
While ultrasound (US) remains the cornerstone of fetal screening due to its safety, real-time capabilities, and cost-effectiveness, occasionally, it meets its limits, too. In these instances, fetal MRI acts as a targeted problem-solving complement rather than a replacement, providing the clarity needed for high-stakes clinical decisions.
Safwan Halabi, MD, speaks with AJR Podcast Series host Raisa Amiruddin, MBBS, on techniques for detailed imaging of the developing fetus and the role of radiologists in the multidisciplinary fetal medicine team.
MRI Steps In: MRI is most frequently utilized when US raises questions that require deeper characterization in the following areas:
- CNS Anomalies—MRI excels at evaluating the fetal brain, offering superior soft tissue contrast to visualize intricate details of cortical development, the corpus callosum, and posterior fossa structures.
- Prognostic Quantification—For conditions like congenital diaphragmatic hernia, MRI provides precise measurements of fetal lung volume, which is a critical predictor of postnatal outcomes and candidacy for fetal surgery.
- Complex Fetal Masses—In cases of masses like sacrococcygeal teratomas, MRI clarifies the internal composition and relationship to adjacent structures, which is essential for surgical and delivery planning.
Technical Hurdles: One of MRI’s greatest strengths is its independence from the technical limitations that often challenge US. MRI quality is not degraded by:
- Fetal position or maternal body habitus
- Low levels of amniotic fluid (oligohydramnios)
- Maternal positioning, as mothers can often be adjusted within the scanner for comfort
Safety and Field Strength: Safety is a primary concern for expecting parents, of course. Routine fetal MRI uses no ionizing radiation and is performed without IV contrast, eliminating additional exposure concerns.
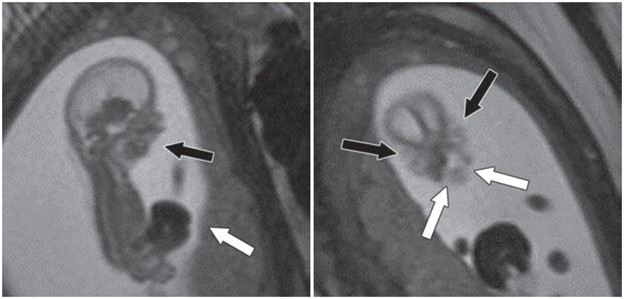
Fetus at gestational age of 13 weeks 0 days evaluated by MRI at 3T to characterize multiple congenital anomalies. Left, Sagittal 2D balanced SSFP image through entire fetus shows anterior abdominal wall defect with exteriorized liver (white arrow) and micrognathia (black arrow). Right, Coronal 2D balanced SSFP image through fetal face shows bilateral cleft lip and cleft palate (white arrows) and hypertelorism (black arrows). Additional anomalies depicted by this fetal MRI examination (not shown) included bilateral cerebral ventriculomegaly measuring 10–11 mm and severe dextroconvex thoracolumbar scoliosis. Umbilical cord length was normal, arguing against limb–body wall complex despite presence in this case of numerous typical diagnostic elements of this condition.
While 1.5T has been the standard, many centers are transitioning to 3T MRI for its improved SNR and spatial resolution, particularly for early-gestation anatomy. Recent research published in AJR provides further reassurance, showing no significant differences in neonatal growth parameters (e.g., birth weight, head circumference) between neonates exposed to 1.5T, 3T, or no MRI in utero.
Shailin Thomas, MD, discusses the AJR article by Danzer et al. supporting the safety of fetal MRI performed at 3T based on neonatal anthropometric measurements.
Bottom Line: Fetal MRI is most effective when part of a multidisciplinary team approach. Rads provide the diagnostic “missing link,” working with maternal-fetal medicine specialists, neonatologists, and pediatric surgeons to translate complex images into a clear plan for the family. By identifying whether an anomaly is isolated or part of a larger syndrome, MRI helps guide the timing and mode of delivery, ultimately reducing parental anxiety during a critical time.
Leave a Reply