
It’s the age-old CXR dilemma: “I don’t want to go to CT unless I have to!” But when a potential finding appears, how do chest rads decide if it’s really real or simply a summation of shadows?
Here, we do see a nodule in the right lung. And it certainly looks discreet. Could it be an abnormality within the overlapping rib? Perhaps. Could it be something on the patient’s skin? Maybe, but probably not.

According to Travis S. Henry, MD, professor of radiology and chief of cardiothoracic imaging at Duke, his approach to focal lung disease is decidedly inquisitive.
- Is there volume loss?
- Is there lymphadenopathy?
- Is the finding chronic/recurrent?
The first line of questioning here, though? “Is there anything else?”
Finding associated abnormalities can turn a “maybe” into a “must-scan,” and in this case from Dr. Henry’s ARRS Web Lecture, a closer look reveals a huge subcarinal lymph node.
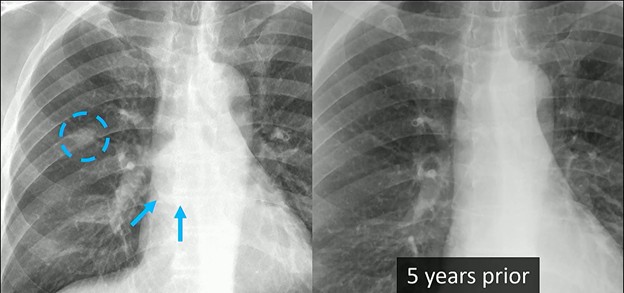
Clinical Context: The diagnostic weight of these findings increases significantly when combined with the patient’s history. This individual had a remote history of epithelioid angiosarcoma. While there was no known metastatic disease at the time, the combination of a new nodule and significant lymphadenopathy is highly concerning.
CT Correlation: Indeed, follow-up CT confirmed what the radiograph found:
- The presence of that right lung nodule.
- The massive subcarinal lymph node is clearly visible, showing exactly why the azygoesophageal interface was obscured.
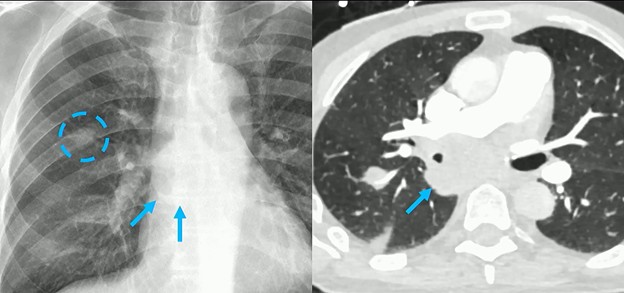
Bottom Line: Rads mustn’t look at any nodule in isolation. Always search for secondary signs or associated findings to guide your next step.
Leave a Reply