
In the ICU, thoracic POCUS is most impactful when applied systematically. Two frameworks anchor its use in acute respiratory failure: the BLUE protocol and lung aeration scoring. Together, they provide rapid diagnosis and quantitative monitoring.
BLUE Protocol Structures Diagnosis: The Bedside Lung Ultrasound in Emergency (BLUE) protocol, developed by Lichtenstein and Mezière, standardizes lung ultrasound evaluation in patients presenting with acute respiratory failure. Core elements include:
- Assessment of 2–3 predefined points per hemithorax
- Identification of key sonographic patterns:
- A-lines (normal aeration)
- B-lines (interstitial syndrome)
- Absent lung sliding
- Consolidation
- Adjunct venous ultrasound when pulmonary embolism is suspected
Rather than scanning the entire thorax, the protocol focuses on reproducible anatomical windows and interprets artifact patterns within a diagnostic algorithm. Validation studies report approximately 90.5% diagnostic accuracy in acute respiratory failure. BLUE’s strength lies in speed and structure, transforming artifact recognition into actionable bedside triage.
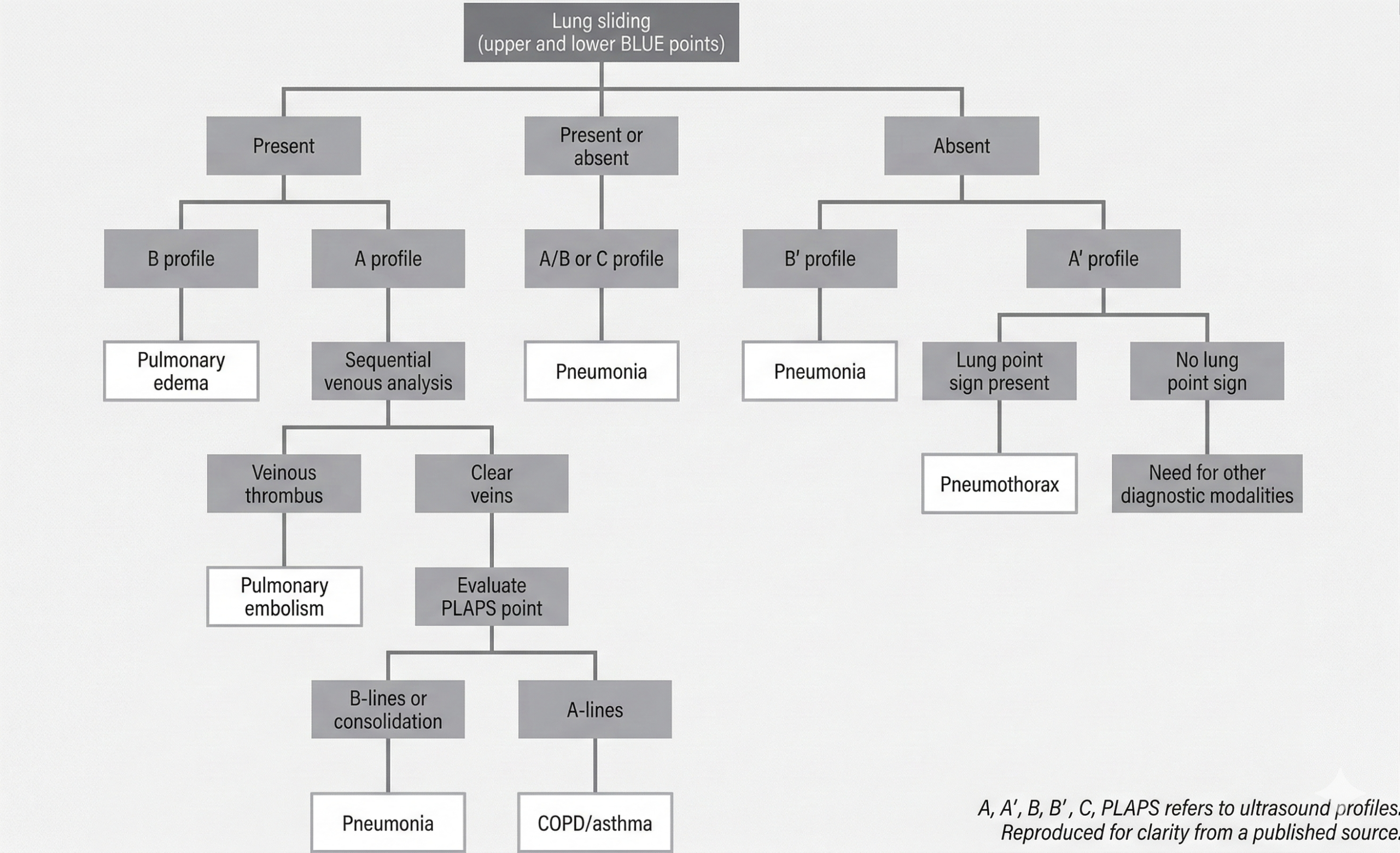
Chart summarizes bedside lung ultrasound emergency (BLUE) protocol as applied to patients with undifferentiated respiratory failure. This protocol includes two to three points: upper BLUE point (anterior below clavicle), lower BLUE point (anteriomedial between nipple and anterior axillary line), and posterior lateral alveolar/pleural syndrome (PLAPS) point (behind posterior axillary line at level of lower BLUE point). Diagnoses are indicated in white boxes. Designation of A profile means fewer than three B-lines are present in all imaged points and ultrasound is considered normal. B profile means more than three B-lines are present in multiple points and ultrasound is suggestive of pulmonary edema. C profile indicates consolidation, typically pneumonia. B’ profile indicates absent lung sliding with present B-lines, which suggests pneumonia. A’ profile indicates lack of lung sliding or B-lines suggesting pneumothorax. A/B profile indicates mix of A- and B-lines and suggests pneumonia.
Lung Aeration Assessment Quantifies Disease Burden: While the BLUE protocol classifies pathology, lung aeration scoring quantifies severity. This scoring system grades each lung region as follows:
- 0: A-lines or fewer than three B-lines (normal aeration)
- 1–2: Increasing B-line burden (partial loss of aeration)
- 3: Consolidation (complete loss of aeration)
Six regions per lung are evaluated, yielding a cumulative score from 0 to 36. Clinical applications include:
- Monitoring pulmonary edema and response to diuresis
- Assessing ventilator-associated pneumonia
- Guiding PEEP adjustments
- Predicting post-extubation respiratory distress
This approach enables longitudinal tracking. Instead of asking, “Is there edema?” clinicians can ask, “Is aeration improving?”
Complementary Roles: The two systems serve distinct but complementary purposes:
- BLUE protocol → Rapid etiologic diagnosis
- Aeration scoring → Severity assessment and treatment monitoring
Together, they represent a shift from qualitative bedside imaging to structured, reproducible, and semi-quantitative critical care ultrasound.
Clinical Takeaway: When applied correctly, thoracic POCUS is not an ad hoc scan; it is protocol-driven medicine. The BLUE protocol accelerates diagnosis in respiratory failure, whereas lung aeration scoring measures trajectory. In the ICU, this combination can change management within minutes.
Leave a Reply