
Well over a decade since ACR’s last lexical update, BI-RADS® v2025 Manual—née Atlas—truly reflects the tech, integrating the nomenclature of digital breast tomosynthesis (DBT), automated breast ultrasound (US), and contrast-enhanced mammography (CEM). Sure, adopting this latest manual can feel like “learning a new language,” but one of v2025’s standout features is modality-neutral terminology.
Informal, food-based descriptors for mammographic calcifications have retired, too. Out: “popcorn-like” and “milk of calcium.” In: precise descriptors, such as coarse and layering. Across all modalities, mass shapes are standardized: oval, lobulated (which has been reintroduced!), round, irregular. The mammographic descriptor “microlobulated” has been removed to prevent confusion with the shape descriptor “lobulated.” It’s replaced with indistinct.
Now, let’s look at a challenging clinical scenario presented by Stamatia Destounis, MD, during the ARRS Online Course, BI-RADS 6th Edition: What’s New, What’s Not.
Presentation—A screening mammogram revealed subtle calcifications in the lateral aspect of the breast (yellow box). After magnification and stereotactic needle core biopsy, the pathology returned as atypical ductal hyperplasia (ADH), suspicious for ductal carcinoma in situ (DCIS).
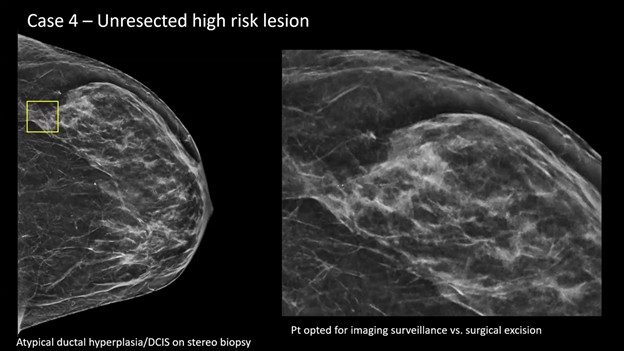
Management Dilemma—Typically, surgical consultation and excision are recommended for this pathology. However, in this case, patient and surgeon alike opted for surveillance, instead of excision.
Reporting the Follow-Up—When a patient with an unresected high-risk lesion returns for surveillance (e.g., 6 months to 1 year later), your goal is active monitoring. Step 1: identify the titanium biopsy marker (yellow box) . . .
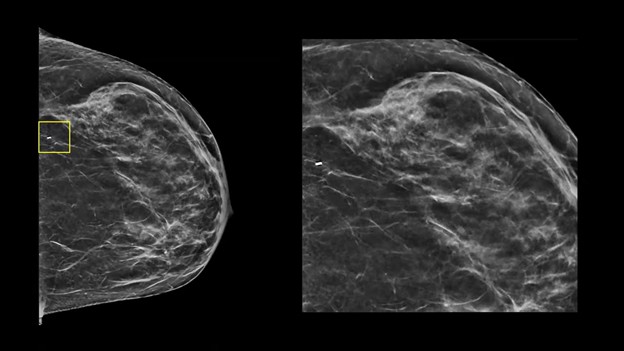
Step 2? Check for changes. Specifically, you’re looking for residual calcifications or any new areas of calcification.
II vs. IV—If the biopsy site and any residual calcifications remain stable over a designated period (as defined by your practice), you can safely assign a BI-RADS 2. Post-biopsy changes from a vacuum-assisted device are acceptable here, as long as you are comfortable with their stability.
If you see more calcifications on follow-up, you must assign a BI-RADS 4. This requires either repeating the needle biopsy or sending the patient back for a surgical excision consultation.
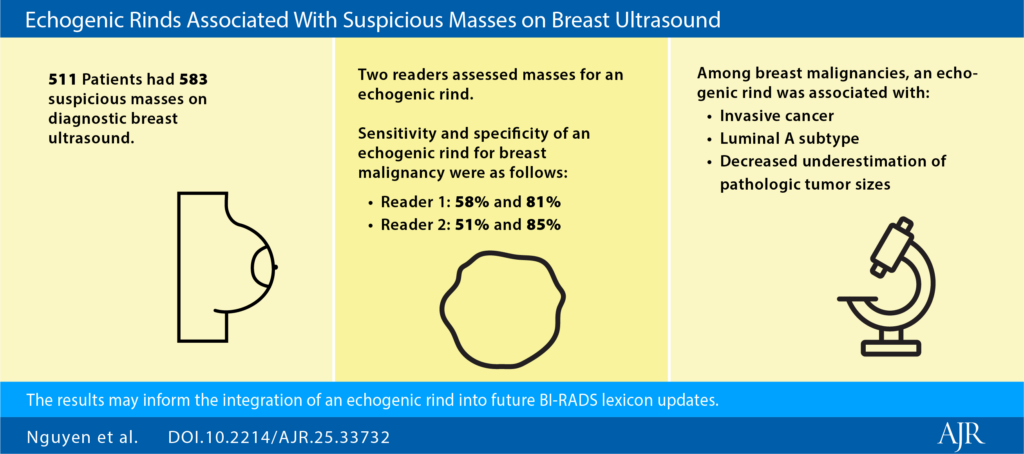
Cool To Be Rind: It’s worth noting that BI-RADS v2025 terminology now aligns more closely with contrast-based modalities via descriptors for nonmass lesions. Additionally, “echogenic rind”—a feature long known to be associated with malignancy—is officially included, with specific guidance for inclusion in your lesion measurements.
MRI & CEM Tweaks:
- No “focus”for MRI; these findings should now be categorized as either small masses or background parenchymal enhancement (BPE).
- “Multiple regions” is similarly removed for nonmass lesions, also better described as BPE.
- Give the rise of ultrafast MRI, “early phase” replaces “initial phase.”
- A new descriptor for T2-hyperintensity has been added as well.
Staging & Reporting:
- BI-RADS 6 Extent-of-Disease: This Cat 6 definition allows for additional “close findings” (within 2 cm of a known malignancy) to be included if they would not change patient management.
- Method of Detection: You are highly encouraged to document MOD to help track outcomes, demonstrate the benefits of early detection, and improve communication.
Temporal Shift: Finally, in a move toward purely morphologic assessment, descriptors that explicitly incorporate temporal change (i.e., “developing asymmetry”) have been removed. In AJR, Drs. Seely and Bissell warn that this risks underemphasizing the diagnostic importance of temporal changes, so be sure to acknowledge such in your reports for appropriate management.
Leave a Reply