
No matter what happens here, suffice it to say that it almost always begins in the scala chambers. Whether identifying pathology or planning for surgery, as Amy Juliano, MD, of Massachusetts Eye and Ear Infirmary and Harvard Medical School delineated in her ARRS Quick Byte, rads need to lend their own ear toward the scala tympani.
Three Examples: Understanding the compartmental anatomy of the osseous and membranous labyrinth allows rads to differentiate between tumors, inflammatory changes, and surgical targets.
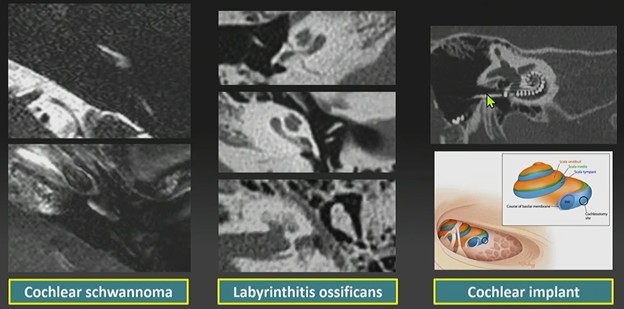
- Cochlear schwannoma: More often than not, these space-occupying, enhancing masses originate within the scala tympani. Contralateral comparison is key for detection.
- Labyrinthitis ossificans: This pathological calcification of the lumen often follows meningitis (frequently bilateral), trauma/fracture, or prior surgery. It predominantly affects the scala tympani. Working theory? White blood cell recruitment from specific vasculature predisposes this chamber to ossification.
- Cochlear implant: The surgical goal is to thread the electrode array into the scala tympani. Placing the implant in the scala vestibuli is a no-no.
Bottom Line: Look first and frequently at the scala tympani, as that’s where clinical and pathological significance alike most likely lies.
Leave a Reply