
This panel discussion from the ARRS 2024 Wellness Summit examined the factors that influence a well and safe day at work, and a well day of teamwork. This discussion provides an understanding of the impact of workload, the physical work environment, relational climate, and workflow on wellbeing.
Category: HFT Tools
-
Strategies and Solutions for Driving Wellness
Multiple peer-reviewed studies have consistently demonstrated a high prevalence of radiologist burnout. In this session from the ARRS 2024 Wellness Summit, practical strategies and solutions to improve radiologist workflow are described.
-

Empowering Families: Using Financial Freedom to Take Paternity Leave
I am the lucky father of three girls. Before the birth of my youngest daughter, my hospital emailed to let me know that I was entitled to 3 weeks of paid parental leave. I was ecstatic. However, as I looked into it further, I found out that I was actually entitled to 12 weeks off! There was one small catch: 3 weeks were paid leave, and 9 weeks were unpaid leave. Not only was it unpaid time off, but I would have to pay the hospital for continuing some of my benefits during that time. My initial instinct was that I should just take the 3 weeks.
As the date of my daughter’s birth approached, I started to rethink my priorities. For me, time with my family was more important at my early- to mid-career stage than the 9 weeks of salary. Also, my wife and I had saved an emergency fund of 6 months of expenses that we could easily access. What better way to spend that money than to have bonding time with my new daughter and help my older daughters make the transition to being older sisters to our new arrival.
Understanding the benefits and laws surrounding paternity leave in the United States, particularly the Family and Medical Leave Act (FMLA), is crucial. Moreover, having financial literacy and an emergency fund can make this transformative experience not just feasible, but enriching for families. In this blog post, I will explore the advantages of paternity leave, delve into the FMLA laws, and discuss how financial literacy plays a vital role in embracing this invaluable time off.
Paternity Leave Benefits
Bonding Time
Paternity leave allowed me to establish a strong emotional bond with my newborn daughter. Those initial months were invaluable for building connections that will last a lifetime. For my family with multiple children, the initial weeks involved a large change in family dynamics. Since my wonderful wife was very occupied with our newborn, I played a large role in helping my older daughters adjust to having a new member in the family, helping them embrace their new roles as older siblings, teachers, and helpers.
Support for Partners
My wife had some physical and emotional challenges after childbirth. During my paternity leave, I was able to support her and share many of the responsibilities that she was accustomed to doing. This allowed her to concentrate on our youngest daughter, helping the wellbeing of both my wife and my youngest daughter.
Time with Family
In our practice, it is very difficult to get a long period of contiguous time off. However, paternity leave offers this. During my leave, we were able to rent an Airbnb in Canada for 6 weeks. This allowed us to be very close to my dad and sister, which allowed for so much bonding time between my family and my daughters. It was the best part of the leave time. As members of a sandwich generation, my wife and I are caring for our children and our parents at the same time. It was great to be able to bring them together and spend an extended period of time together. A fantastic blog post titled “The Tail End” by Tim Urban and the Wait but Why team does a great job of explaining why such time is so precious! I highly recommend reading it.
Understanding FMLA Laws
The FMLA, enacted in 1993, enables eligible employees to take up to 12 weeks of unpaid, job-protected leave for specified family and medical reasons, including the birth or adoption of a child. Understanding these laws is crucial for fathers planning to take paternity leave.
Eligibility
FMLA applies to public agencies, public and private hospitals, and companies with 50 or more employees. To be eligible, an employee must have worked for the employer for at least 12 months and have completed at least 1,250 hours of service during the 12-month period preceding the leave.
Job Protection
One of the significant benefits of FMLA is the job protection it offers. Employees are entitled to return to their original or equivalent positions after the leave period, ensuring job security.
Health Insurance Continuation
During FMLA leave, employers must maintain the employee’s health benefits as if they were still working. During my leave, my hospital paid the employer contribution to the health plan premiums, and I was responsible for paying the employee portion of those premiums, as well as deductible and out-of-pocket costs.
Financial Independence and Emergency Fund
While the FMLA provides job protection, it is unpaid leave, which can pose financial challenges for unprepared families. Having an emergency fund can bridge this gap.
Peace of Mind
An emergency fund provides peace of mind, knowing that there’s a financial cushion to support the family during the paternity leave period.
Focus on Family
Financial stability allows fathers to focus entirely on their families—without the stress of immediate financial obligations. It empowers them to be present, both physically and emotionally, during this crucial time.
Future Planning
Financial independence encourages families to plan for the future. It ensures that the leave period doesn’t impact long-term financial goals, providing a sense of security for the entire family.
I am very lucky to work with amazing, supportive colleagues. When I proposed taking paternity leave, even though no one had done it before, I was met with support from my department, hospital, and colleagues. Another unique benefit to my leave? I was able to take it intermittently during the first year of my daughter’s life. This flexibility allowed me to work when we had visiting family in town, who could help, then take leave when it was just my wife and me. However, the present FMLA law does not require such accommodation, so this is likely employer-dependent. Now, I talk to all fathers who are expecting new babies about establishing an emergency fund, pointing out the benefits of more paternal leave. Anecdotally, this seems to be gaining traction among physicians. I know two recent father doctors who are taking their full allotment of paternity leave, as well as another father who is strongly considering taking some unpaid leave.
I believe that paternity leave (supported by laws like FMLA) is not just a break from work; it’s an investment in your family and the future. Understanding these laws and ensuring financial stability through an emergency fund can transform this period into a beautiful and enriching experience for fathers, mothers, and children alike. By embracing paternity leave and advocating for supportive policies, we contribute to the creation of healthier, happier families and a more balanced society.
Sherwin Chan, MD, PhD
Professor of Radiology, University of Missouri at Kansas City
Vice Chair of Research, Children’s Mercy Kansas City
-

What’s Your Number?
Planning for retirement is daunting. Something that many of us end up putting off in place of doing something else, anything else. We tell ourselves it is 10, 20, 30, or even 40 years in the future. Why is it that many of us, myself included, will spend more time researching a new TV purchase or our next vacation destination than planning for retirement? I’m here to tell you that it is better to start planning for your retirement now. We can strive for improvement, as I firmly believe that a doctor who is financially literate also becomes a more effective health care provider. When you have a solid grasp of your finances, you gain the capacity to make more informed decisions, not only for the benefit of your practice but also for the wellbeing of our patients.
Determining Your Retirement Number
Many of us delay retirement planning because it appears to be an intimidating endeavor. However, it doesn’t have to be. One of the initial steps is to determine your financial independence target, recognizing that this number is likely to evolve over the course of your career. Your number represents the amount of investable retirement assets required to maintain your desired standard of living throughout retirement. When you search for “how much do you need to retire,” you’ll encounter a wide range of responses, some of which may be inaccurate. Is it $1 million, $5 million, or even $10 million for a doctor to retire? Should it be 70% of your pre-retirement income, or perhaps 10–12 times your pre-retirement income? Regrettably, many of these responses fail to address the fundamental factor: how much you spend each year ultimately determines the amount needed for your retirement.
Safe-Withdrawal Rate and the 4% Rule
In order to comfortably retire, you will need about 25 times your annual spending to fund a 30-year retirement. To put another way, an investor who maintains a portfolio consisting of 75% stocks and 25% bonds can safely withdraw 4% of their portfolio’s value annually, adjusted for inflation, to support a typical 30-year retirement without the risk of depleting their funds. This is known as your safe-withdrawal rate and what has been known to many as the 4% rule of thumb. Now, this 4% withdraw rate and spending allocation must encompass all expenses, including taxes, health care costs, and financial advisory fees. If you spend $120,000 per year, you will need about $3 million in invested assets. For every $40,000 a year spending, you will need another $1 million in your retirement portfolio. This is based off “the Trinity study,” where Cooley et al. looked at historic safe withdrawal rate based on varying percentages of a stock/bond portfolio. This American Association of Individual Investors feature helped determine what percentage of money you could safely withdraw each year, indexed to inflation, and still have a reasonable chance of having money left after a 30-year retirement. In the majority of instances, individuals employing a 4% withdrawal rate during retirement will find themselves with a larger sum of money by the end of their retirement period compared to their initial retirement savings, frequently exceeding twice the amount they began with.
Informally referred to as “the Trinity study,” as all three authors were professors at Trinity University in San Antonio, TX, Cooley et al. updated their original 1998 paper in 2011 to include data from the Great Recession of 2008. The authors looked at historic, rolling 30-year periods from 1926–2009 to help determine what withdrawal rate, indexed to inflation, would sustain different retirement lengths using different portfolios that were invested in a mixture of stocks and bonds. This study challenged the long-held belief that if a stock portfolio maintained an average annual return of 9–12%, it would be safe to withdraw 7–9% annually in retirement, ensuring the portfolio’s sustainability indefinitely. The primary factor rendering this strategy unfeasible during various periods is the risk associated with the sequence of returns.
Sequence of Returns Risk
The sequence of returns risk relates to the idea that the performance of your portfolio early in retirement matters more than the performance late in retirement. The term “sequence” pertains to the adverse effects of experiencing low or negative investment returns during the early years of retirement, which can significantly influence the longevity of your retirement portfolio.
Consider, for instance, two retired investors who both achieved an average annual return of 7.75% throughout a 20-year retirement period, all while making annual withdrawals of $70,000 from their initial million-dollar portfolio (Fig. 1).
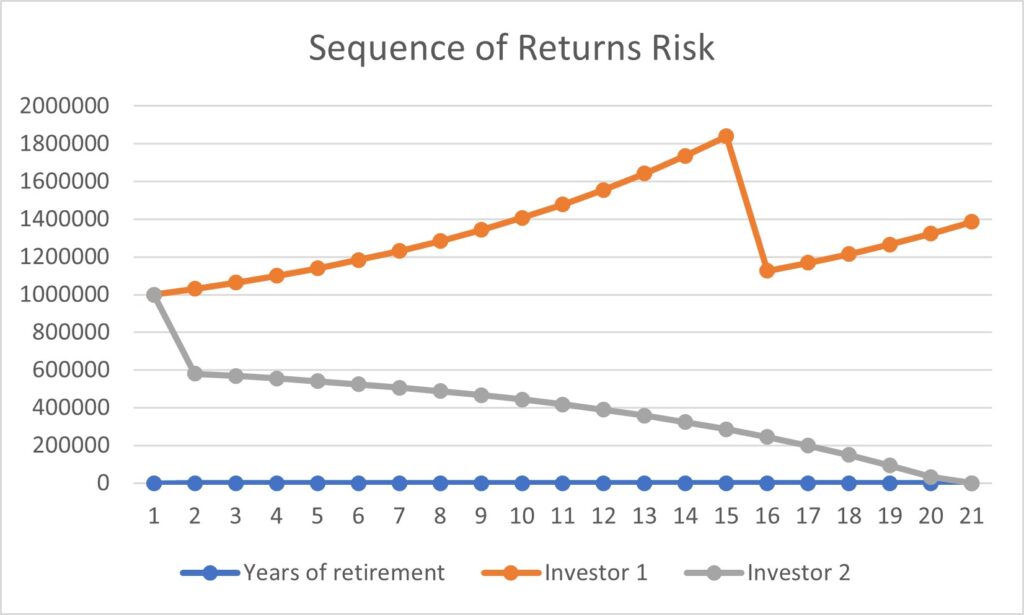
Fig. 1—Both investors initiated their retirement with a $1 million portfolio balance and achieved an average annual return of 7.75% over a 20-year period, while withdrawing $70,000 annually. Investor 1 (orange) experienced a 35% decline in their portfolio balance in the 15th year of retirement, while Investor 2 (gray) encountered the same 35% drop in the first year of their retirement. The sequence of portfolio returns during the early stages of retirement significantly impacts the probability of the portfolio lasting throughout the entire retirement period, necessitating a much lower withdrawal rate when compared to the average portfolio return. In the case of the first individual, they consistently enjoyed returns of 10% per year, but in the 15th year, they experienced a significant negative return of -35%, resulting in an average return of 7.75% over 20 years. The second individual, on the other hand, also averaged a 7.75% annual return, but their portfolio started with a 35% drop in the first year, then averaged a 10% annual return for the subsequent years. It’s important to note that both individuals maintained an average return of 7.75% while withdrawing the same amount annually. However, the outcome differed significantly: the first individual concluded their 20-year retirement with nearly $400,000 more than their initial investment, whereas the second individual exhausted their funds in the 20th year. This highlights the critical importance of setting a withdrawal rate lower than your rate of return in retirement, as the sequence of returns can have a substantial impact on the outcome.
Accumulating 25 times your annual spending in investable assets serves as a general guideline for achieving a successful retirement. However, in practice, many retirees adapt their discretionary spending based on their portfolio’s performance. During prosperous years, they can afford to spend more than the 4% benchmark, while in challenging years, they have the flexibility to reduce discretionary expenses and withdraw less than 4%. Nevertheless, it all commences with gaining a preliminary understanding of your annual spending, as this forms the foundation for determining the retirement nest egg required.
So, I ask again, what’s your number?

Christopher M. Walker, MD
Glen and Karen Cox Endowed Professor of Radiology
University of Kansas Medical Center
The Glen and Karen Cox Endowed Professor of Radiology and a practicing cardiothoracic radiologist at the University of Kansas Medical Center, Christopher M. Walker, MD, is not a certified financial planner, accountant, or attorney. This information is presented for your entertainment only and does not constitute formal and personalized financial, accounting, or legal advice. Your personal situation may be different, so please consult your own tax attorney or fee-only financial planner for advice pertaining to your situation.
-

Anything Goes—Is It True for Leadership Styles?
There is no doubt that, over the next few years, we will need more leaders in radiology that can fill the shoes of the mighty baby boomer generation. Many early career radiologists believe they do not have what it takes for leadership. But is that true? Is it a matter of “nature versus nurture?”
I have concluded that “(almost) anything goes” when it comes to leadership styles, and that while it helps to be genetically endowed with such skills, everything can be learned. Or is that even necessary? After all, most everything, from developing a vision and mission to executing our daily work, can be driven by teams, and it can be the total of team members that has the skill set, rather than a single leader who has it all. After all, this is reflected in many academic radiology departments, where the leadership cadre is made up of vice chairs, who bring very specific leadership and subject matter skills to the table.
When I first became curious about a leadership journey in my career, I asked my then section chief and department chair for leadership book recommendations. One recommended Edward Kennedy “Duke” Ellington’s biography. In reading the Duke’s biography through a leadership lens, it became clear to me that he valued the musicians in his orchestra very much. In fact, he wrote music that would showcase the skills of individual musicians. In addition, Ellington was a phenomenal businessman who was committed to delivering music of the highest quality.
The other recommendation was to read Endurance, a book about the explorer Sir Ernest Henry Shackleton and his expedition to Antarctica on the ship Endurance. The book details how the ship got trapped in packed ice and sank, and how Shackleton’s exceptional leadership resulted in the survival and rescue of all crew. In essence, Shackleton never wavered in his vision of survival for the entire crew, which informed all decisions he made along the way. On the other hand, in terms of planning this expedition for all eventualities, Shackleton miserably failed in his leadership.
In my career, I have both employed and lived through a large variety of leadership styles, and I have concluded that more often than not, circumstances inform which leadership style works best.
Authoritarian – Participative – Delegative
While there are undoubtedly negative connotations to being an authoritarian leader in the political world, this leadership style can be very effective when projects need to be completed quickly. A group may prefer this leadership style, when the leader is the most knowledgeable group member. This style does not, however, support the professional skills and advancement of others.
Participative or democratic leadership, on the other hand, is all about welcoming diverse opinions and collaboration. Research finds that this leadership style leads to higher-quality outcomes, but it can take longer to get buy-in from all team members.
Delegative leadership is a laissez-faire style. The leader is removed from the team’s process, but expects a certain outcome. This could be successful when all group members are qualified experts.
Visionary – Coaching – Affiliative – Commanding – Pacesetting
Visionary leadership is often authoritative and can inspire and motivate others. However, a vision only takes the team so far. Having a clear vision to hold on to can help teams that are undergoing dramatic changes within the organization, such as a new practice leader.
Coaching leaders are those who can help team members improve to support the organization’s goals. This requires the ability to give feedback, which can be an artform in itself…
The affiliative leader is relationship-focused and creates harmony among team members. However, if harmony is of the utmost priority, team performance could suffer from lack of constructive feedback.
The commanding leader coerces the team through policies and procedures. As a sole leadership style, this can lead to disengagement of team members. Undoubtedly, though, policies and governance are the necessary foundation for creating accountability and guiding performance assessments.
Pacesetting leaders serve as an example in productivity, performance, and quality. Leaders who create clear requirements for their teams and set deadlines may be very successful, but this style can also result in overworked teams.
Transformational – Transactional
The transformational leader uses coaching and other means to empower teams towards building skills and growing towards a common goal. Meanwhile, the transactional leader drives performance through rewards and punishment. Since external reward/punishment systems work better for achieving short-term goals, this leadership style may not be successful in the long run. I hope this brief overview piques the interest of radiologists who are interested in leadership, but who are unsure if they are cut out for it. A good starting point may be to ponder one’s strengths and find a leadership opportunity in a setting that would benefit from existing skill sets.

-

A Recipe for Resilience: 10 Key Ingredients to Add to Your Mix
This post was originally featured in ARRS InPractice.
“This pandemic is really getting me down… I’m not sleeping well… Small things worry me constantly… My concentration drifts while interpreting studies… Antacids are taking care of my epigastric symptoms… Alcohol has become a necessary crutch to help me sleep… Everybody seems so needy around me… The media is driving me insane… The sense of loss overwhelms me at times… I cannot bear the thought of more Zoom meetings…”
Resilience. It’s a concept that predates the pandemic and one that we’ve heard about in personal development books, TED Talks, and leadership courses many times before. The word conjures a sense of unshakeable inner strength that’s impermeable to outside forces, like a giant African baobab tree—also known as the continent’s “tree of life”—during a torrential storm. You might define resilience as the capacity to recover and bounce back from adverse circumstances, such as those many of us are currently experiencing, as illustrated by the sampling of comments above.
It often feels like the pandemic swiftly derailed the pre-2020 tools and strategies we had introduced to our organizations to identify and combat employee burnout and support the collective health and wellness of our teams. While stressors have expanded and amplified, the concepts that were leading us on a path to healthier workplaces are still valid and valuable, particularly when it comes to resilience. With intention, practice, patience, and persistence, resilience can be learned, sustained, and strengthened; with resilience, we can emerge from our proverbial emotional basements, even during the most turbulent of weather.
Opening the Cookbook
While it’s not quite as simple as following a step-by-step recipe for your favorite meal, several key ingredients can help you develop resilience. Let’s explore 10 of them here.
- Take care of yourself, first and foremost: If you’re a leader, remind yourself of the airline analogy to put on your own oxygen mask first. Learn to practice mindfulness to slow down and reduce anxiety. Learn to focus on being intensely aware of your senses and feelings in the moment, without interpretation or judgment. Be mindful, too, that you may be using unhelpful coping solutions. Try to eat healthily, sleep to rejuvenate, and exercise as best as you can, wisely. Doing so should boost your capacity for physical resilience. Consider strategies to boost your mental resilience, as well. How do you reignite your energy and creativity after challenging situations? Are you able to effectively disconnect? Build time into your schedule to recharge. Develop coping skills to help you manage stress, so that it doesn’t compound. One example of a valuable coping mechanism is laughter, which can reduce anxiety and increase our intake of fresh oxygen. Try to find ways to laugh each day, as part of your self-care practice. You can even find laughter yoga exercises on YouTube.
- When something is not quite right, recognize, acknowledge, and call it what it is: Stress. Anxiety. Overwhelm. Depression. PTSD. Whether it is a formal diagnosis from a care provider or a gut instinct that you have, it’s OK not to be OK. The pandemic is amplifying our national mental health crisis. Recognize and mourn your losses, no matter how big or small you think they are. Communicate openly and honestly about your current state of mind; don’t minimize or ignore your symptoms until they become intolerable. Share your concerns with your primary care provider, a licensed therapist, a trusted family member or friend, or a 24/7 hotline. If you are in a potentially life-threatening situation, call 911, or go to your nearest emergency room. Opening up and asking for help can be terrifying, but you are worth it. No one is alone here. Seek the support and care that you deserve and need.
- Find your sense of purpose: Develop your personal W-H-Y? Find intentional ways to connect to your larger life purpose and learn to savor them. What are your volunteer efforts? What does your charitable giving list look like? Altruism drives a sense of purpose and is a recognized trait of resilient individuals. Try to integrate your work and life effectively for you. Strive to be a realistic optimist and, rather than focusing on the negative, hone in on what you can contribute to your community, region, state, or country.
- Get connected: Establish and nurture a supportive social network. Who comprises your safety net? Whose safety net are you in? Help others to support and nourish you by building a social resilience community. Never be afraid to lean on your support systems, even if virtually. How did you build your support group? Do you have an online community? Develop positive and trusting relationships in which you can work together to endure and recover from stressors. By listening and hearing, we can be kind and compassionate to others when they need it most. Do a proverbial mitzvah!
- Find your resilience role models: On a personal level, I derive such joy and inspiration experiencing the resilience of my immediate family members. As a South African, it will also never cease to amaze me when I consider the remarkable resilience shown by Nelson Mandela. His endurance and persistence in the face of severe adversity were coupled with his ability to show emotional regulation, empathize, build connections, demonstrate self-efficacy, and stick to his guiding moral compass through authenticity. His favorite poem was “Invictus,” written by William Henley, which ends with the powerful line, “I am the master of my fate / I am the captain of my soul.”
- Seek to constantly learn and improve: Be coachable and seek feedback that you learn from and act upon. Seek this feedback from those sources most likely to be helpful to you. Recognize that change can be good, however inconvenient or uncomfortable. View so-called “failures” as learning and improvement opportunities and embrace them; activate your action plan, rather than dwelling on what might have been.
- Know what emotional intelligence looks like: Practice self-awareness by knowing your stress levels and noticing your emotions. Train your brain—build emotional intelligence, moral integrity, and physical endurance. To boost your emotional resilience, work on understanding, appreciating, and regulating your emotions, while consciously choosing your feelings and responses to avoid being reactive. Learn to become self-aware. This includes recognizing what drives your stressors. What pushes your buttons? Finding and sticking to your moral center may aid this journey.
- Find ways to relax and decompress that work for you: Some examples include spending time with friends, pursuing hobbies, cooking, meditating, and listening to music. Each of these can be enjoyed in groups or individually, depending on what you prefer. As one example, photography is an art that can be practiced in mindful ways, shared with colleagues, and even used as a communication and connection tool. It might even influence your choice of travel locations and online connections. Surround yourself with positive energy. Misery doesn’t love company—find new ways to manage or even avoid adversities and adversaries. Have an executable plan to eliminate your blockages.
- Practice gratitude and self-compassion: Hardwire this into your daily activities list; it will help you to feel content. This might simply include journaling things that you are grateful for. You already possess a series of resiliency tools and have likely overcome adverse situations that you learned from. Your journey has already begun, and you have endured 100% of your worst days. Congratulate yourself for this.
- Reflect: This can go hand-in-hand with journaling. Simply put, sit quietly with the events and feelings of the day and see what comes up. Committing to creating the time for reflection allows one to build and increase self-awareness (an important component of emotional intelligence), encourages learning, and opens doors to being more adaptable. For events that occur, consider what happened, how it made you feel, and what lessons or new approaches you learned from the experience.
Sharing the Recipe
As a leader, your resilience impacts your performance, as well as the performance and engagement of your teams. Stressed leaders engage in fewer positive leadership behaviors, such as enunciating optimistic visions, setting and overseeing goals, communicating confidence, clarifying roles, showing genuine appreciation, and recognizing performance. Stressed leaders can become passive—they step in only when needed, tend to avoid decision-making, and can be emotionally absent. These attributes get noticed and impact teams. Resilient leaders can keep calm under pressure and develop additional skills (a component of posttraumatic growth) in the face of adversity. Through self-reflection and feedback, resilient leaders have a keen sense of the main components of emotional intelligence.
Resilient leaders can also regularly assess their leadership effectiveness and styles, more readily responding to change and unexpected situations. Striving to learn and grow continuously, resilient leaders are often purpose-driven individuals—they can visualize their work effort as being meaningful. Resilient leaders cultivate relevant and helpful relationships in their internal and external work environments that support them through tough times.
Why Is Resilience at Work Important?
Resilience shapes the way employees respond to the stress of change. It also relates to work engagement, job satisfaction, and organizational commitment. Resilience is inversely related to the frequency and manifestations of burnout and can improve organizational and employee performance.
How Do We Recognize Resilient Behaviors in Others?
A spectrum of characteristic behaviors and skills is recognized under the resilience rubric. Many of these are also included under a larger umbrella of effective leadership behaviors. A person who manifests resilient behavior communicates clearly, thoughtfully, and consistently. Moreover, effective leaders may design a strategy for communicating and managing change that accounts for different stakeholders and their communication preferences. Resilient individuals are coachable, regardless of their position in a hierarchy, and many seek opportunities for learning and improvement. They are willing to embrace change, and, ideally, they’re skilled at managing it. Resilient individuals are comfortable saying, “I don’t know” (and “I would like to learn”). They know how and when to take bold risks or when to initiate new ideas. Similar to effective leaders, resilient individuals are willing to and do invest in the development and advancement of others.
Those with high levels of resilience are better equipped to cope with stressful situations. They tend to see change as an opportunity, are optimistic, adaptable, and realistic about realities, and engage colleagues for support. Resilient individuals possess emotional regulation skills and don’t allow stress to impede their functioning. They practice self-compassion to reduce harsh self-criticism, soothe difficult emotions, and find sources of motivation. Resilient individuals show cognitive agility, a difficult skill to develop, which entails shifting how one thinks about negative situations.
Let’s face it: It’s really difficult learning to become resilient. It takes time, persistence, effort, commitment, energy, and a drive to succeed. We do know that resilient teams are best served by resilient leaders. Now more than ever before, we need our imaging teams to function effectively. Our teams should be equipped with resilience to face ever-changing challenges and unanticipated adversities, and whether they are or not begins with us as leaders.
About the Author
-

Reimagining and Reinventing Postpandemic Radiology
This post was originally featured in ARRS InPractice.
Some days, it’s hard to recall what prepandemic life was like. Things have forever changed in light of this historic global event, and it’s vital to reflect and process these last three years. We’ve endured some of the most trying times of our careers, but we also have a bright future as a medical community ahead. You’re wondering what that might look like and how we can collectively “skate to where the puck is going to be, not to where it has been,” as Wayne Gretzky famously said.
COVID-19 precipitated a fundamental change in clinical service delivery, teaching, research, staff retention, employee wellness initiatives, and communications strategies. We amended workplace safety standards and practices, stood up and resourced remote teams, recruited trainees virtually, and transformed in-person grand rounds programs into digital ones. These are just some of the many efforts that we as a specialty undertook to protect our people, uphold our missions, and keep our teams employed. And while not all changes were novel ones, the pandemic catalyzed their implementation. We now have tremendous momentum to continue innovating, especially as we begin to emerge from crisis mode together.
Accelerating Change
Here at Beth Israel Deaconess Medical Center, we simply couldn’t have managed this public health crisis without our highly effective, efficient, and resourceful operational surveillance systems and teams. Some of these teams were in place before the pandemic started; they rapidly responded to the initial phases of COVID-19, then swiftly transitioned into a multidisciplinary incident command structure to assess, rethink, reinvent, iterate, and communicate our health care systems and strategies on a daily, hourly, and minute-by-minute basis. This collaborative structure operated in real time and kept our trains running, on schedule and on the tracks, far more often than not. Light started to appear at the end of the tunnel, and then, the alphabet of variants arrived. It soon became clear that we would never return to prepandemic normalcy. A fundamental shift had taken place in the way we delivered our services, and some of this change represented the necessary digital transformation many had envisioned long before COVID-19 struck.
So, what are our next steps? How can we effectively shift from a reactionary mode to one that is deliberate and purposeful? What structure will best support the necessary regrowth phase that will support our medical practices and organizations? Now is our time to be accelerators rather than incubators, to reinvent and rebrand our skills and clinical contributions, and to be thoughtful and strategic in the process. This is where the most strategic, imaginative, and operationally agile teams will lead the way and define our recovery. Those who embrace change and progress will be the best positioned to thrive. Lead the change. Be the change.
Building COVID Recovery Hubs
Let’s be the disruptive thinkers our field will be proud of. Define, then communicate your future radiology vision. Do this in an inclusive manner that involves all role groups. For such plans to be adopted and successful, leaders will need to continue to create forums for staff to weigh in, ask the right questions of their teams, listen to feedback, barriers, needs, and ideas, and provide other ways to share input, such as through short pulse surveys in a departmental newsletter or real-time polls during meetings. Ensure everyone’s voice is heard and incorporate major common themes into your plans.
We suggest constructing and resourcing a formal COVID recovery hub, which can house your postpandemic mission, vision, and recovery playbook. Appoint and support a multidisciplinary team to lead and own these pioneering transformation efforts. Who have you appointed to lead your radiology recovery, reinvention, and reengineering transformation? What does your “r4” portfolio look like? By answering these questions, you will help your practice continue to keep its staff and patients safe, deliver exceptional care, manage ongoing people and supply chain shortages, support staff morale and wellness, nurture remote teams, and effectively communicate and engage with a multigenerational workforce.
Reimagining Administrative Functions
As part of your COVID recovery hub, consider the roles, responsibilities, and constituents of your leadership team. Are you best positioned for your recovery? Now might be a great time to reimagine these elements and challenge the traditional hierarchy, as we work to flatten authority gradients, build diverse, inclusive, and multigenerational teams, and ensure that form follows function. Additionally, these roles have likely transformed out of necessity during the pandemic and might need to evolve to meet your practice’s future needs.
Let’s be a little provocative: how can we identify the best person to be our “knowing exactly where the puck will be in 2030” portfolio leader? Actually, this is not a task for one person—and this is precisely why building and sustaining high-performing diverse and inclusive teams will become paramount and essential. Proudly establish your recovery hub, appoint a vice chair of recovery and reinvention to lead this effort, then establish and resource new portfolios to signal just how serious you are about recovery, regrowth, and reinvention. For example, have you considered the future of your remote teams? Based on national employee preferences, it’s clear that some level of remote work is here to stay. Perhaps, as part of a practice’s new digital innovation and transformation lab, it could create a remote workplace and team-building portfolio. Will your organization continue producing short video messages, digital newsletters, social media content, and academic webinars? What will your postpandemic communications strategy look like? Perhaps it’s a question for a newly formed digital communications and connections team. While these structures might not be novel in a large, digital-first corporate setting,they would be a progressive leap forward for many of our major academic medical practices.
Additionally, we all know that health care delivery has progressed to incorporate population health, cost reduction improvement efforts, care coordination and integration, and customer experience, among other important factors. Simply put, our aim is to deliver the highest-quality, safest possible care and experience at the most sustainable costs. This boils down to value, and who better to drive it than an effective chief value officer?We’ve certainly been talking about this value proposition for quite some time already. On a different but equally important note, we must think about how we will continue to support the health and wellness of our staff postpandemic, especially during our nation’s mental health crisis. Is there an influential and compassionate leader on your team who could become your chief wellness leader and drive these vital efforts to aid your entire team?
The structure of a leadership team should primarily relate to its intended function and purpose. Once you have reconfirmed your foundational core purpose, reimagined your vision and mission, and defined your annual goals, then form the team (and define their precise roles) that will help you reach your ideal future state. Energize your teams by including them in strategic brainstorming and planning sessions, imagining an exciting and successful future together.Designing a newoperational landscape is not a task for one person, which is why building and sustaining high-performing, diverse, and inclusive teams will be paramount.
The interesting exercise that we are all engaged in now is to define that future state. Has anybody considered a leader of a recovery and reinvention portfolio? Your entire team wants to contribute! Be inclusive and build diverse teams.
Mapping New Pathways
This is an era of posttraumatic regrowth. Reimagining your pathway should be an inclusive, aspirational, and even inspirational process. Be thoughtful and strategic when redefining your path forward toward the new normal you and your team aspire to achieve. Reengage and revitalize your most precious resource, your workforce. Recommit to safe practices, wellness initiatives, and high-performing team building. Reconnect your teams, and work to sustain these connections. Reimagine and rethink your strategic plan and goals, and start your new journey today. Those who will flourish and thrive will do this effectively, thoughtfully, and strategically; consider the long-term goals, map out your route, and take action. As you shift from managing operations to imagining the future, try to shift your focus from keeping the trains running to considering where new rails could be built. Periodically, it’s important to pause and ponder—to consider not only how trains can be better engineered, but also to contemplate whether train travel will be a safe and efficient customer choice in the future. That’s strategic thinking.
Let’s try to simplify. You’re done with reacting, reflecting, and responding. You’re starting to see some light at the end of this tunnel. You’re hoping that omicron is the last symbol of this pandemic alphabet. Now, more than ever before, is the time to look forward, plan your recovery strategy, and focus on building and sustaining innovation. The practices that are most likely to thrive are already thinking outside the traditional administrative oversight box. And they are moving ahead right now.
And, finally, find ways to share your experiences of this journey. We’re all traveling new paths and learning as we go. We must learn from each other’s successes and missteps, and there will be plenty of both. As we build our departmental COVID recovery hubs, we also need to design and build collaborative teams to communicate and interact with institutional, regional, and national COVID recovery hubs, to the extent they exist. These new systems must be capable of redefining and reimagining the future, so that we can all travel along the path of progress together.
It’s now time to be intentionally inclusive, as we commence this new journey.
About the Authors
-

Finding Our Proverbial Sunrooms
This post was originally featured in ARRS InPractice.
Feeling stuck, joyless, or “meh?” You, like many others, might be languishing. In fact, it might be the dominant emotion of 2021.
Sociologist Corey Keyes describes mental health as a continuum: ranging from flourishing, that state of wellbeing we all seek to achieve, to languishing, the absence of wellbeing, and a lower state of mental health. Languishing is distinct from depression, yet individuals who are languishing are at a higher risk of future mental illness (such as depression and anxiety disorders), as shown by Keyes et al..
Simply put, languishing is a series of emotions, rather than a mental illness. Adam Grant, writing in the New York Times, refers to languishing as “the neglected middle child of mental health” and “the void between depression and flourishing.” Given the negative impacts on productivity, morale, innovation, team building, retention, and engagement, nonprofit organizations and corporations alike must take this widespread state seriously.
The pandemic has impacted almost every structural framework of our lives, such as socializing, working, vacationing, traveling, and exercising—and, in turn, compromised our sources of joy. With no clear path as to when and how our “future state” will present itself, we continue to exist in an ongoing and indefinite interim state. As uncertainties persist and routines remain in flux, many people are being shuffled into a state of languishing.
You Might Be Languishing if You Are:
- overwhelmed or emotionally numb
- distracted and unfocused
- depleted, empty, and/or disinterested
- unmotivated or procrastinating
- not functioning at your full capacity
- unable to feel excited about upcoming events
- cynical about your colleagues and leaders
How Can We Shift From Languishing to Flourishing?
Below, I share a compilation of suggestions from the experiences of many. If the symptoms of languishing seem familiar to you, perhaps one or more of these strategies might help. If even one person finds solace in these ideas, it would bring me joy.
- Prioritize your health: Do your best to eat healthily, drink plenty of water, sleep well, and incorporate movement into your life. Schedule and keep your annual health appointments. Consider alternative medicine modalities, such as acupuncture and chiropractic medicine. Find moments to sit in silence and simply breathe. Use your personal time and plan vacations, including memorable “staycations.” Disconnect from work and social media during your time off. Set boundaries and learn how to respectfully say “no,” when needed. Take your first small step toward doing something you’ve always wanted to do for your health today.
- Protect your time: Manage your time intentionally and purposefully. Detach, disconnect, and learn how to engage your personal reset button. You might try scheduling uninterrupted time for yourself to recharge your batteries, even if this means “doing nothing.” Limit social media scrolling and email checking. Consider recapturing your prepandemic experiences; for example, create a virtual “commute” that includes a home spin class, podcast episodes, reading, music, or another element that helps you transition from the waking to working hours.
- Make positive connections: Reengage or recreate your personal and professional network. Recall who once might have lifted you up. Walk and chat, gather and eat, find and embrace, and explore commonalities with positive people. When possible, spend less time with those who drain your energy and spirits. Seek a peer support buddy with whom you can share your experiences and feelings. Look for authentic and uplifting connections to replenish yourself emotionally.
- Reflect on the current situation: Acknowledge the loss and anxiety and frustrations and grief. What have you lost? What have others lost? What has everybody lost? Recognize that you’re not alone here.
- And then, practice gratitude: Recognize what you do have, rather than focusing on what you don’t. Appreciate what is working, rather than focusing on what isn’t. Try keeping a daily gratitude journal or using a meditation app, like Calm or Headspace, for guided gratitude practices.
- Find flow and motivation: What’s on your music playlist, and when did you last update the content? Step out of your comfort zone by trying a new recipe, exercise, podcast, app, or online class. Get better at something, whether it’s dance, yoga, art, reading, writing, meditation, music, composting, or gardening. Explore mindful crafting, photography, collecting, and other hobbies. Reconnect with and walk barefoot in nature for additional grounding.
- Celebrate small successes: Rethink what constitutes success, however small. It may be someone else’s success or happiness that you contributed to. When overwhelmed, rethink your goal-setting strategy. Set simpler goals that are achievable, and enjoy the successes that you are contributing to. It’s OK to start small. Perhaps also schedule achievable self-care activities each day.
- Rethink your possessions: What would you like to keep or surround yourself with? These items might include things that bring you joy, inspiration, hope, confidence, or calm. Consider decluttering a room or maybe even your entire living space over a period of time. According to a recent Psychology Today article, decluttering can be very beneficial.
- Change your scenery: Breaking from a stagnant routine is challenging. I encourage all of us to find ways to get out of our emotional basement and head up to our proverbial sunroom. Take a stroll through your memory banks to recall what may have once ignited your passions. Learn the art of introspection—what does your perfect day look like?—and consciously do something new or different to refresh your spirits. Check out your local museum, gallery, or library with a friend. Sign up for an online class or enjoy a virtual comedy show. You never know what you may discover.
- Find joy in giving: When did you last wrap a small gift? Who can you help today? What causes would you like to reengage with? Have you discussed and explored different options with your friends and family? Try to get back to your talents and gifts. Learn to be a peer supporter. Research volunteer opportunities in your community. Contemplate your purpose and remember what truly drives you. Helping others can bring a tremendous sense of inner fulfillment.
- Activate your personal coping strategies: For some, the average workday may seem filled with one stressful encounter after another. Meetings may not go as planned. Your workflow may be interrupted. The dominant sentiment might be that this is just another tough day. Is it possible that you are being too hard on yourself and in your judgments? For example, while you may feel that a meeting, interaction, or event didn’t quite go as planned, perhaps that is from your perspective. Maybe others had a different perspective and felt more positive about the encounter. Activate your personal coping strategies to decompress, relax, boost your energy, stay focused, gain perspective, and reflect on the bigger picture.
- Explore therapy. It’s a strength to recognize when we need professional help. According to a recent Value Penguin survey of more than 1,300 US adults, “nearly 30% of Americans have seen a therapist during the coronavirus pandemic, and 86% say it’s helped them cope.” Psychiatrists, psychologists, social workers, therapists, and other licensed practitioners are trained to help patients construct a personal repertoire of coping strategies. There are many forms of therapy to consider, including psychodynamic, cognitive behavioral, dialectical behavioral, mindfulness-based, and art. One or more of these modalities could help you address and manage stressful life events.
The journey from languishing to flourishing is of indeterminate length, and some of the “travel aids” listed above may be more effective than others. What we need is a means of sharing best practices—what worked well and what didn’t—multigenerational preferences and impacts, as well as other solutions that have been identified along the path. I can only wish each of you who may be experiencing a state of languishing a very safe, healthy, memorable, and rewarding trip back!
About the Author
-

Addressing the Concept of ‘Moral Injury’
This post was originally featured in ARRS InPractice.
The COVID-19 pandemic continues to exacerbate the pre-existing epidemic of stress, distress, dis-ease and burnout in our profession—and across the country. Contributors to workplace stress in radiology have been further compounded as we grapple to provide safe care to our patients, keep our teams healthy, uphold social distancing requirements, support, sustain, and engage remote teams, deploy effective communication strategies, and cultivate diverse and high-performing teams. People across the country are fighting silent battles against chronic anxiety, depression, and other mental health disorders during any given workday.
Prior to the pandemic, we heard frequent reference to the hamster wheel environment in which we work; expectations of ever increasing workloads and so-called quality metrics driving us to work faster and longer hours all while meeting ever increasing regulatory requirements. Not surprisingly, the consequences of just trying to keep up include burnout, and the field of radiology is still seeking solutions to mitigate our recognized high incidence.
However, in parallel with burnout is the growing focus on mitigating known stressors, those that establish a genuine conflict between our core values as care-providing physicians and our daily activities in the trenches. This is the reality of the so-called moral distress and injury, which is frequently associated with burnout. To me, this implies that we as individuals are unable to balance work expectations against personal resources—that, somehow, we are failing at what we “should” be doing and achieving. There is a growing school of thought that the symptoms of burnout simply reflect a healthcare delivery system in need of urgent repair. The moral insults and injury of healthcare is not being able to provide the high quality of care that we would want to, thus highlighting the opportunity to address what is contributing to this state. And the consequences are dire: physician suicide rates are now twice that of active-duty military members. Now more than ever, it is clear that we must reprioritize employee wellness efforts and implement additional strategies to protect and support our workforce.
Treating the Cause
To effect lasting change, we must reshift our focus and address the cause rather than the symptoms. While appreciated and beneficial in their own right, wellness programs, flexible schedules, extra time off, and other employee benefits oftentimes treat the short-term symptoms, not the long-term cause.
Relaxation practices, exercise, vacation, mindfulness activities and meditation might be extremely effective at resolving some symptoms on a temporary basis, at least until that time that we are back trying to balance on the hamster wheel. To address the causes, we need brave and effective leaders who are willing to question and confront the constellation of drivers, and who recognize and respect the fourth component of the quadruple aim of healthcare (care of the patient requires care of the provider). We must excavate the problem that is moral injury until its origins become clear.
Numerous factors detract from what we believe is our primary mission and contribute to such injury, including the profit-driven healthcare environment, electronic health records and productivity metrics, provider review sites, litigation concerns, turnaround time targets, and the ever-expanding regulatory mandates. Here I refer to practices mandated by regulatory agencies such as audits, documentation expectations, annual testing, and of course, the unpopular practice of peer review.
Let’s consider peer review as our low hanging fruit here. This is a process that in radiology is often known for being onerous, burdensome, distracting, divisive, resource-intensive, inefficient, and ineffective. In my experience, it can be difficult to use peer review as a driver for meaningful and impactful improvement.
However, the concept persists, in large part due to meeting accreditation and reimbursement requirements. As radiologists, we are expected to devote time to rank the diagnostic skills of our colleagues. During this process, targeting occurs, under-reporting is rampant, and job security might be impacted, yet challenging the status quo is difficult. Despite evidence that radiologists make errors almost 30% of the time, national peer review data reports fewer than 5% of these discrepancies. Is this practice truly an effective use of our time and skills?
Forging a New Path
Peer learning and improvement offers us an enormous opportunity to remove a mandated hurdle to our work-related distresses; it also allows us to embrace an emerging practice that will provide new learning and improvement opportunities. Today, I’d like to give a loud shout-out to the many peer learning trailblazers out there, including: David Larson, Richard Sharpe, Jennifer Broder, Nadja Kadom, Lane Donnelly, Mythreyi Chatfied, Andrew Moriarty, and Richard Heller. And this cohort is growing rapidly.
Now is an ideal time for the field of radiology to commit to taking the necessary steps to embrace peer learning in our practices. This will be a journey that many have commenced, along varied paths, influenced by practice patterns and cultures. In some practices, this will require cultural transformations, so that staff are willing to speak up safely in a Just Culture without fear of consequences. It will require hospital administrators to embrace all components of peer learning as meeting local OPPE requirements. It will require that the focus shift from scoring diagnostic discrepancies to identifying learning and improvement opportunities, and that participation is expected. In fact, willing participation could replace annual denominators altogether. Peer learning leaders could be identified and appropriately trained, and their work acknowledged as a vital part of our performance improvement processes. Most important, the American College of Radiology (ACR) has now approved a new pathway for ACR-accredited facilities to meet the Physician Quality Assurance program requirement, opening a path for practices to embrace this learning and improvement and non-punitive approach, thus no longer needing to use a score-based approach.
I started this column addressing the additive impacts of the pandemic on our preexisting stressors and burnout numbers. I highlighted the growing recognition that the so-called moral injury is an additional and major contributor to our current distress. Transitioning from retrospective peer review to prospective peer learning practices is one superb example of how we can mitigate a known contributor and provide what will, hopefully, be some major relief to our radiologists. This could allow our colleagues to participate in a process that is likely to positively impact our performance and the quality of care that we deliver. Because, ultimately, I believe that’s why we are all here.
About the Author
-

Abundant Opportunities to Bridge Digital Disparities
This post was originally featured in ARRS InPractice.
During this year’s virtual and highly successful American Roentgen Ray Society meeting, it became apparent that we are living in a time of accelerated development and deployment of existing and emerging digital technologies. Individuals and teams are using innovative solutions to care for patients, teach trainees, collaborate with colleagues, and connect within an expanding digital universe.
I for one never imagined that my weekly mobile COVID-19 prediction report would include hourly population densities in nearby airports, supermarkets, restaurants, and bars. With geographically traceable devices, what data could possibly be next?
In the same way that NASA’s Apollo program sparked the development of new technologies (many of which were largely realized and appreciated years later) that landed the first humans on the moon, we are witnessing a fundamental transformation in health care operations that will be captured in future history books. Few could have predicted, for example, that CT scans would become an indispensable screening, diagnostic, staging, and management tool during a global pandemic. Providers have harnessed such a wide swath of tools—from laptops, mobile and wearable devices, and video conferencing to artificial intelligence, thermal sensors, and robots—to better serve patients and their loved ones, sustain remote reading and teaching environments, and uphold compliance and safety protocol. We now achieve efficiencies through rapid scanning, recruit new faculty through social media, teach our trainees in cloud-based classrooms, and attend national conferences with just a click—all without ever boarding a plane or even crossing clinical campuses.
The Future Is Now
The evidence shows that embracing digital technologies results in improved patient outcomes, cost savings and efficiency, increased productivity, heightened compliance and safety, transformed teaching methods, stakeholder satisfaction through digital connections, sustained remote teams, and accessible employee communications and wellness initiatives.
Previously, such innovation resided primarily within the hospital and physician domains, with the gradual integration of patients as they began accessing their personal electronic health records. Now, our digital stakeholders include not only patients, but referring providers, remote teams, educators and learners, researchers, public health authorities, policymakers, schedulers, transporters, the public, commuters, and travelers.
And as the digital stakeholder pool expands, so does its impact: Such technologies now routinely support telehealth, data analysis, access, scheduling, and follow-ups, management decision-making, bidirectional communication, safety compliance and practices, PACS enhancements, teaching and readouts, patient monitoring, diagnostics, consulting, screening, training, forecasting, reporting, and, of course, socializing.
Examining Digital Disparities
We must remember that our digital environment is far from globally universal. At-risk, vulnerable, underserved, and marginalized populations, such as those living more than 7,600 miles away in India today, are grappling to secure simple access and connect effectively with providers and health care delivery services through traditional means, let alone digital ones. They desperately need hospital beds, oxygen and plasma, life-saving vaccine doses, and medical workers. Resources that hospitals, such as ours, are so fortunate to have readily on hand. However challenging these issues are to address, such disparities in access, care, and connections must be studied and included in the many national efforts aimed at eliminating them. What a terrific opportunity for us to make a meaningful difference that matters.
To a large extent, this digital divide is driven by equality, equity, and justice, or the lack thereof. With equality, we assume that here in Massachusetts, for example, all of our patients benefit from the same supports. All are treated equally, irrespective of any differences. But this isn’t necessarily true yet. Having a laptop certainly doesn’t mean a patient can easily access and understand one’s medical records. Additionally, not all laptops have video cameras, and not all hardware supports the ability to participate in video conferencing or telehealth solutions. And then there are those patients who don’t have access to a laptop to begin with. Where does that leave them? It is our responsibility to find out.
From the perspective of equity, everybody receives the specific and different supports they need and, therefore, receive equitable treatment. This is closely tied to justice (some view this as liberation); our underserved patients receive access to appropriate care without requiring specific accommodations because the fundamental causes of inequities have been addressed. In other words, the preexisting systemic barriers have been effectively identified and removed. Consider the impacts and barriers that may exist due to language, poverty, mobility, cognition, geography, access to water, electricity, food, transport, comorbidities, and employment status. By working to eliminate or flatten these barriers, care becomes more equitable and just. There are innumerable opportunities for making a difference that matters here, starting locally.
Bridging Local Gaps
Consider your own imaging team: When you hold video meetings, do all members have equal access to the necessary hardware and software to participate effectively? Are all members afforded the same privacy and time to participate in these meetings? This lesson was brought home to us when we recently convened a video meeting of our wellness council and noticed that several of our technical and nursing staff did not have access to video equipment in their workplace.
Consider your patients, as well: While a health care system might deploy sophisticated software to support their telehealth endeavors, this does not mean that all patients have the necessary hardware or software to participate. Additionally, solutions to barriers such as vision, language, and hearing must be readily available. One additional effort I applaud is to make our digital reports more comprehensible; not every patient understands what is meant by the phrase “the hepatic parenchyma demonstrates a normal echotexture,” nor should they. We should support software solutions to simplify the communication and accuracy of our recommendations.
And in keeping with our educational mission, think about the brisk implementation of so many solutions to support ongoing academic efforts. Will we ever return to our traditional morning resident teaching conference? I’d imagine not; if anything, the pandemic will finally allow us to move away from the prolonged didactic and synchronous teaching methods to ones that are more appropriate, personalized, and contemporary.
Another essential pillar of academic radiology is teaching and developing the next generation of radiology leaders during readouts. We seem to be mired in surveys and comparisons about what processes work best for our traditional readouts. Let’s instead open our eyes to completely new and asynchronous approaches. What an opportunity! And last within this category is lifelong learning. The necessary transformation to virtual national academic meetings this past year has demonstrated the many advantages that our digital environment offers for such forums. Be it cost savings for participants and practices, wider availability of CME credits and on-demand content, less time away from the workplace, or and the ability to directly connect with speakers, the benefits are plentiful.
Keeping Our Imaginative Focus
Where the opportunities lie here are in fostering participant connections and rethinking how we should transform the content, styles, and media of our traditional talks to take full advantage of individual learner needs and preferences. Again, what terrific opportunities exist in this domain!
So, where do we go from here?
While tremendous and necessary strides have and continue to take place in our abilities to communicate, manage, and connect remotely, I only ask that we continue to be mindful and considerate that not all stakeholders are currently able to participate equally and effectively. The phrase “you’re only as fast as the slowest member of your relay team” is so apt nowadays. In our digital environment, the concept of “precision medicine” should now expand to embrace the specific needs and preferences of our many stakeholders.
As we continue to build and expand our digital frontend, it is equally necessary to focus on supporting the backend, so that all of our team members and stakeholders can participate and benefit from the systems and solutions that are being deployed. The opportunities here are endless, and we need to develop, implement, and share solutions that will ultimately meet the needs and improve the outcomes for our patients. Let’s please keep our imaginative focus on why we entered this wonderful, exciting, and ever-expanding field of radiology in the first place.
About the Author
-

Keys to Creating and Maintaining a High-Functioning Team Culture
All members have a voice, that is heard
Getting your voice heard can give you so much, especially in the way of meeting others and exposing yourself to a greater audience of people, where you will have the chance to interact with a greater spectrum of culturally diverse people, much like, or different to yourself.
Wellness initiatives
Leaders of high functioning teams recognize the stresses inherent in our contemporary work environment, as well as their downstream impacts and the many manifestations of burnout. Efforts should be made to mitigate the many and ever-expanding factors contributing to stress and burnout. Recognized solutions include finding meaning in work, learning to be resilient, providing resources to support efficiency in work, and while not always practical, working less.
Additional Resources:
- A Call to Action – Our Radiology Chairs Are Burning Out
- The Road to Wellness: Engagement Strategies to Help Radiologists Achieve Joy at Work
- A Road Map to Foster Wellness and Engagement in Our Workplace
- Radiologist Burnout According to Surveyed Radiology Practice Leaders
- Burnout: Redesign the Work Process Rather Than the Person
Just culture
Just culture is a concept related to systems thinking which emphasizes that mistakes are generally a product of faulty organizational cultures, rather than solely brought about by the person or persons directly involved. In a just culture, after an incident, the question asked is, “What went wrong?
Additional Resources:
- How We Do It: Operationalizing Just Culture in a Radiology Department
- The Just Culture Framework
- Just Culture: Practical Implementation for Radiologist Peer Review
Speak up safely programs
Healthcare practitioners are expected to speak up about patient safety concerns to help intercept errors and avoid adverse patient outcomes. By ‘speaking up,’ we mean raising concerns for the benefit of patient safety and quality of care upon recognizing or becoming aware of a risk or a potential risk.
Additional Resources:
- Speak Up, Listen Up! Toolkit
- Help Prevent Errors in Your Care
- The Many Ways to Speak Up for Patient Safety
Codes of conduct
To assure a collaborative and inclusive culture, radiologists, interventional radiologists, radiation oncologists, and medical physicists should conduct themselves in a professional manner, respecting all individuals, including patients and colleagues, and advocate for those who cannot advocate for themselves.
Additional Resources:
Environment of professionalism
Medical professionalism is a belief system in which group members (“professionals”) declare (“profess”) to each other and the public the shared competency standards and ethical values they promise to uphold in their work and what the public and individual patients can and should expect from medical professionals.
Additional Resources:
- Excellence and Professionalism in Radiology
- Radiologic Professionalism in Modern Health Care
- Professionalism in Radiology: Ideals and Challenges
- Professionalism in Radiology
- The Evolution of Professionalism in Medicine and Radiology
- Designing a Curriculum for Professionalism and Ethics Within Radiology
Dignity and respect
Dignity and respect in the workplace follows the “golden rule” of treating others the way you want to be treated. A workplace where everyone shows each other dignity and respect usually has plenty of laughter, a free-flow of ideas and clear policies on expected work results and behavior.
Additional Resources:
- Setting the Stage: Why Health Care Needs a Culture of Respect
- Office of Equity Diversity and Inclusion (EDI), POLICY ON “RESPECT AND DIGNITY IN THE WORKPLACE”
Collaboration and team science
Team science is a collaborative effort to address a scientific challenge that leverages the strengths and expertise of professionals trained in different fields. Although traditional single-investigator driven approaches are ideal for many scientific endeavors, coordinated teams of investigators with diverse skills and knowledge may be especially helpful for studies of complex social problems with multiple causes.
Additional Resources:
A shared vision
Strategic planning is the process of documenting and establishing a direction—by assessing both where you are and where you’re going. The strategic plan gives you a place to record your mission, vision, and values, as well as your long-term goals and the action plans you’ll use to reach them.
Strategic planning
Strategic planning is an organization’s process of defining its strategy, or direction, and making decisions on allocating its resources to pursue this strategy. It is here that priorities are set. It may also extend to control mechanisms for guiding the implementation of the strategy.
SWOT analysis
SWOT analysis is a strategic planning technique used to help a person or organization identify strengths, weaknesses, opportunities, and threats related to business competition or project planning.
Team functions as a learning organization
Peter Senge stated in an interview that a learning organization is a group of people working together collectively to enhance their capacities to create results they really care about. Peter Senge’s 5 characteristics: systems thinking, personal mastery, mental models/open culture, shared vision and transform from individual to team learning approaches.
Additional Resources:
- Building a Learning Organization
- Peer Feedback, Learning, and Improvement: Answering the Call of the Institute of Medicine Report on Diagnostic Error
- Transitioning From Peer Review to Peer Learning: Report of the 2020 Peer Learning Summit
- Is Yours a Learning Organization?
Scenario planning
Scenario planning is making assumptions on what the future is going to be and how your business environment will change overtime in light of that future. More precisely, Scenario planning is identifying a specific set of uncertainties, different “realities” of what might happen in the future of your business.
-

Resources for Effectively Managing Radiology Personnel
Provide effective feedback
Feedback is vitally important in the workplace. It helps individuals grow and projects stay on track, and in doing so, it helps companies progress. Yet many people find giving and receiving feedback in the workplace to be totally nerve-racking. Observe a specific behavior and then explain what you observed. Tell your colleagues what kind of impact that behavior had on you, the team, and/or the organization. Provide a suggestion or an expectation for future behavior (feedforward approach), or alternatively ask how the other person wants to move forward.
Running effective meetings
An effective meeting is one where it’s objectives where accomplished within the stated timeframe. Being prepared is the most effective way to have a successful meeting.
Additional Resources:
- How To Run a Meeting
- How to Run a More Effective Meeting
- Seven Steps to Running the Most Effective Meeting Possible
People first language
People First Language is a way of communicating that reflects knowledge and respect for people with disabilities by choosing words that recognize the person first and foremost as the primary reference and not his or her disability.
Imposter syndrome
Impostor syndrome (also known as impostor phenomenon, impostorism, fraud syndrome or the impostor experience) is a psychological pattern in which an individual doubts their skills, talents or accomplishments and has a persistent internalized fear of being exposed as a “fraud”.
Improving Communication
TeamSTEPPS® is a teamwork system designed for health care professionals that is: A powerful solution to improving patient safety within your organization. An evidence-based teamwork system to improve communication and teamwork skills among health care professionals.
Ethical behavior, practices and oversight
Examples of ethical behaviors in the workplace includes; obeying the company’s rules, effective communication, taking responsibility, accountability, professionalism, trust and mutual respect for your colleagues at work. These examples of ethical behaviors ensures maximum productivity output at work.
Inter-personal support
Ubuntu can best be described as an African philosophy that places emphasis on ‘being self through others‘. It is a form of humanism which can be expressed in the phrases ‘I am because of who we all are.’
Managing internal conflict
The role of an ombudsperson is to investigate and facilitate resolution of allegations by any staff member of perceived unfair, inappropriate, discriminating or harassing treatment (behavior) by faculty, staff, administrators, or fellow students.