
For radiologists to flag intimate partner violence (IPV) in the clinical setting, the key lies in identifying specific patterns of physical injuries that increase the likelihood of abuse. By observing combinations of target and defensive injuries—especially when they lack a consistent trauma history—rads can play a frontline role in early detection.
As Ellen X. Sun, MD, from the Trauma Imaging Research Innovation Center at Brigham and Women’s Hospital/Harvard Medical School outlined during the ARRS Web Lecture Emergency Radiology III, synchronous injuries in multiple locations without a history of major trauma are giant red flags. Common combinations include:
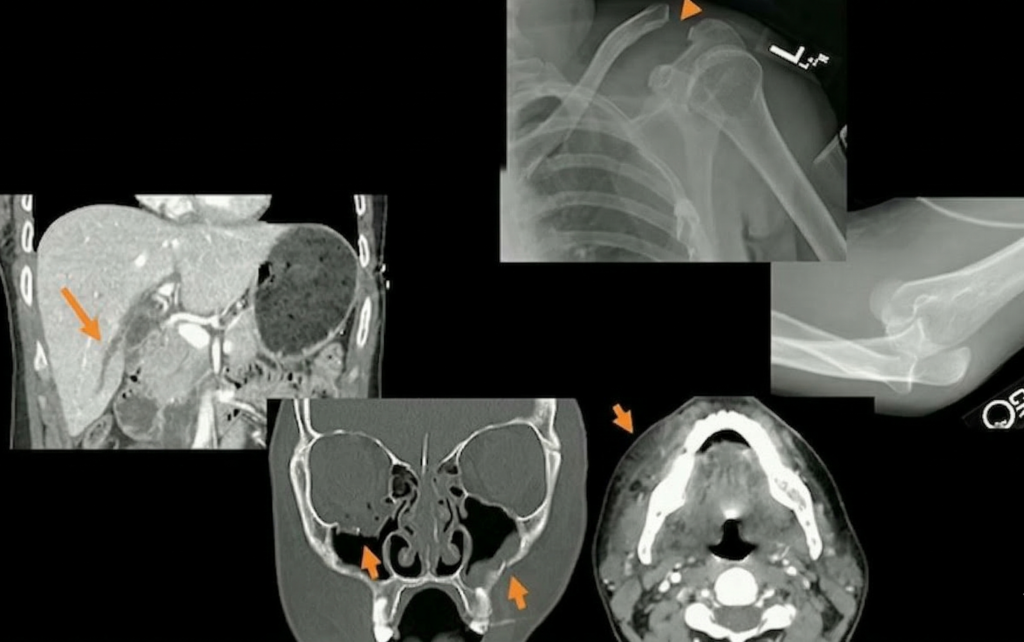
- Defensive Upper Extremity (UE) + Target Craniofacial Injuries
- Defensive UE + Target Abdominal Injuries
Dr. Sun presented a case study of a 24-year-old female patient who sustained both blunt and penetrating trauma from a partner she met on a dating app.
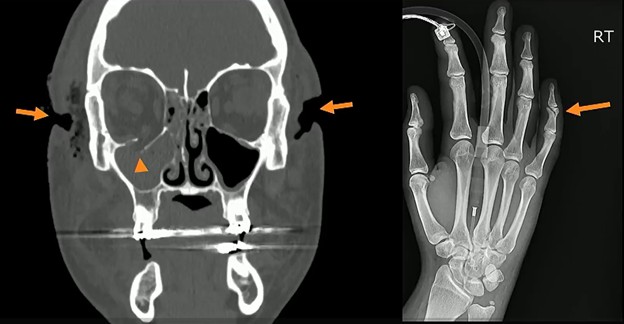
- Craniofacial: CT revealed multiple lacerations and facial fractures, including fracturing of the right orbital floor.
- Defensive: Radiography revealed a right-sided fifth middle phalangeal fracture, characteristic of defensive positioning.
Chronic Injuries: Injuries of different ages—such as the acute periorbital hematoma alongside a chronic nasal bone fracture below—are highly suspicious for repeated cycles of abuse.
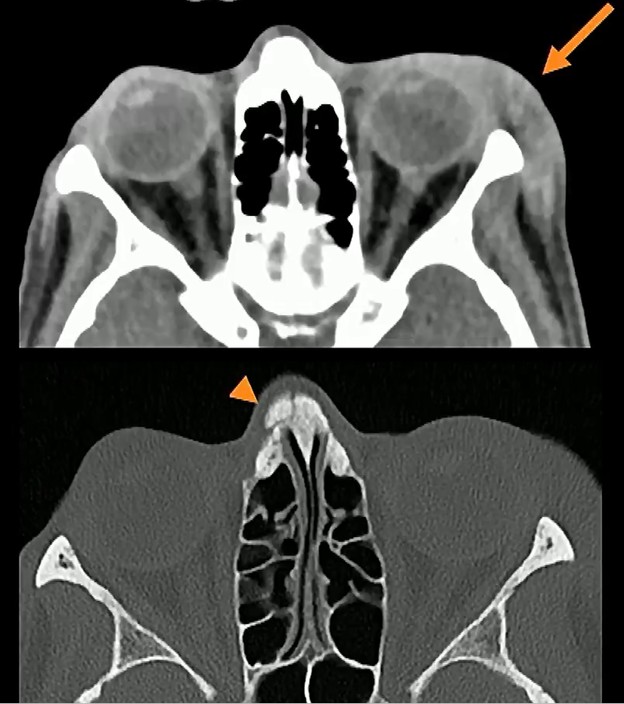
- Recurrence: Chronic fractures of the extremities and nasal bones are significantly more frequent among victims of IPV, compared to matched controls.
- Consistency: Suspicion increases when old and new injuries involve the same target or defensive side, such as the midface, hands, feet, or ankles.
Reporting Dilemma: Rads face the challenge of documenting suspicion without compromising patient safety, especially since aggressors may access federally mandated online portals. When IPV is suspected, the recommended workflow is to inform the referring physician to facilitate a private, caring conversation with the patient. If she or he confirms abuse, clinicians then need to follow institutional protocols; if patients deny it, they should still be pointed toward actionable resources.
Bottom Line: Rads can, indeed, make a difference by recognizing the high imaging use of IPV victims, injury location and imaging patterns specific to IPV, injuries inconsistent with the provided history, as well as old injuries that may be caught on physical exam.
Leave a Reply