
Budd-Chiari syndrome is a disorder of hepatic venous outflow obstruction involving the accessory hepatic veins, major hepatic veins, or the suprahepatic inferior vena cava. Clinically, patients present with abdominal pain, hepatomegaly, and ascites—manifestations of sinusoidal congestion and portal hypertension.
The pathophysiology is straightforward: impaired venous drainage leads to hepatic congestion, rising sinusoidal pressures, and progressive liver dysfunction. However, as Baljendra S. Kapoor, MD, pointed out during this ARRS Quick Byte, the management algorithm is nuanced.
Baby Steps: Initial therapy is systemic anticoagulation. For patients with short-segment hepatic vein stenosis, balloon angioplasty with possible stenting is recommended, consistent with guidance from the American College of Gastroenterology.
When these approaches fail or are not feasible, the next-line intervention is Transjugular Intrahepatic Portosystemic Shunt (TIPS) placement. TIPS functions by creating a low-resistance channel between the portal and systemic venous systems, decompressing congested hepatic sinusoids and restoring effective outflow.
Recent Evidence: A meta-analysis of 1,395 patients published in JVIR demonstrated:
- 98.6% technical success
- 90.3% clinical success
- 0.5% TIPS-related mortality
These outcomes underscore both feasibility and safety. Much of the data derives from Asian cohorts, and randomized comparative trials remain limited, leaving questions about optimal patient selection and timing. Nonetheless, the existing evidence base supports TIPS as a highly effective salvage—and, in many cases, definitive—therapy.
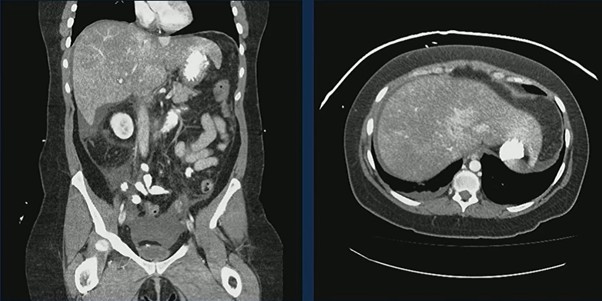
Case in Point: A 44-year-old woman with prior cerebrovascular accidents and paroxysmal nocturnal hemoglobinuria presented with abdominal pain, nausea, and vomiting. CT demonstrated an enlarged, heterogeneous liver with markedly heterogeneous enhancement and small-volume ascites—classic features of hepatic venous outflow obstruction.
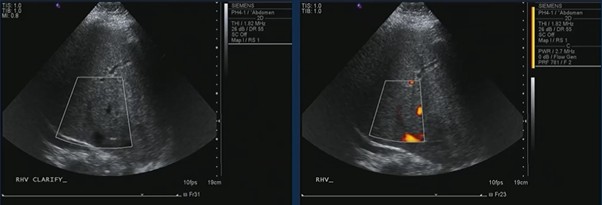
Ultrasound confirmed hepatic vein occlusion.
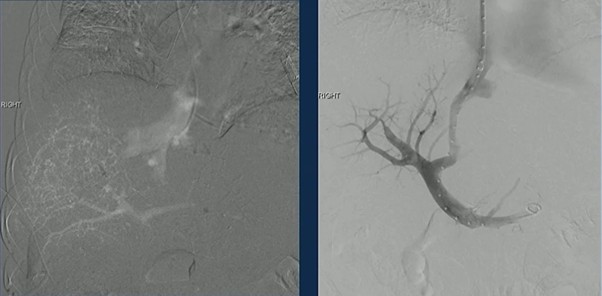
TIPS was successfully created, re-establishing outflow and decompressing the congested liver.
Clinical Inflection Point: Budd-Chiari management reflects a broader interventional principle…anticoagulate → recanalize, if possible → decompress, if necessary. For patients who fail medical therapy and angioplasty, TIPS is not merely palliative. It directly addresses the hemodynamic derangement driving symptoms and liver injury.
Bottom Line: Budd-Chiari syndrome is a vascular disorder with mechanical consequences. When hepatic venous obstruction persists despite anticoagulation and angioplasty, TIPS provides high technical success, strong clinical response rates, and low procedure-related mortality. In appropriately selected patients, decompression changes the trajectory of disease.
Leave a Reply