
The Problem: Traditional CTA is a structural map. It tells you there is a fallen tree on the road (i.e., the clot), but it doesn’t always tell you if the traffic has stopped (i.e., the perfusion). In subsegmental disease or “dirty” scans with beam-hardening artifacts, structural-only imaging leaves radiologists in the equivocal trap.
The Fix? As the ARRS Online Course “Practical Dual-Energy CT Throughout the Body” points out, by pairing iodine quantification with anatomical imaging, rads can move from searching for filling defects to visualizing physiologic impact.
The Breakdown—A multi-vector look at a left subsegmental PE...
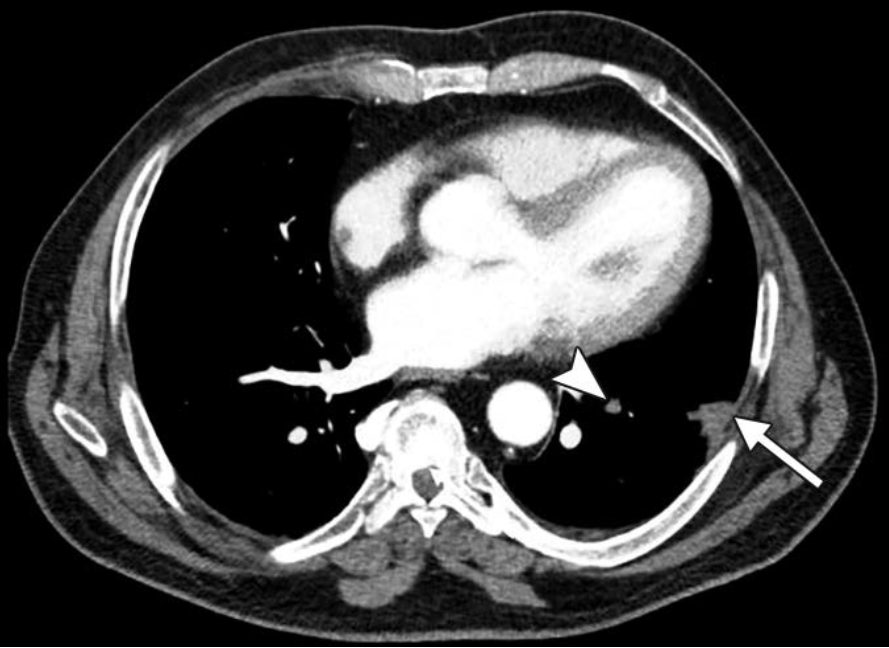
Standard Blended—We see the “What.” A classic peripheral wedge-shaped opacity: Hampton Hump (solid arrow). There is a subtle luminal filling defect in the feeding vessel (arrowhead), but in a motion-degraded scan, you might doubt it.
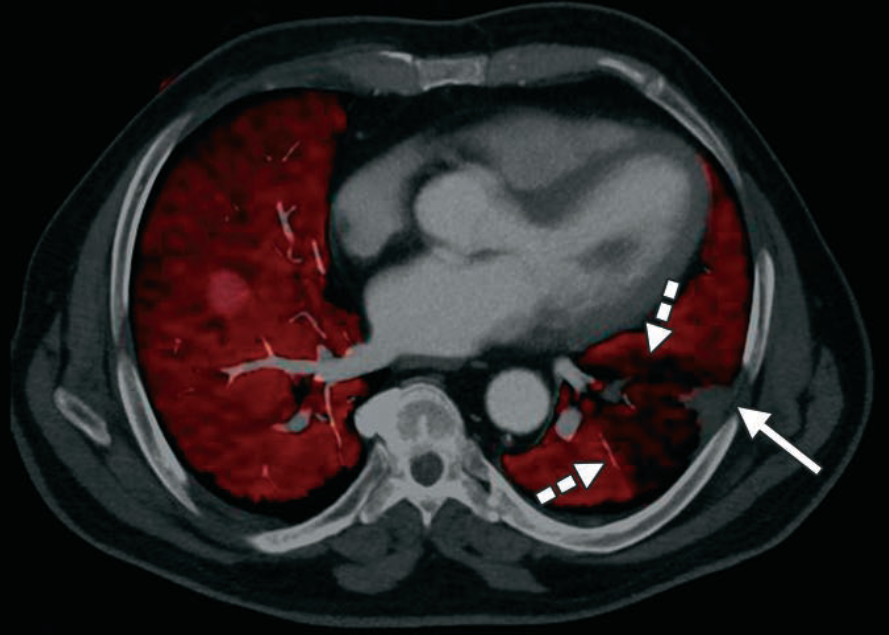
Iodine Map—We see the “So What.” The red overlay represents iodine concentration. The dashed arrows highlight a perfusion “cold zone.” This wedge-shaped defect provides orthogonal confirmation that the clot isn’t just an artifact; it’s a functional obstruction.
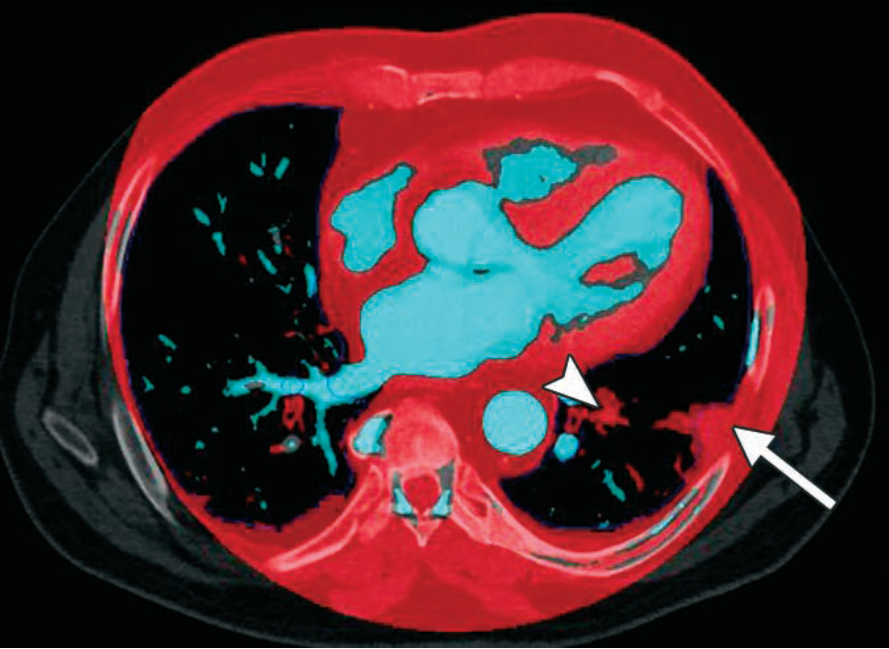
Vessel Analysis—This reconstruction isolates iodine signal. Note the iodine dropout (arrowhead) within the artery. This removes the noise of the lung parenchyma to focus strictly on the continuity of the blood column.
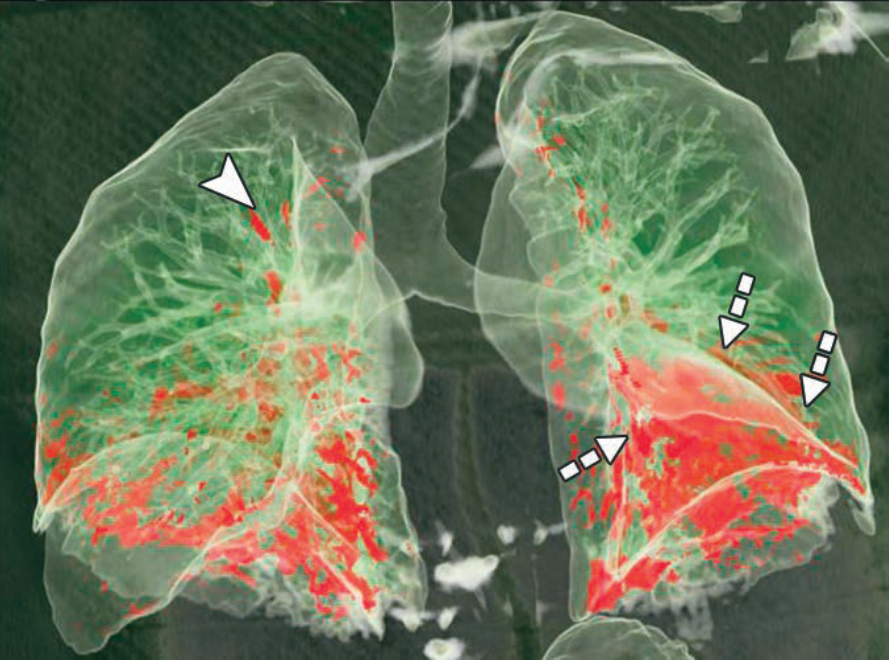
3D Perfusion—The “Global Impact.” This 3D volume rendering maps the total territory of the ischemic lung (red zones). It’s the visual shorthand for clinical severity.
Push for DECT in Your PE Protocol?
- Tie-Breaker: Small distal clots are often equivocal. If you see a corresponding wedge-shaped perfusion defect on the iodine map, your confidence in calling a subsegmental PE jumps from “possible” to “definitive.”
- Artifact Insurance: Beam hardening from dense contrast in the SVC often obscures the right upper lobe. DECT iodine maps help differentiate true clots from “pseudo-filling defects” caused by photon starvation.
- Infarct Prediction: A Hampton Hump is a late sign of infarction. DECT identifies the ischemic penumbra (the area at risk) before it potentially progresses to permanent tissue death.
Bottom Line: DECT transforms PE imaging from a binary search (clot vs. no Clot) into a physiologic assessment (obstruction + ischemia). Result? Fewer “equivocal” reports and higher diagnostic defensibility.
Leave a Reply