung nodules early. Indeed, crucial research from the National Lung Screening Trial shows it can reduce lung cancer mortality by up to 20% [5].
And yet, uptake is still cripplingly low; fewer than 6% of eligible patients receive LDCT screening. To buttress the resolution’s goals, the American College of Radiology is launching complementary efforts, including expanding its early lung cancer registry to capture incidental findings from routine CTs, not just formal screening exams [6]. Such distinction will deepen insights into nodule detection and follow-up.
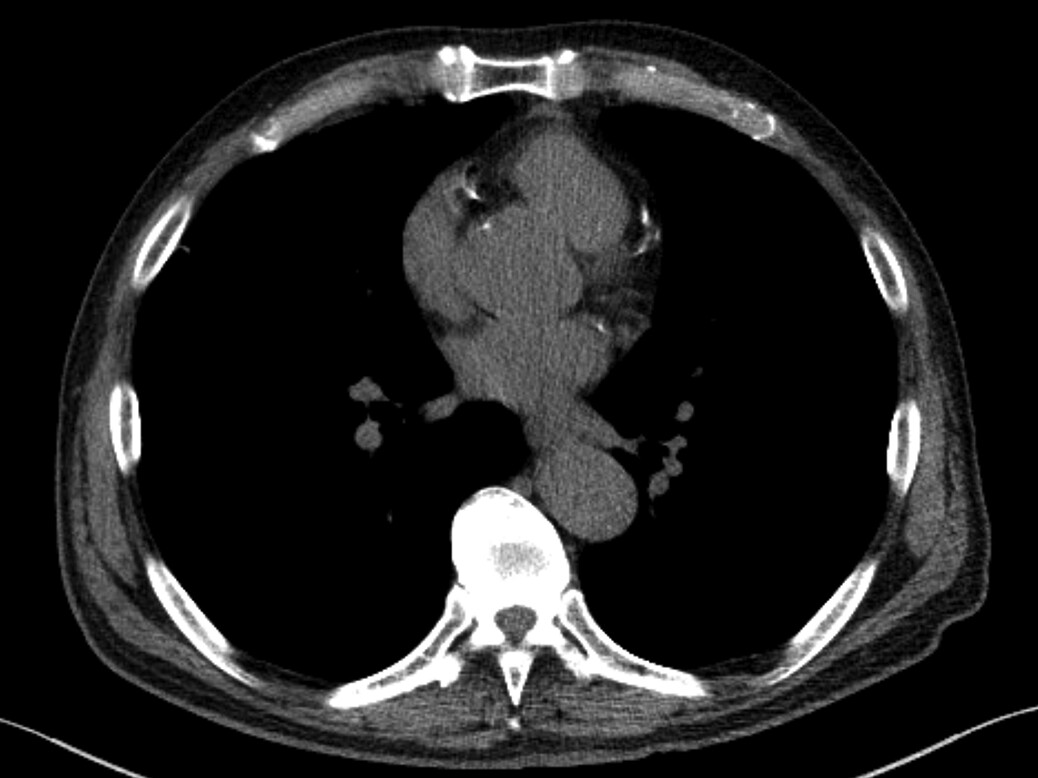
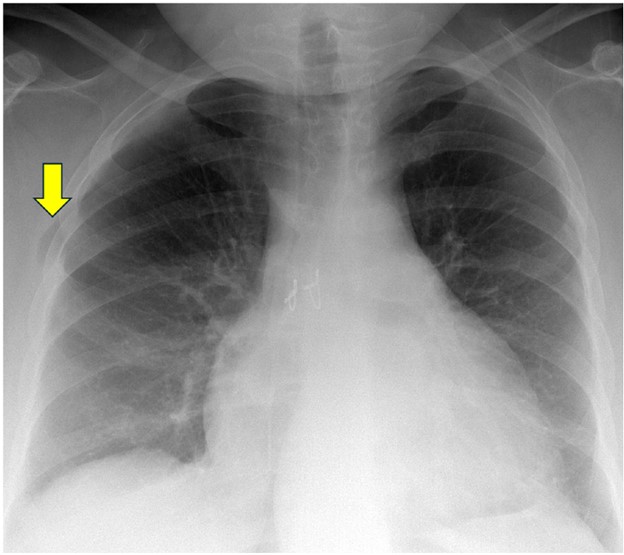
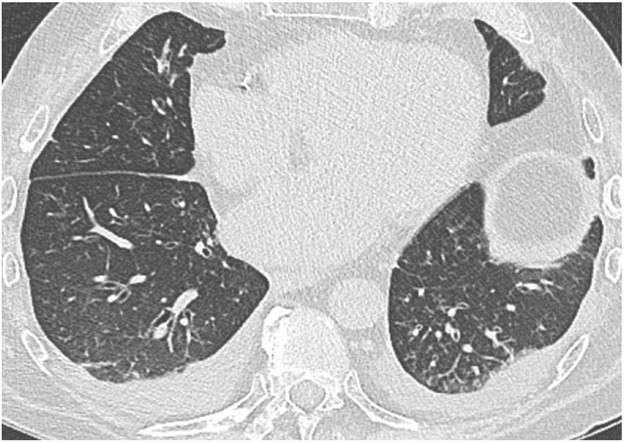
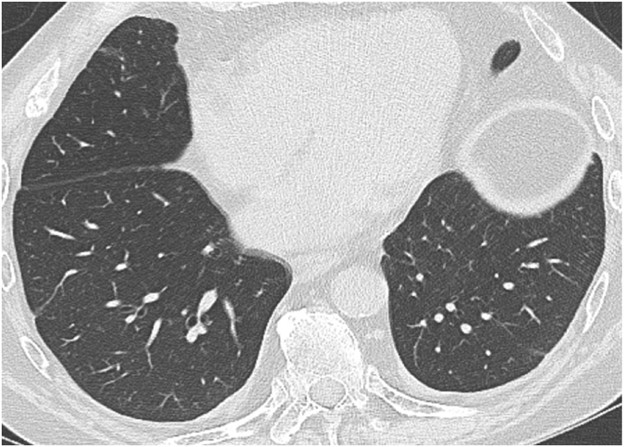
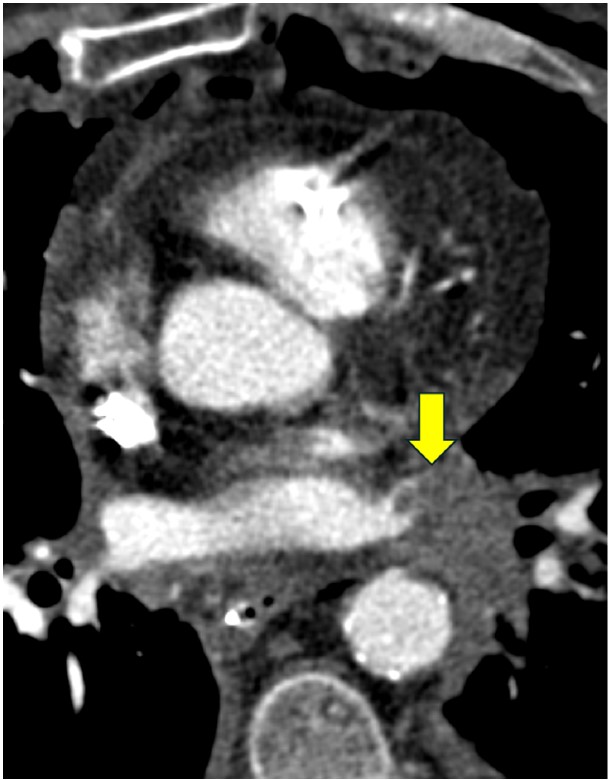
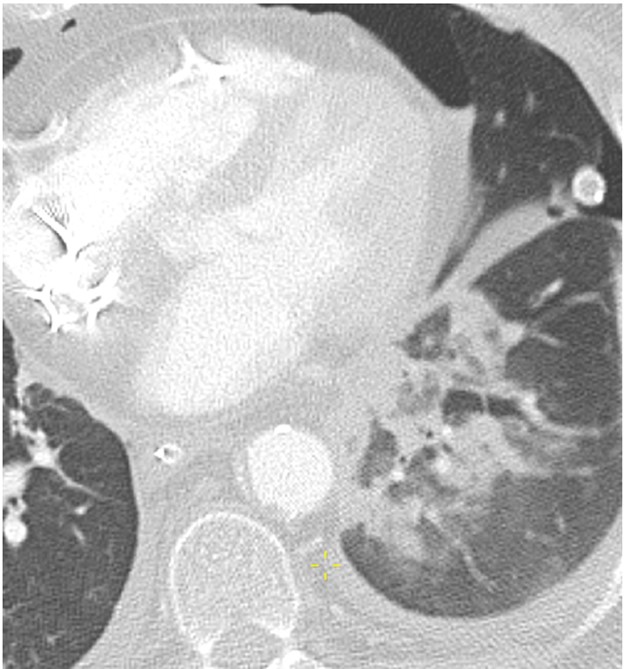
Fig. 2—73-year-old patient who underwent lung cancer screening by LDCT of the chest. Axial CT image shows coronary artery calcification (CAC). CAC was assessed as severe by consensus visual analysis.
More broadly, many hospitals have begun offering low- or no-cost LDCT screenings as an entry point for preventive care. Apropos, this resolution specifically solicits a coordinated national effort of public awareness campaigns and provider education to ensure affordable, widespread access to this potentially life-saving tool.
For further details about the 2025 Annual Meeting of the HOD, click here.
Stacy J. Kim, MD Mallinckrodt Institute of Radiology Washington University in St. Louis
The first human lung transplant was performed in 1963. Since then, the number of lung transplant cases in the United States has steadily increased due to continued advancements in surgical technique and immunosuppressive medication. There were over 3000 lung transplants performed in the United States in 2023, and the number of lung transplants is likely to continue to increase [1]. The patients who undergo lung transplant are those with end-stage lung disease, which can result from a variety of pathologies including emphysema, fibrosing interstitial lung disease, cystic fibrosis, and pulmonary arterial hypertension. Postoperatively, these lung transplant recipients are vulnerable to complications for the remainder of their lives. The complications can be categorized by time course; that is, the time period after transplant during which the complications occur or most often occur.
The postoperative time periods can be organized as follows: immediate, within 24 hours of transplant; early, from 24 hours to 1 week after transplant; intermediate, from 1 week to 3 months after transplant; and late, more than 3 months after transplant [2]. Some complications can occur during more than one time period or span multiple time periods. This chapter will discuss the complications that occur or most often occur during the 1st month or so after lung transplant, which includes immediate, early, and some of the intermediate complications. Late complications of lung transplant will be discussed during the 2025 ARRS Annual Meeting Categorical Course, “Comprehensive Insights Into Transplant Imaging,” in San Diego, CA, and online April 27-May 1.
Imaging Techniques
Chest radiography is the most commonly used imaging study in the immediate and early postoperative setting. Chest radiographs are easy to acquire at the bedside and are useful in evaluating the positions of tubes and lines, which are ubiquitous immediately after transplant, such as endotracheal tubes, central venous catheters, and chest tubes. The lung parenchyma and the pleura can also be evaluated with chest radiographs for complications such as pneumonia and pleural effusion. Given the lower radiation dose of chest radiography when compared with CT, chest radiographs are useful for serial imaging; that is, image acquisition over multiple days to assess for change over time.
CT of the chest is performed if a more detailed assessment of the chest is required. Example scenarios in which a detailed assessment may be necessary include if there is concern for bronchopleural fistula in the setting of a persistent pneumothorax, if a pulmonary embolism (PE) is suspected due to new-onset tachycardia, and if a patient with decreasing hemoglobin values must be evaluated for hemorrhage. A noncontrast chest CT examination is sufficient for evaluation of the lung parenchyma, airways, and bones. A contrast-enhanced chest CT examination should be acquired (if the patient’s renal function permits and if the patient does not have a contrast media allergy) for evaluation of the vasculature and the pleura and assessment for active hemorrhage. The protocol or phase of contrast should be tailored to the diagnosis being evaluated; for example, a PE protocol should be used when evaluating for PE.
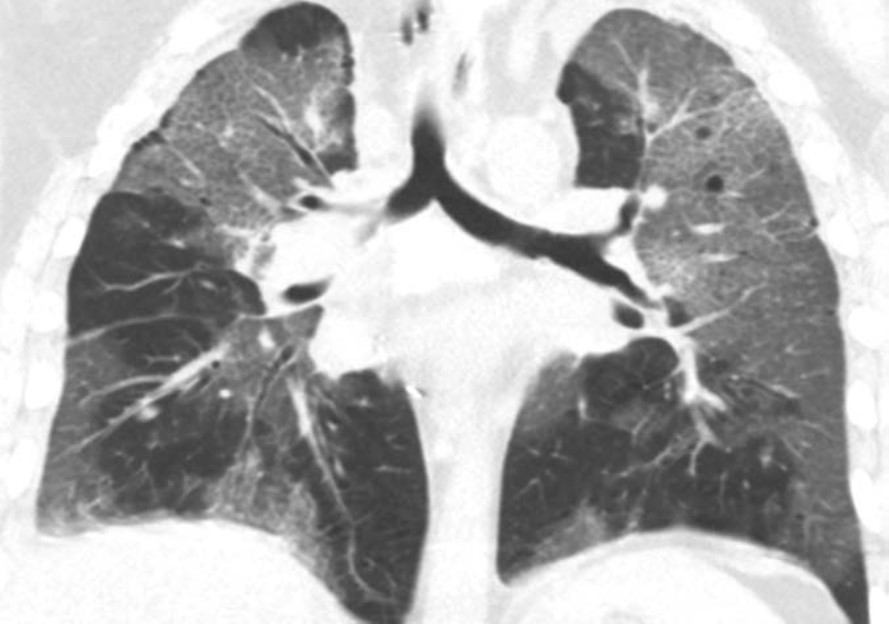
A noncontrast high-resolution chest CT examination is rarely necessary for the evaluation of early lung transplant complications. However, it is useful for the evaluation of late lung transplant complications as it can be used to detect air trapping and fibrosis (discussed in the next chapter). MRI, sonography, and nuclear medicine imaging are not typically used in the evaluation of early lung transplant complications.
Hyperacute and Acute Rejection
Hyperacute rejection occurs during the lung transplant surgery or within 24 hours of transplant when preformed recipient antibodies react to donor antigens in the allograft [3]. It is exceedingly rare because ABO blood group antigens and human leukocyte antigens are taken into account when lung donation is arranged, to ensure donor-recipient compatibility. Hyperacute rejection manifests as fulminant multiorgan system failure, and most patients with hyperacute rejection die within a few days to 2 weeks after lung transplant. The imaging findings of hyperacute rejection are nonspecific and resemble severe pulmonary edema, including consolidation, ground-glass opacities, and septal-line thickening. Acute rejection can occur anytime after lung transplant. It consists of two types, acute cellular rejection (ACR) and antibody-mediated rejection (AMR), which can coexist. ACR is the more common of the two types and occurs when recipient T lymphocytes attack donor antigens within the lung allograft. Approximately 35% of lung transplant recipients experience at least one episode of ACR during the 1st year after transplant [2]. During these episodes, patients may be asymptomatic or may present with nonspecific symptoms such as dyspnea and cough. The imaging findings of ACR are nonspecific and include consolidation, ground-glass opacities, and septal-line thickening; as with hyperacute rejection, ACR resembles pulmonary edema. Given its nonspecific clinical and imaging manifestations, ACR requires transbronchial biopsy and tissue analysis for diagnosis. Timely treatment, typically by increased immunosuppression with steroids, is important because ACR is the greatest risk factor for chronic lung allograft dysfunction [4]. Figure 1 shows a patient with biopsy-proven ACR.
Fig. 1—Patient with history of bilateral lung transplant who developed acute cellular rejection (ACR). Left: Chest CT at time of biopsy-proven ACR shows bronchial wall thickening and nodular ground-glass opacities in both lungs, as well as small pleural effusions. Right: Chest CT several months after treatment of ACR shows resolution of bronchial wall thickening, ground-glass opacities, and pleural effusions.
AMR, the less common of the two types of acute rejection, occurs when recipient B lymphocytes create donor-specific antibodies (DSA), donor-specific antigens and DSA form complexes, and the complexes trigger the immune system’s complement pathway. Like patients with ACR, patients with AMR can be asymptomatic; can have nonspecific symptoms such as dyspnea and cough; and can have normal chest imaging or nonspecific imaging findings resembling pulmonary edema such as consolidation, ground-glass opacities, and septal-line thickening. Transplant physicians diagnose patients with clinical versus subclinical AMR and definite versus probable versus possible AMR on the basis of the presence or absence of allograft dysfunction, histology results suggestive of AMR (such as neutrophil arteritis and capillaritis), immunostaining results (positive C4d staining of the capillary endothelium), and the presence or absence of DSA in peripheral blood [4]. Treatments include plasmapheresis and IV immunoglobulin to remove harmful antibodies and to suppress antibody production, respectively. Steroids are not typically used to treat AMR, unlike ACR. Figure 2 shows a patient with AMR.
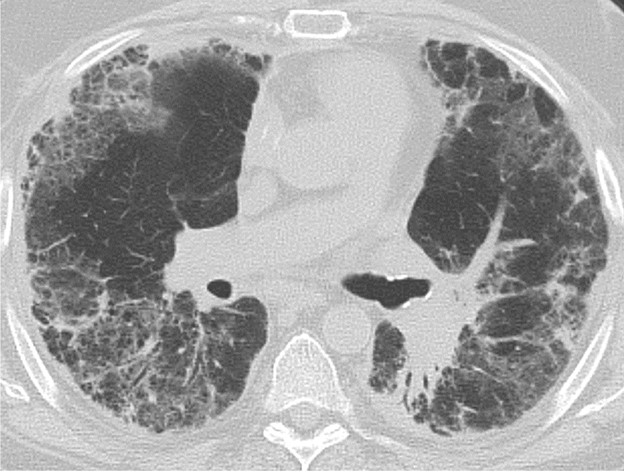
Fig. 2—Patient with history of bilateral lung transplant who developed antibody-mediated rejection (AMR), which was diagnosed by transbronchial biopsy and donor-specific antibody blood testing. Chest CT at time of AMR diagnosis shows ground-glass opacities and reticulation in both lungs and small pleural effusions.
Primary Graft Dysfunction
Primary graft dysfunction (PGD) is a transient complication that occurs within 24–72 hours after lung transplant and tends to resolve by postoperative day 5–10. PGD is thought to be secondary to ischemic injury of the allograft before and during transplant and secondary to reperfusion injury after transplant. PGD occurs in approximately 10–30% of lung transplant recipients [5]. On imaging, it manifests as perihilar and lower lung–predominant airspace and interstitial opacities and is similar in appearance to pulmonary edema. Clinically, PGD is graded from 0 to 3 on the basis of the presence or absence of imaging abnormalities and the severity of hypoxemia [6]. In patients who have undergone a unilateral lung transplant, PGD and pulmonary edema can be differentiated by observing the distribution; PGD affects only the lung allograft, whereas pulmonary edema affects both the lung allograft and the native lung. Like acute rejection, PGD is considered a risk factor for chronic lung allograft dysfunction. It is treated with supportive care, such as mechanical ventilation and extracorporeal membrane oxygenation. Figure 3 shows a patient with PGD.
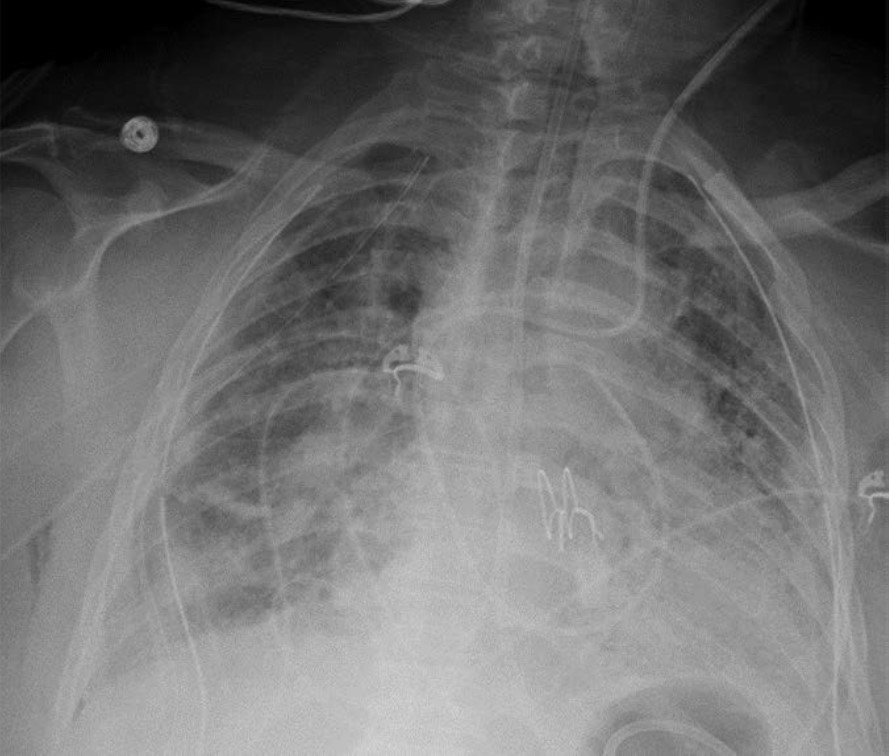
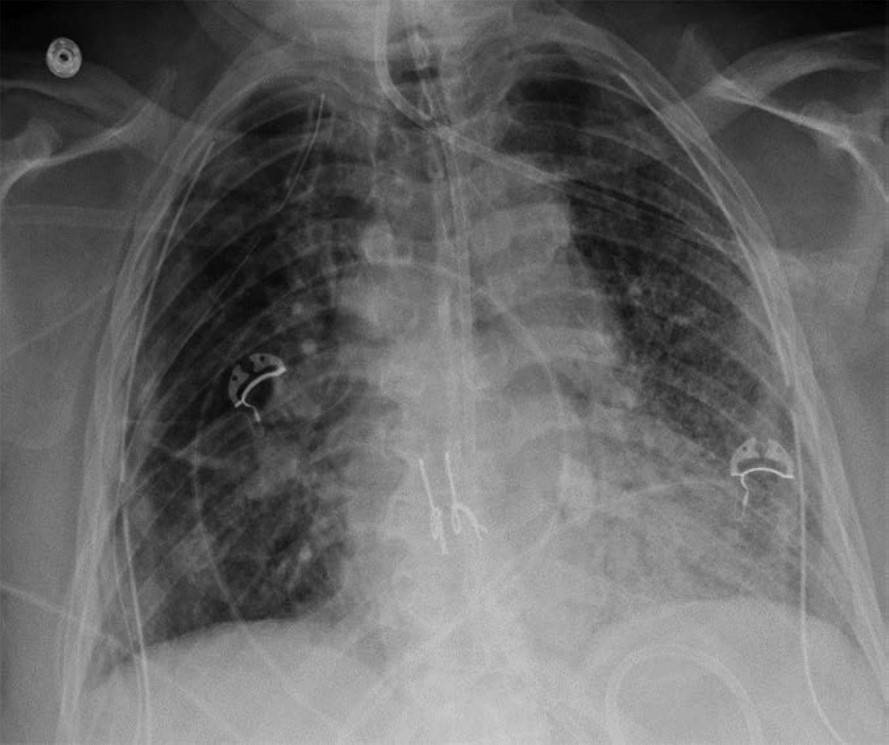
Fig. 3—Patient with right lung transplant who developed primary graft dysfunction (PGD). Left:Chest radiograph on postoperative day 0 shows clear right lung allograft and fibrosis of native left lung. Center: Chest radiograph on postoperative day 3 shows interval development of hazy airspace opacities throughout right lung allograft. Right:Chest radiograph on postoperative day 4 shows near resolution of right lung allograft airspace opacities, consistent with PGD.
Infection
Infection of the lung parenchyma and airways is exceedingly common after lung transplant due to immunosuppression and decreased mucociliary clearance in the airways after transplant. Infection can occur anytime after transplant, including the early postoperative period. Patients are vulnerable to bacterial pneumonia as well as viral and fungal pneumonias not commonly encountered in immunocompetent patients. Common pathogens include Pseudomonas organisms, Staphylococcus aureus, cytomegalovirus, Epstein-Barr virus, herpes simplex virus, Aspergillus organisms, and Candida organisms [2]. The clinical and imaging manifestations of pneumonia in transplant recipients are similar to those of nontransplant patients. Lung transplant recipients who present with dyspnea, cough, or fever are evaluated for pneumonia. Imaging findings of pneumonia include consolidation, ground-glass opacities, septal-line thickening, and pulmonary nodules. Pulmonary nodules can be single or multiple; they may be solid or ground-glass in attenuation. Cavitary nodules and nodules with ground-glass halos can occur, especially in patients with fungal pneumonia. Imaging studies should be scrutinized for complications of infection such as pulmonary abscess and bronchopleural fistula. Patients may also have reactive pleural effusions or reactive mediastinal or hilar lymphadenopathy. Treatment is the same as in nontransplant patients and consists of antibiotics, antivirals, or antifungals depending on the causative pathogen. Figure 4 shows three different lung transplant recipients with pneumonia.
Fig. 4—Three different patients with history of bilateral lung transplant who presented with pneumonia. Left:Chest CT image shows consolidation and numerous small nodules in lungs due to bacterial pneumonia, in addition to left lower lobe cavitation and left empyema with gas in pleural space. Center: Chest CT image shows ground-glass opacities and septal-line thickening throughout both lungs caused by viral pneumonia (SARS-CoV-2). Right:Chest CT image shows cavitary lesion and multiple small nodules in right lung in patient with fungal (Aspergillus) pneumonia.
Pleural Complications
Simple pleural effusions and small pneumothoraces are frequently encountered in the immediate and early posttransplant setting and typically resolve within a few days to 1 week or so after lung transplant. Pleural fluid collections and pneumothoraces that are large, increasing in volume over time, or persist over 1 week may indicate a potentially serious complication such as hemothorax, empyema, bronchial anastomotic dehiscence, or bronchopleural fistula.
Hemothorax, the presence of blood products in the pleural space, should be suspected if there is rapid increase in the volume of pleural fluid over serial imaging or if pleural fluid is hyperattenuating relative to simple fluid on CT. Hemothorax can be heterogeneous in attenuation on CT due to mixing or layering of new blood products with old blood products; a fluid-fluid level may be present. Figure 5 (left) shows a patient with hemothorax.
Fig. 5—Two different patients with history of bilateral lung transplant who presented with hemothorax and empyema. Left: Chest CT image shows large heterogeneous-attenuation collection throughout right pleural space, consistent with hemothorax. Right: Chest CT image shows small- to moderate-volume collection in left pleural space with associated visceral and parietal pleural thickening and enhancement extending into prior left chest tube track, consistent with empyema. Patient also has small right pleural effusion with mild pleural thickening.
Empyema, the presence of infected material (i.e., pus) in the pleural space, should be suspected if there is persistence of pleural fluid over serial imaging for more than 1 week or so after transplant and if visceral and parietal pleural thickening or loculated pleural fluid is present on chest CT. On contrast-enhanced CT of the chest, patients with empyema may have abnormal thickening and enhancement of the visceral pleura and parietal pleura with fluid between the two pleural layers, which is known as the split pleura sign. Figure 5 (right) shows a patient with empyema.
Pneumothorax, the presence of gas in the pleural space, may be indicative of a bronchial anastomotic dehiscence or a bronchopleural fistula if it persists more than 1 week after transplant or increases in volume over time. A tension pneumothorax with cardiomediastinal shift away from the affected hemithorax should be immediately communicated to the transplant medicine team, as an untreated tension pneumothorax can cause cardiovascular and respiratory collapse. Small pneumothoraces on immediate postoperative chest imaging that resolve over the next few days, at which point any chest tubes present would be removed, are considered to be expected postoperative findings.
Treatment of pleural collections typically involves drainage of the pleural space material via pleural catheters or thoracostomy tubes. Surgical intervention may be required if drainage via catheters and tubes is unsuccessful or if the pleural collections are caused by complications such as bronchial anastomotic dehiscence or a bronchopleural fistula.
Vascular Complications
PE can occur after lung transplant. Hemorrhage most commonly occurs during the immediate and early postoperative periods and can manifest as hemothorax, other forms of thoracic hemorrhage such as mediastinal hematoma and chest-wall hematoma, and nonthoracic hemorrhage such as retroperitoneal hematoma. Approximately 4.5% of lung transplant recipients experience posttransplant hemorrhage severe enough to require surgical intervention [7]. The causes of hemorrhage include inadequate coagulation, vascular anastomotic dehiscence (which is rare but can be catastrophic when it occurs), and injury of other vessels. CT of the body part of concern (for example, CT of the chest if there is concern for mediastinal hemorrhage) should be performed, ideally with IV contrast material. If active hemorrhage is suspected, CT can be performed before and after the administration of IV contrast material in the arterial and venous phases to detect contrast material extravasation.
PE also most commonly occurs during the immediate and early postoperative periods. Patients are typically bedbound for at least the first few days after lung transplant, and some patients require mechanical ventilation during that time. Some patients may have been bedbound and/or may have been receiving mechanical ventilation while awaiting the transplant surgery. Immobility increases these patients’ risk for developing deep venous thrombosis (DVT) and subsequently developing PE. It is important to understand that lung transplant recipients are at increased risk of pulmonary infarction secondary to PE because the bronchial circulation is not reestablished during the transplant, and until collateral vessels form in a few weeks, these patients are relying on blood supply from the pulmonary circulation. If PE is suspected, CT of the chest with IV contrast material should be performed per the PE protocol.
The imaging findings of hemorrhage and PE are the same in lung transplant recipients as in nontransplant patients. Hemorrhage manifests as hyperattenuating fluid (higher attenuation than that of simple fluid) or a hyperattenuating mass (if it is a hematoma) that often has a heterogeneous appearance. PE manifests as hypoattenuating and well-defined filling defects in the contrast material–opacified pulmonary artery branches. These filling defects can be occlusive or nonocclusive; nonocclusive acute PE is centrally located in the vessel lumen, rather than eccentric. Patients with coagulopathy and patients who are receiving anticoagulation therapy for DVT or PE may have both hemorrhage and PE on imaging. Figure 6 shows a patient with bilateral chest-wall hematomas.
Fig. 6—Patient with history of bilateral lung transplant who developed deep venous thrombosis in early postoperative setting was prescribed anticoagulation therapy and then spontaneously developed chest-wall hematomas, left greater than right. CT image shows heterogeneous-attenuation collections in right and left chest walls deep to pectoralis major muscles, which represent hematomas.
Pulmonary vein thrombosis and pulmonary venous anastomotic stenosis occur during the immediate and early postoperative periods, usually within 48 hours of lung transplant [8]. In pulmonary vein thrombosis, CT of the chest with IV contrast material shows a filling defect within a pulmonary vein, which may or may not be accompanied by consolidation, ground-glass opacities, and septal-line thickening in the lung parenchyma drained by the thrombosed pulmonary vein; the airspace opacities and septal-line thickening represent edema and hemorrhage due to venous ischemia and infarction. Endovascular intervention can be attempted, but cases of severe pulmonary vein thrombosis require surgery. Figure 7 (left) shows a patient with pulmonary vein thrombosis.
Fig. 7—Patient with history of bilateral lung transplant who presented with thrombosis of left inferior pulmonary vein. Left: Chest CT image acquired day after lung transplant shows occlusion of left inferior pulmonary vein (arrow). Right: Chest CT image shows consolidation and ground-glass opacities in left lower lobe indicative of edema and hemorrhage due to venous ischemia.
The pulmonary venous anastomosis is created adjacent to the left atrium. Stenosis of the pulmonary venous anastomosis is rare compared with stenosis of the pulmonary arterial anastomosis. On imaging, stenosis manifests as a focal narrowing of the pulmonary vein anastomosis that may or may not be accompanied by findings of venous ischemia and infarction in the lung parenchyma drained by the affected pulmonary vein, such as consolidation, ground-glass opacities, and septal-line thickening. As with pulmonary vein thrombosis, treatment options include endovascular intervention and, in severe cases, surgical repair. Figure 7 (right) shows a patient with pulmonary venous anastomotic stenosis.
Mechanical Complications
Mechanical complications include pulmonary torsion and lung herniation. Pulmonary torsion is a very rare complication of lung transplant and occurs during the immediate and early postoperative periods. A risk factor for lung torsion is when the donor lung is small relative to the recipient thoracic cavity, which means that the allograft is more mobile and likely to twist around its vascular pedicle after the transplant [9]. Careful size matching between the donor lung and the recipient chest cavity before the transplant surgery has greatly reduced the risk of lung torsion; however, given the potentially catastrophic consequences of torsion and the need for emergent surgical intervention, it remains an important diagnosis to be aware of. As previously stated, lung transplant recipients are particularly vulnerable to allograft ischemia and infarction because the bronchial circulation is not reestablished during transplant and the lung allograft must rely on pulmonary circulation until collaterals can form. Vascular compromise of the allograft due to torsion can result in severe allograft damage, allograft failure, or even death.
Imaging findings of pulmonary torsion can involve a lobe (in lobar torsion) or the entire lung (if the entire lung has twisted around its vascular pedicle). Pulmonary torsion can manifest as volume loss or collapse of the affected lobe or lung; it can also manifest as rapid expansion or opacification of the affected lobe or lung. Because of the twisting that occurs in torsion, patients with torsion have abnormal orientations and positions of anatomic structures such as lobes, hila, fissures, vessels, and airways. There may be abrupt cutoff of vessels and bronchi at the site of twisting. If pulmonary torsion is confirmed or suspected, the transplant physicians should be notified immediately to salvage as much of the allograft as possible. Pulmonary torsion requires emergent surgery to prevent allograft infarction and patient death.
Lung herniation can occur anytime after lung transplant. A major risk factor for lung herniation is increased intrathoracic pressure, as can be seen in patients with persistent cough due to pneumonia or aspiration after transplant. On imaging, herniated lung has an abnormal contour with a portion of lung bulging into the chest wall; this can occur at surgical sites (such as thoracotomy incisions) or at intercostal spaces. Mild herniation involving a small portion of the lung allograft with normal-appearing parenchyma is not worrisome. However, herniation involving a large portion of the allograft or deep herniation into the chest wall places the patient at risk for atelectasis, ischemia, infarction, and gangrene of the herniated lung, all of which can manifest as opacities within the herniated portion of lung. Surgical repair of the chest wall may be necessary in cases of pulmonary infarction or gangrene. Figure 8 shows a patient with lung herniation.
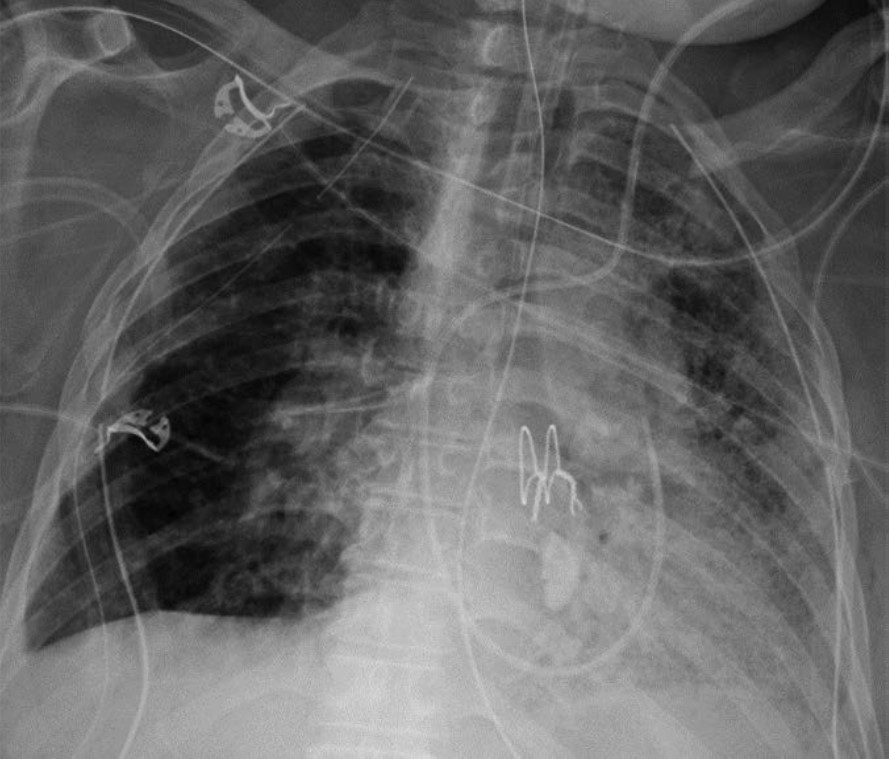
Fig. 8—Patient with history of bilateral lung transplant who presented with lung herniation. Frontal chest radiograph shows mild herniation of small portion of right upper lung into chest wall at thoracotomy incision site (arrow).
Conclusion
Lung transplant is increasingly becoming a cure for many patients with end-stage lung disease. In addition to academic chest radiologists, private practice radiologists and general radiologists are likely to encounter lung transplant recipients at some point in their careers. It is therefore essential for all radiologists to have a basic understanding of lung transplant complications—both common complications such as pneumonia and rare but life-threatening complications such as torsion. Although great progress has been made since the 1960s, the mean life expectancy of lung transplant recipients lags behind that of other organ recipients at only 6–7 years after transplant [10]. Early complications account for much of the morbidity and mortality in lung transplant recipients. These complications must be accurately detected and described when interpreting imaging studies, and they should be taken into account when protocoling imaging studies for lung transplant recipients. By doing so, radiologists can contribute to the postoperative care of lung transplant patients and can help optimize the quality and the duration of their posttransplant lives.
ERRATA:The winter issue featured this article with production errors, including inadvertent unauthorized changes to the title, introduction, and figures 3 and 4. We regret these errors and have republished the complete, corrected article for clarity.
References
Organ Procurement and Transplantation Network, U.S. Department of Health & Human Services. National Data: Transplants in the U.S. by Region. optn.transplant.hrsa.gov/data/view-data-reports/national-data. Published 2024. Accessed August 25, 2024
Kim SJ, Azour L, Hutchinson BD, et al. Imaging course of lung transplantation: from patient selection to postoperative complications. Radiographics 2021;41:1043-63
Masson E, Stern M, Chabod J, et al. Hyperacute rejection after lung transplantation caused by undetected low-titer anti-HLA antibodies. J Heart Lung Transplant 2007;26:642-45
Shah RJ, Diamond JM. Primary graft dysfunction (PGD) following lung transplantation. Semin Respir Crit Care Med2018;39:148-54
Snell GI, Yusen RD, Weill D, et al. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction, part I: definition and grading – a 2016 consensus group statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant 2017;36:1097-1103
Adelmann D, Koch S, Menger J, et al. Risk factors for early bleeding complications after lung transplantation – a retrospective cohort study. Transpl Int 2019;32:1313-21
Kim SJ, Short RG, Beal MA, et al. Imaging of lung transplantation. Clin Chest Med 2024;45:445-460
Amadi CC, Galizia MS, Mortani Barbosa EJ Jr. Imaging evaluation of lung transplantation patients: a time and etiology-based approach to high-resolution computed tomography interpretation. J Thorac Imaging 2019;34:299-312
Verleden GM, Glanville AR, Lease ED, et al. Chronic lung allograft dysfunction: definition, diagnostic criteria, and approaches to treatment – a consensus report from the pulmonary council of the ISHLT. J Heart Lung Transplant 2019;38:493-503
The American Roentgen Ray Society (ARRS) is pleased to announce Francis Baffour of Mayo Clinic in Rochester, MN, as the 2024 Melvin M. Figley Fellow in Radiology Journalism. ARRS also recognizes Hyun Soo Ko of the Peter MacCallum Cancer Centre and Epworth Medical Imaging in Melbourne, Australia, as the 2024 Lee F. Rogers International Fellow in Radiology Journalism.
Supported by The Roentgen Fund® and named for two distinguished Editors Emeriti of ARRS’ own American Journal of Roentgenology (AJR), the Melvin Figley and Lee Rogers Fellowships offer practicing radiologists an unparalleled opportunity to learn the tenets of medical publishing via “the yellow journal”—the world’s longest continuously published radiology journal. Through hands-on experience with ARRS staff and AJR personnel—as well as personal apprenticeship with AJR’s 13th Editor of Chief, Andrew B. Rosenkrantz—Drs. Baffour and Ko will receive expert instruction in scientific writing and communication, manuscript preparation and editing, peer review processes, journalism ethics, and both print production and digital publication.
Founded in 1907, AJR is one of the specialty’s leading peer-reviewed journals, publishing clinically oriented content across all imaging subspecialties and modalities relevant to radiologists’ daily practice. Overall, “the yellow journal” garnered 35,480 citations in 2022, ranking AJR fourth among all radiology journals.
Since 1990, The Roentgen Fund has granted millions of dollars to hundreds of imaging professionals for both research pursuits and professional development. Today, through six vital scholarship and fellowship programs, the generosity of The Roentgen Fund’s donors is channeled to every corner of the globe—establishing dual foundations in innovation and leadership for a true diversity of radiology’s next generation.
Francis Baffour practices as a diagnostic radiologist with expertise in advanced MRI and CT techniques for musculoskeletal imaging. His clinical and research interests align with his goal of identifying novel applications for advanced imaging technologies, then rapidly translating these discoveries into practical patient care. As associate medical director of the CT Clinical Innovation Center in Mayo Clinic Rochester’s department of radiology, he supports the mission of facilitating high-impact imaging innovations with direct effect on patients, such as radiation dose reduction techniques, novel CT technologies, and quantitative assessment of disease activity. Dr. Baffour earned his M.D. from the Albert Einstein College of Medicine in New York City and a B.A. in biochemistry from Vassar College in Poughkeepsie, NY.
A German and Australian board-certified radiologist with over 20 years of international experience, currently, Hyun Soo Ko practices at Peter MacCallum Cancer Centre and Epworth Medical Imaging in Melbourne, Australia, holding affiliations with the University of Melbourne and University of Bonn in Germany. Her expertise is diverse, with specialized fellowships in breast imaging (Melbourne), imaging research (Toronto), and pediatric radiology (Heidelberg, Germany). Dedicated to advancing translational medicine, her research focuses on AI and radiomics to discover predictive imaging biomarkers. She is an active member of the Royal Australian and New Zealand College of Radiologists (RANZCR) Advisory Committee on Artificial Intelligence and the German Roentgen Society (DRG) Working Party Methodology and Research. As a clinician researcher, Dr. Ko remains committed to mentoring and supporting emerging radiologists, firmly believing multidisciplinarity and inclusiveness are key elements for equitable progress and impact.
From May 5–9, 2024, Drs. Baffour and Ko will attend the 2024 ARRS Annual Meeting in Boston, MA, where they will co-present the AJR Year in Review Sunday Session and participate in the Editor’s Forum.
More about the Figley and Rogers Fellowships
Melvin M. Figley (1920-2010) assumed the editorial mantle of AJR with the January 1976 issue. Hiring a full-time professional staff and, for the first time, a managing editor, he appointed associate editors to facilitate the peer review process. Publication accelerated, and the quality of illustrations improved, leading to the AJR Pictorial Essay. Dr. Figley was also central to the partnership between ARRS and the American Society of Neuroradiology, including the founding of the American Journal of Neuroradiology in 1980. After more than a decade of dedicated service to “the yellow journal,” Dr. Figley retired in 1985.
Lee F. Rogers, the distinguished musculoskeletal radiologist and longtime chair of imaging at Northwestern University Medical School, was named AJR’s chief editorial officer in 1996. Highlights from Rogers’ tenure at the journal included more contemporary design, introducing of a medicolegal column, authored by Dr. Leonard Berlin, and his popular editor’s notebook. Both the quality and the variety of papers published in AJR remained quite high, as the information revolution propelled “the yellow journal” into new formats, such as CD-ROM, and frontiers, like the internet.
Five prior Melvin M. Figley Fellows of The Roentgen Fund® will also present during the 124th ARRS Annual Meeting in Boston, MA:
In radiology, whether you work in a large or small private practice, remotely by yourself, an academic department in a medical center, or part of a mega radiology practice, there has been a palpable shortage of radiologists. This shortage is fueled by a trend toward exclusive subspecialization with declining numbers of radiologists who can handle general work, ever-increasing expectations for service to our patients, referring doctors, hospitals, and health care systems. We have been stretched thinner. There is a desire by radiologists to have more flexible work hours or, simply stated, to work less hours overall compared to years past. There is a concern about what role artificial intelligence and machine learning will play; will we be displaced? Reimbursement has been decreasing relative to inflation and compared with other specialties. As a result of these realities and others, there is clear evidence of burnout among radiologists, similar to health care workers in other specialties. On top of that, sometimes, we find that the leaders in our organizations may be distant, or too corporate, or suffer from “toxic positivity,” which may be worse than “toxic negativity.”
There has been a steady headwind for years, but it now feels like a gale force wind. And a lot of this feels out of our control. So, goodness, how do we manage all of this? Hold on, let’s take a breath. One strategy that we can embrace and control is to develop a culture of teams within our workplaces. In fact, I have titled this series “The Teamwork Imperative” because we must establish teamwork as a core value within the radiology workforce. I believe that if we foster a culture of teams, we can mitigate and shield ourselves from some of these headwinds.
Let me be clear. Here, when I say teams, I am specifically not referring to the “macro teams” that many of us find ourselves in. For example, at Duke Health, it is said that the 30,000-plus employees are my “teammates.” That very well may be true. But no, I am referring to your local and focal team. I am referring to the individuals that you rely on daily or weekly to deliver your work product. It’s the folks you huddle with. And the teams develop where you huddle. If you are in training, I am referring to your team of co-residents, your chief residents, maybe your program director or program coordinator who you lean on. If you are in a private practice, I am referring to those that you share physical space with, or perhaps switch call with, or the individuals you show difficult cases to, or the referring docs you have developed close relationships with, and who rely on you to deliver care. In an academic environment like mine, it might be the members of your subspecialty division. If done well, the division pulls together as a team to deliver care, service, teaching, and research.
Those divisions that have a culture of team are far more effective than those who are unable to act as a team. If you are lucky enough to have these local and focal teams (and these often form and evolve organically), many challenges at work open up and become more manageable and attainable. The clouds begin to lift. Specifically, your deliverables, whatever they may be, are far more easily and effectively achieved if you have your team and approach your work from the perspective of that team.
Work becomes more efficient and fulfilling and, frankly, more fun. The work becomes more manageable, with more aspects under your control. You become more engaged. And that then becomes an antidote to burnout. Teams, therefore, contribute to retention.
Coaches discuss this all the time. I’ll borrow here from Mike Krzyzewski, the legendary Duke University men’s basketball coach. “Coach K” famously talked about the five keys to an effective team, likening them to the fingers on a hand. Each finger is individual and can stand alone, but when the five fingers of communication, trust, responsibility, caring, and productivity come together into a fist, the fist proves to be much stronger than the sum of the individual fingers.
Communication
Yes, of course, communication is about sharing news back and forth, accurately and honestly, but more importantly, communication is to be able to probe, to be able to respectfully question, and to be able to expect honest answers from your teammates. Sometimes, the questions aren’t easy, and the answers may not be easy either. To foster an effective team requires the ability and the safety of pointing out the opportunities—those ones are easy. More importantly, it is to have safety in pointing out deficiencies—those are more difficult. It is critical for teammates to be able to receive and internalize the information coming from within the group, whether it is a kudo, an observation, or a deficiency or a criticism.
You have to talk to each other. Actually talk. And in a world of remote work and texting, we don’t talk enough. Maybe the talking occurs in a partner meeting, defined clinical case conference, resident meeting, or division or department meeting. Maybe it is your team taking a coffee break or going for a midday walk to achieve “step” goals. Hopefully, the team dynamics are such that one can tap a teammate on the shoulder and engage in an effective and safe conversation.
Communication needs to be practiced. That is why I think standing, regular, in-person meetings, even if the agenda is light, are very important. The opportunity to come together regularly promotes the importance and expectation of communication. And it is habit forming. You get better at it.
Trust
Trust means telling the truth, and telling it sooner rather than later; knowing that within a team, that can be hard. It can be hard because so many of us struggle with confrontation and conflict and try to avoid them. But consider it this way, from the perspective of the iconic University of Tennessee women’s basketball coach, Pat Summitt. She said, “The absolute heart of loyalty is to value those people who tell you the truth, not just those people who tell you what you want to hear. In fact, you should value them the most, because they have paid you the compliment of leveling with you, assuming you can handle it.”
Honest and fair difficult conversations almost always produce results. If you can get through the first thirty seconds of a difficult conversation, often the clouds lift and a very productive conversation follows. For me, I need to write down the key first few sentences for that opening thirty seconds and the rest flows. If difficult conversations don’t produce results, you have learned something.
Collective Responsibility
A coach might say, “We win together, we lose together, there is no “blame game.” In the workplace of radiology, the collective responsibility is the pulling together to deliver on our various missions. Everyone does not play the same role. One partner may be a fast and efficient reader, that’s great. Her partner is slower because he spends a lot more time consulting and discussing with referring docs. Both these individuals are important to the team. Or in an academic environment, one may be more focused and skilled clinically, another may be more focused on teaching. In a team where there is collective responsibility, they complement one another and each can be proud of each other’s successes. Indeed, the light of their success shines on the other teammates, on the entire team.
Caring
This is also about humanity and human connections and colleagueship. Caring in a team reflects time spent with each other and sharing aspects of ourselves, in this case the women of Duke Radiology. The caring strengthens the interconnective web between team members, in this case at our annual Fall Gathering. It makes the team softer in a positive way, and more personable, yet, at the same time stronger.
Here is where I worry about remote work. I get it. The pandemic has shown that we can do radiology effectively, even remotely. People like it and expect it. And we have learned that we can teach remotely. Sort of. But it seems far more difficult to foster a genuine, caring environment when work is dispersed in many geographic locales and individuals work essentially independently, free of meaningful, direct interactions with other teammates, other humans. To me the same applies to Zoom meetings. All the nuanced talk and greetings pre- and post-meeting are lost. The body language is lost. The sense of community is lost, or at least different. And I think the effectiveness of the meeting suffers. Indeed, on a Zoom meeting, you can’t even have real eye contact. I worry that with remote work, the culture of our teams maybe eroded. We do need to incorporate the best aspects of some remote work, but incorporate it in a fashion that fosters caring.
Pride/Productivity
Coach K says, “Everything we do has our own personal signature on it…and if we all sign off on everything we do, then we have a chance to be great.”
And your teammates all do have the chance to add their personal touch and signature. Collectively then, we have the opportunity to harness the best of what we can be, and to be great, even with all that is facing us and challenging us in our current and future work environments. “And it is going to be hard; we all wait in life for things to get easier…when we are well staffed, when I pass the Boards, when I make partner, when the kids are older, when the pandemic is over … it will never get easier. What happens is, you handle hard better.” As pointed out by Kara Lawson, Duke women’s basketball coach.
Each of these domains, communication, trust, collective responsibility, caring, and pride; the five individual fingers are important. But when the five fingers are formed into a fist, a true team, the collective strength is much greater than the sum of the individual parts. When these five areas can be applied to our teams in radiology, we can become more effective and efficient. As individuals alone, we are relatively weak. Together as a team, we are stronger. And this is something within our control.
To me, there is an imperative to create, sustain, and grow teams in our workplace.
Colleagues, I personally invite you to join us for ARRS 2024, either in Boston or online. This exceptional event brings together top radiologists from around the world to share new knowledge shaping our field.
Our Annual Meeting is renowned for its cutting-edge education, providing clinical information you can put into practice right away. We are excited to share the latest advancements in radiology, along with comprehensive review lectures to stay sharp on core topics.
Whether you attend in person and immerse yourself in the vibrant atmosphere of Boston, or choose our convenient online option, ARRS 2024 promises to be a remarkable experience. Your participation and engagement will help us connect, learn, and advance radiology together.
Assistant Professor, Department of Diagnostic and Interventional Imaging McGovern Medical School, UT Health Houston
It is my pleasure to discuss a topic that holds a very special place in my heart—the patient experience in breast imaging. What makes this topic truly captivating is that it touches upon several areas that are significant to me: patient-centered care, team leadership, and wellness. But there is an interesting twist, and I would like to share that as well, because it’s a kind of secret passion that I’ve had for years. And that is my love for spas, just the unforgettable experience you can get during one of the most memorable stays in a hotel.
Now, you might be wondering how on earth these interests come together. How can these unrelated topics merge to create a health care experience that is as luxurious and comforting as a world-class spa getaway, while also providing exceptional patient care?
We’ve all been on the other side of the examination table. We can relate to that mixture of emotions when walking into a doctor’s office. Just think about it for a moment. What stands out in your memory from those visits? Was it the mountains of paperwork you had to fill out, the warmth of the receptionist’s smile, the chill in the examination room? Maybe it was the time you spent waiting or the multiple ongoing discussions with your insurance company. Hopefully, and more importantly, perhaps it was the actual conversation you had with your doctor. Did you feel rushed, or were you heard and understood with all your questions addressed? Too often in our fast-paced working world of technicians and radiologists trying to meet numbers and targets, we may forget that the patient is the very reason we’re in this profession.
Really think about it. The news of a potential cancer is something threatening, and it is understandable that patients are stressed and anxious from the moment they walk into our office. Why not try to make the best possible experience when patients need it the most, for when they’re the most stressed and worried in their lives?
This is where my love for hotels comes in. When I was a girl, I loved a TV show about a lady who would receive the best stays and treatments at five-star hotels in incredible places around the world. She would then share her experiences with viewers. I used to think that, one day, I could do what this lady did. Of course, I didn’t end up being like her, but as a breast imager and as a patient now, I have always liked to compare the health care industry with the hospitality business. Although going to the doctor is not all leisure or pleasure, it is part of our wellbeing, and we’re all going to need it at some point.
So, how do five-star hotels approach guest satisfaction and train their staff for this amazing service? These hotels are renowned for their exceptional customer service experience, and they invest heavily in preparing their staff. Please allow me to share a few of these key elements that I think we could borrow from their playbook. Thankfully, some of them we are already incorporating as radiologists.
Let’s start with a customer-centric philosophy. Just as in five-star hotels, we should prioritize patient satisfaction above everything else. Every interaction with a patient should reflect our commitment to their wellbeing. This is exactly what the American College of Radiology’s Imaging 3.0 initiative is all about.
Then, we have role-specific training. As hotels do, health care should provide training that is tailored for specific positions, whether it’s radiologists, technicians, or administrative staff. Everyone should receive training that is aligned with their responsibilities. Those of us who are in academic institutions, for example, should model and objectively evaluate the interactions between our trainees and our patients to identify potential areas for improvement.
I want to continue with empathy and emotional intelligence. This might be a hard one, but we can train our health care professionals to empathize with patients’ needs and emotions. Recognizing and responding to patients’ moods can lead to a more compassionate and effective health care experience.
Next, we have language and communication, which is very important. In our diverse world, especially in the United States, language training is crucial for health care professionals. Being able to communicate effectively with patients from various backgrounds is going to enhance trust and understanding.
I’ll continue with problem-solving and decision-making. Similar to how hotel staff practice handling several guest scenarios, our health care professionals can benefit from training that sharpens problem-solving and decision-making skills, ensuring they can address patient concerns effectively and promptly.
Ongoing training. I think we’re good at this one. Learning in health care should not be a one-time event. Continuing education and professional development opportunities are not only going to keep our staff updated, but will also keep them committed to the patient experience.
Finally, we have guest feedback. Like hotels—now with Yelp and Google reviews—we should actively seek patient feedback. Comments, both positive or negative, are going to be valuable for improvement.
Let’s connect all of this back to breast imaging. In diverse cities (for example, Houston, TX), diversity among our medical professionals and staff becomes essential. Having tools for communication, like translators, is helpful. More notably, having health care professionals who speak a patient’s language and share their culture creates an immediate sense of connection and trust, just as in five-star hotels.
We know that trust is the foundation of an excellent patient-radiologist relationship, ensuring they return to us for essential care; however, establishing that trust is not the radiologist’s job alone. Since we are often the last ones to see a patient, our front desk and technician staff set the tone for what the patient’s visit will look like. We all need to be on the same page, so periodic meetings and reminders about our goals in terms of patient experience are necessary.
Most importantly, we must not forget about our own wellbeing as health care professionals. And this is where administrators come in. Burnout, unfortunately, is a critical concern for radiologists. It affects our ability to provide the best care possible. We must set clear and appropriate boundaries in scheduling to prevent our staff from becoming overwhelmed and exhausted.
I know there are times when we must go above and beyond, but this should not be the baseline. If we have burned out staff, we cannot deliver the exceptional patient care and experiences we are aspiring to provide. I do feel like our role as breast imagers extends beyond our technical expertise and medical knowledge. We should create an environment where our patients feel valued, heard, and cared for. Borrowing some of these insights from the world of five-star hospitality, promoting diversity, and ensuring staff wellbeing, we can sincerely elevate the patient experience. Remember, it’s not only about what we see on the screen or the images we interpret, but how we make our patients feel through their health journey. We want this experience to be what they remember from their visit.
@RHWiggins Associate Dean of CME Professor of Radiology and Imaging Sciences University of Utah Health Science Center
Subdivided at the hyoid bone, the soft-tissue core of the extracranial segment of the head and neck can be divided further into two discrete areas: the suprahyoid neck and the infrahyoid neck. Whereas the infrahyoid portion lies inferiorly between the hyoid bone and clavicles, the suprahyoid area comprises the deep spaces between the base of the skull and the hyoid bone. While decades ago, lesions in the deep suprahyoid neck lead to a vague report listing a long differential diagnosis, an understanding of the suprahyoid neck anatomic space can lead to an accurate space-specific differential diagnosis. Here, three layers of cervical fascia help to define all the separate spaces in the deep part of our face.
Presented live on Sunday, April 16 during the 2023 ARRS Annual Meeting in Honolulu, HI, our “The Suprahyoid Neck—Pathology Through Anatomy” Featured Session will focus on reviewing important anatomical subunits and common pathologies of the suprahyoid neck: the parapharyngeal, pharyngeal mucosal, masticator, parotid, carotid, retropharyngeal, danger, and perivertebral spaces (Fig. 1).
Fig. 1—Axial drawing depicts relevant anatomy of paramaxillary and submastoid approaches. In submastoid approach, needle takes approach that is out of axial plane to pass caudal to mastoid process. Approximate location of seventh cranial nerve as it courses inferior stylomastoid foramen is labeled.
Examining imaging findings crucial for diagnostic radiologists and neuroradiologists alike to identify, attendees will enhance their clinical performance through a greater, more holistic understanding of cross-sectional anatomy and common pathologies that lead to various lesions in these regions—each a critical check point for accurate interpretation of radiological studies of the suprahyoid neck.
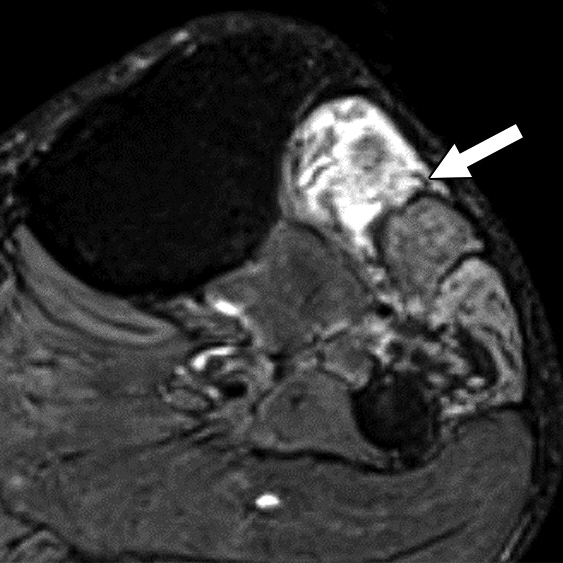
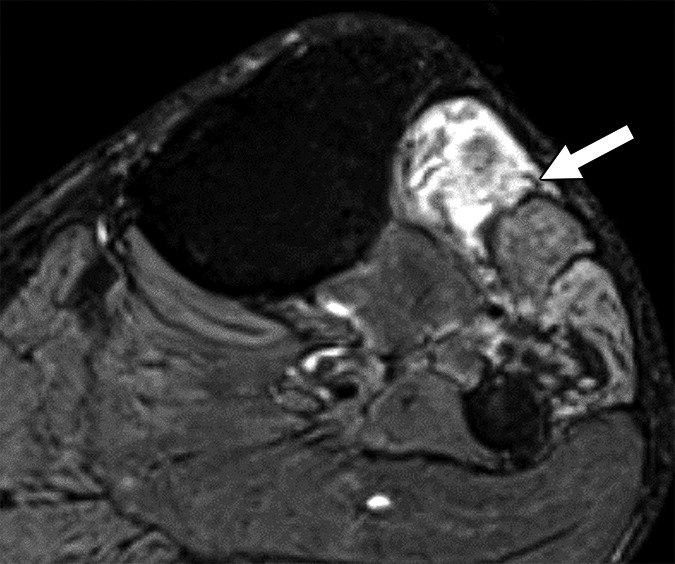
Speaking of studies, our illustrious Featured Sunday Session faculty are especially looking forward to leading breakout sessions regarding the various modalities most frequently found in imaging the suprahyoid neck. The comparative insensitivity of CT for artifacts, CT’s more comprehensive delineation of facial structures, and the promise of contrast-enhanced images to reveal critical vasculature continue to make CT more advantageous than ultrasound guidance (Fig. 2).
Fig. 2—72-year-old with right facial and neck pain and dysphagia associated with 7.7-kg (17-lb) unintentional weight loss. Left: Axial contrast-enhanced CT image of neck shows incidentally identified soft-tissue mass centered in right deep parotid space. Right: Axial CT image obtained with patient positioned with his head angled contralateral to lesion. Needle is advanced percutaneously, caudal to mastoid tip and through sternocleidomastoid muscle. It is then advanced with tip oriented cranially for access to parotid lobe lesion.
And because CT-guided fine-needle aspiration and biopsy can be performed with patients in three positions (supine, prone, lateral decubitus), multiple clinical studies in the imaging literature continue to conclude that this procedure remains safe and effective for obtaining tissue to diagnosis lesions of the head and neck. For quick reference, we encourage you to consult the following preprocedural patient care checklist for fine-needle aspiration and/or biopsy to help promote a professional and efficient imaging encounter with your patients:
Procedure
Relevant to ongoing care?
Anesthesia
Moderate sedation available?
General anesthesia more appropriate?
Consent Approval
Both procedure and sedation?
Imaging
Preprocedural images available for review?
Positioning
Planned trajectory verified?
Patient able to tolerate?
Lab Results
Values within acceptable ranges?
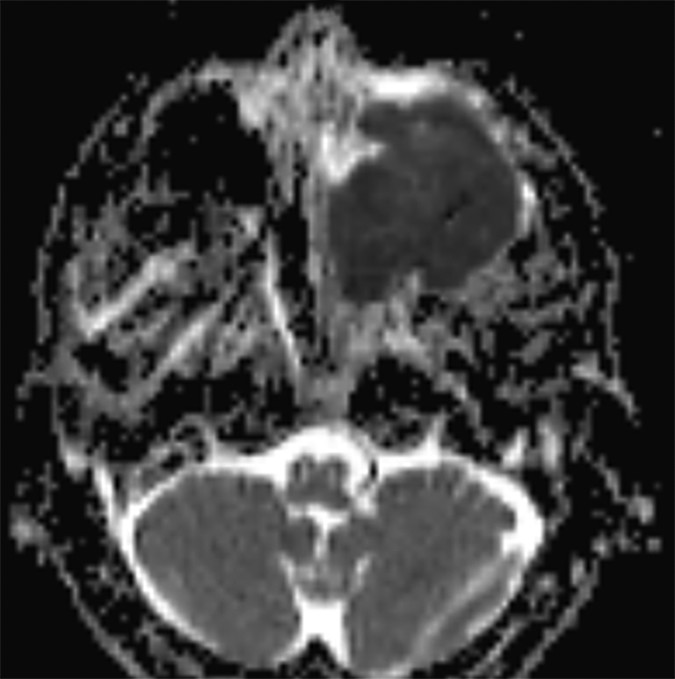
In certain instances, diffusion pulse sequences can offer a complementary adjunct to conventional MR pulse sequences, but neither diffusion-weighted imaging (DWI) or diffusion tensor imaging (DTI) should be utilized as a standalone technique for characterizing the benignity of head and neck lesions. Moreover, since mean apparent diffusion coefficients (ADC) values derived from DTI parameters are characteristically lower than ADC values developed from DWI parameters—frequently lower than reported malignant threshold values—the two should not be used interchangeably (Fig. 3).
Fig. 3—48-year-old with sinonasal neuroendocrine carcinoma. Left: Mass appears bright on diffusion-tensor imaging trace image (left) and dark on corresponding apparent diffusion coefficient (ADC) map (right), consistent with reduced diffusivity in high cellularity lesion.
With personalized, precision medicine becoming increasingly more critical for our patients in today’s value-based health care environment, the topic of the suprahyoid neck is particularly timely for medical imagers at all professional levels and of every practice type, notably so for head and neck radiologists, neuroradiologists, and in-training imagers of both subspecialties. Closely working alongside head and neck surgical teams—often on complex cases of deep space neck masses with widely differential diagnoses—practicing radiologists must intimately understand each significant space of the suprahyoid neck, as well as their surrounding fascial boundaries.
Unique in the quality of the educators and the breadth of the curriculum, our “The Suprahyoid Neck—Pathology Through Anatomy” live event from Oahu Island on Sunday the 16th will also address key concepts for radiologists to improve their accuracy in reporting complex imaging cases. A key didactic point will be how a better understanding of suprahyoid neck anatomy can lead the imager to a space-specific differential and diagnosis. Once again, just as we concluded the ARRS “Temporal Bone Imaging Made Easy” symposium this March, I will then review top points from all the earlier expert presentations. We will officially adjourn after another spirited Q&A block, allowing faculty to address individual questions regarding both anatomical and pathological considerations when imaging the suprahyoid neck spaces.
The Upper Aerodigestive Tract
Also presented live on Sunday, April 16 during the 2023 ARRS Annual Meeting in Hawaii, our “The Upper Aerodigestive Tract” session will review essential anatomy and pathology of this tract surrounding the suprahyoid neck spaces. Each subunit of the upper aerodigestive tract will be examined, including the nasal cavity, nasopharynx, oral cavity, oropharynx, larynx, hypopharynx, cervical trachea, and cervical esophagus. Esteemed faculty for this Featured Sunday Session have prepared clinically focused sessions on important anatomical subunits, examining cross-sectional anatomy and pathology findings that are critical for the head and neck radiologist to understand for each region. Participants will enhance their performance by gaining a greater understanding of common pathologies that occur, honing in on critical check points for accurate interpretation of head and neck imaging studies of the upper aerodigestive tract, which is critical for certain pathologies—especially so for squamous cell carcinoma.
As an instructional topic for medical imaging professionals, the upper aerodigestive tract is timely in today’s health care environment, too. Awareness and appreciation of the many issues that can arise are indispensable to rendering better health care for our patients. Specifically, when collaborating with head and neck surgeons on non-cutaneous head and neck squamous cell carcinoma cases, it is the imaging that determines the staging—and, therefore, the therapy—in these complex cases.
Similar to our “The Suprahyoid Neck—Pathology Through Anatomy” course on the same day, an overall primer on critical spaces will be presented first, before diving into the more detailed subunit lectures our experts have prepared. Once more, each region of the upper aerodigestive tract will be assessed in functional terms alongside normal imaging findings, followed by a thorough analysis of pathologies for common head and neck cancers, as well as important mimics and differentials.
@AChhabraMD Professor of Radiology Chief of Musculoskeletal Imaging UT Southwestern Medical Center Parkland Health & Hospital System
Collectively, ultrasound, electromyography, and even physical findings play a role in diagnosing anomalies of the peripheral nervous system. Increasingly, though, MR neurography (MRN) is becoming very common for the evaluation of peripheral neuropathy. This enhanced adoption is due to technological advancements in imaging quality and acquisition speed, such as newer 3D techniques, improved coil equipment, sparser k-space sampling, and compressed sensing, etc. In fact, in today’s tertiary care setups, MRN is being quickly incorporated for the workups of peripheral neuropathy and plexopathy patients, due to both need and ask from the peripheral nerve physicians, orthopedic surgeons, and pain management specialists. Although many articles about the evolution of MRN have been published in the clinical literature, thus far, no standards for the evaluation and recording of peripheral nerve pathologies on MRI have been acknowledged, much less validated.
Our retrospective study included 100 patients with nerve imaging examinations and a variety of known clinical diagnoses. Utilizing mutually agreed-upon qualitative benchmarks for classifying and grading peripheral neuropathies, different classes were established to account for the spectrum of underlying pathologies (unremarkable, injury, neoplasia, entrapment, diffuse neuropathy, not otherwise specified, and postintervention state) with subclasses to describe lesion severity or extent. Validation was performed by 11 fellowship-trained musculoskeletal radiologists across 10 institutions, and after initial multimedia training, all 100 cases were blind-presented to readers (Fig. 1).
Fig. 1—Neuropathy Score Reporting and Data System (NS-RADS) subclass I3 M2. Axial fat-suppressed T2-weighted (left) and T1-weighted (right) images show extensor compartment and peroneal compartment denervation changes with fatty infiltration, edemalike signal, and mild atrophy (arrows) consistent with NS-RADS subclass M2.
Offering a uniform lexicon and practical guideline for reporting neuropathic conditions on MRI, ultimately, NS-RADS accuracy for determining milder versus more severe categories per radiologist ranged from 88% to 97% for nerve lesions and from 86% to 94% for muscle abnormalities (Fig. 2).
Fig. 2—Neuropathy Score Reporting and Data System (NS-RADS) subclass M1. Axial T1-weighted (left) and STIR (right) images depict denervation edemalike signal of extensor muscles of dorsal and mobile wad compartments with no fatty infiltration or atrophy, consistent with NS-RADS subclass M1. (Arrows in right show edemalike signal of muscles.)
On the basis of the overall promising interrater agreement shown in this study, we believe that the newly proposed NS-RADS classification will perform as well in routine practice as it did in this initial validation study (Fig. 3).
Fig. 3—Neuropathy Score Reporting and Data System (NS-RADS) subclass E2 M0. Axial (left) and oblique coronal (right) fat-suppressed T2-weighted images show proximally enlarged and hyperintense ulnar nerve (arrows) and normal nerve caliber distal to cubital tunnel (arrowhead on right).
However, we must acknowledge several barriers that still exist for learning and successful incorporation of routine MRN in radiology practices:
lack of widespread usage of technology, especially information on recent advancements
optimization for different tissue resolutions
complexity of peripheral nerve anatomy
uniformity of reporting with multidisciplinary teams
paucity of knowledge about diagnostic imaging criteria for lesion classification—something NS-RADS intends to correct
NS-RADS Details at ARRS Annual Meeting in Hawaii
Presented live during the 2023 ARRS Annual Meeting in Honolulu, HI, “MR Neurography and NS-RADS: Assist Your Neuropathy and Pain Patients” will focus on the latest advances in MRN and its practical application in routine imaging practice. Pertinent for practicing radiologists, musculoskeletal and neuroradiology subspecialists, fellows and residents in diagnostic radiology, and even radiologic technologists, six experts in MRI protocol and sequence design will deliver a two-hour categorical session. This session has been expertly curated, covering one anatomic site at a time. The majority of our lectures will be nerve-focused—reviewing and updating NS-RADS and detailing innovative MRN techniques for brachial plexus, LS plexus, facial, intercostal, as well as peripheral nerves. Our panel will also address 2D vs. 3D MRI correlations, highlighting relative advantages and disadvantages of different sequences.
Moving forward, modern MRI readers need to be fluent in the latest MRN features of different neuropathies, as well as related syndromes and classifications. We will also discuss current research projects and future applications. By incorporating these imaging interpretation criteria and expert insights from different tertiary care institutes, imaging professionals can impact diagnostic strategies, thus altering management decisions of neuropathy patients for improved outcomes.
Every year, medical students, early in their educational journeys, are encouraged by deans and other high-ranking medical school administrators to consider primary care (internal medicine, family medicine, or pediatrics) as a career choice. Most of us chose a different, more specialized route and wound up in radiology.
Now, I would like to encourage you to be a primary radiologist. By saying primary radiologist, I am not encouraging you to go into primary care, but rather to be the best radiologist that you can be. Primary radiologists are leading radiologists—working at a very high level, communicating clearly and effectively with referring physicians and patients, and keeping up to date with new developments in imaging and medicine. Most practices or groups have a primary radiologist—the highly accurate radiologist who is consulted on the most difficult cases and who is always available to help.
The primary radiologist’s role is based heavily on earning the respect of others. A primary radiologist is the one you and others turn to when you need an expert opinion. Oftentimes, a colleague will ask, did you show the case to Dr. _____? Alternatively, one may want an opinion on how Dr. _____ would approach a difficult procedure.
It is difficult to be a primary radiologist. There are ongoing global stressors, like the COVID-19 pandemic, and stressors affecting radiologists, including high burnout rates and an ever-increasing workload. Bhargavan et al. noted that when 2006–2007 data was compared to 2002–2003 data, the annual workload per full-time equivalent radiologist increased by 7%. When 2006–2007 data was compared to data from 1991–1992, the annual workload per full-time equivalent radiologist increased by 70.3%! Now, 2006–2007 seems like a long time ago, and, undoubtedly, workloads have continued to rise over the last 15 years.
How do we become primary radiologists in the current milieu? When we think of doing a great job, we need to define success. Success may be defined differently by deans, hospital administrators, chairs, section heads, and individual radiologists. As many of us are working very hard these days, it makes sense to think about what success means. John Wooden served as the basketball coach at the University of California, Los Angeles (UCLA) from 1948 to 1975. During that time, he led the UCLA Bruins to 10 National Collegiate Athletic Association (NCAA) basketball championships. I like John Wooden’s definition of success. Coach Wooden stated that “success is peace of mind which is a direct result of self-satisfaction in knowing you did your best to become the best that you are capable of becoming.”
In Coach Wooden’s Pyramid of Success, industriousness and enthusiasm are major cornerstones. Regarding industriousness, I don’t see radiologists’ workloads diminishing any time soon. In our current world of radiology, I agree with Coach Wooden, who noted that “there is no substitute for work. Worthwhile results come from hard work and careful planning.” When discussing planning and preparation, Coach Wooden stated that “failing to prepare is preparation for failure.” This important maxim applies to individual cases and procedures, as well as to our overall growth and development.
As we strive to be primary radiologists, our continued growth and development is based on self-assessment and identifying educational opportunities to rectify our perceived deficiencies. As we head into a new academic year and try to find top-notch educational content to fill our gaps, I suggest looking into the vast portfolio of educational offerings from our American Roentgen Ray Society. On ARRS.org, you will find information on the 2023 ARRS Annual Meeting in Honolulu, Hawaii, upcoming Live Symposia, Online Courses, Web Lectures, Quick Bytes, and Global Partner Education, including American Journal of Roentgenology (AJR) articles with credit, AJR Webinars, Author Videos, Podcasts, Tweetchats, Visual Abstracts, and much more. Whatever you are looking for, it is very likely that you will find it on the ARRS website and various social media channels.
In our quest to become primary radiologists, a key ingredient is enthusiasm. Coach Wooden noted that enthusiasm “brushes off upon those with whom you come in contact.” He continued, noting that “you must truly enjoy what you are doing.” Being enthusiastic about an unrelenting onslaught of work can be challenging, but we should try to be enthusiastic toward those who really need our services—our patients and our referring providers—and our team members. In general, our teams will function at a higher level if we treat everyone with enthusiastic, professional respect.
In addition to enthusiasm and industriousness, I think that in today’s topsy-turvy world, adaptability is critical. If we are going to be at the top of our game and really be the primary radiologists that we are capable of becoming, we must be able to adapt to new and sometimes unforeseen situations. Coach Wooden defined adaptability as “being able to adjust to any situation at any given time.” Just think of how different October 2019 (pre-COVID) was compared to March 2020 (early in the COVID-19 pandemic). The first COVID-19 outbreak was reported in Wuhan, Hubei, China in November of 2019, and by March 11, 2020, we were involved in a major pandemic with 118,465 confirmed cases of COVID-19 and 4,295 deaths worldwide. As we enter a new academic year, I want to encourage you to be the best radiologist that you can be—to be your best version of a primary radiologist. It won’t be easy, but with industriousness, enthusiasm, and a lot of adaptability, I think that we can do it and enjoy the journey!