Dual-energy CT (DECT) is becoming a must-use tool in musculoskeletal (MSK) imaging—not just for hardware, but for crystals, marrow, and trauma. Orthopedic imaging often suffers from two problems: metal streak and ambiguous density. But as the ARRS Online Course “Practical Dual-Energy CT Throughout the Body” duly notes, DECT tackles both by separating materials and controlling photon energy, giving rads clearer views of bone, soft tissue, and implant interfaces.
Where Does DECT Make the Biggest Difference?
Metal Artifact Reduction (MAR) That Actually Works
High-keV VMIs (110–150 keV) reduce photon starvation and scatter from:
Spine instrumentation
Hip and knee arthroplasties
Fracture fixation hardware
Shoulder anchors
Result: cleaner cortices, more visible fractures, and better evaluation of infection or loosening.
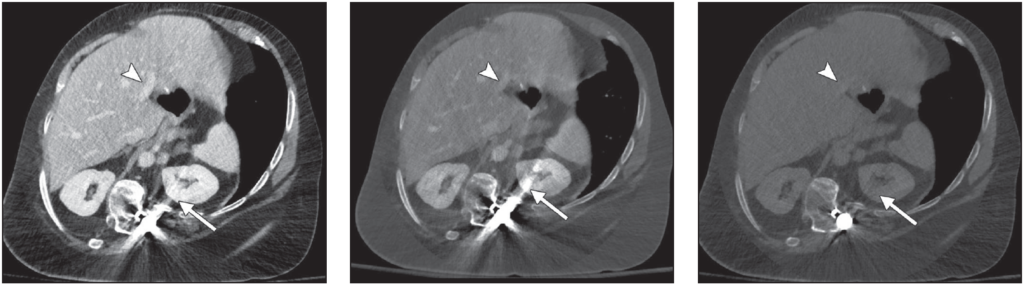
Portal venous phase abdominal CT images obtained after spinal reconstruction surgery. Left, Normal blended image shows considerable amount of metal artifact (arrow) overlaying left kidney and good contrast in portal veins (arrowhead). Center, Virtual monoenergetic image of same slice shown in Left, obtained at 50 keV, shows high portal venous contrast (arrowhead) and high amounts of metal artifact (arrow).Right, Virtual monoenergetic image of same slice shown in Left, obtained at 150 keV, reveals decreasing amounts of metal artifact (arrow) and loss of portal venous contrast (arrowhead).
2. Crystal Imaging: Knowing Exactly What You’re Looking At
Material decomposition differentiates uric acid from calcium, which helps:
Confirm gout even in unusual locations (spine, tendons, postoperative joints)
Distinguish gout from infection or tumor
Map tophus burden for treatment decisions
Patient with suspected tophus of first interphalangeal joint caused by gout. Left, Mixed CT image that is equivalent to single-energy scan acquired at 120 kVp shows tophus (arrowhead). Right, Material decomposition image applied to highlight urate crystals (green area indicated by arrowhead) confirms that lesion seen on regular CT scan is tophus caused by gout.
3. Bone Marrow Edema Detection
DECT water-specific reconstructions reveal bone marrow edema in trauma, stress injuries, and arthritis (especially helpful when MRI is unavailable or contraindicated).
Why Are MSK Rads Adopting DECT?
Saves nondiagnostic postoperative studies
Improves fracture conspicuity
Reduces MRI dependence
Helps differentiate infection, inflammation, and crystal deposition
Speeds up decision-making for orthopedic surgeons
Bottom Line: MSK DECT is no longer just “nice to have.” When hardware, crystals, or marrow ambiguity stand in the way, DECT gives you answers a conventional CT simply can’t.
PSA screening alone lacks specificity, leading to substantial overbiopsy and detection of indolent disease. Nomograms—multivariable risk calculators—were developed to move prostate cancer assessment beyond single thresholds. As Drs. Benjamin Tran, Janelle T. West, Soroush Rais-Bahrami, and Kristin K. Porter noted in their ARRS Online Course, the most effective tools integrate clinical variables with mpMRI, making rads central to risk stratification rather than downstream reporters.
Why Nomograms Matter: Traditional PSA-based decision-making treats all patients similarly despite wide variation in underlying risk. Nomograms combine multiple predictors—PSA, prostate volume, digital rectal exam, age, biopsy history, and increasingly PI-RADS assessment—to estimate an individual’s probability of harboring clinically significant prostate cancer (csPCa).
Multiple studies show that nomograms incorporating MRI outperform PSA alone and MRI alone, improving discrimination while safely reducing unnecessary biopsies.
mpMRI’s Role: mpMRI is not just an add-on variable; it is a dominant driver of modern risk models. PI-RADS category, lesion size, and PSA density materially alter predicted risk.
MRI-integrated nomograms consistently achieve AUCs in the 0.80–0.88 range for csPCa detection, while reducing biopsy rates by 20–34% depending on the population and risk threshold chosen. In practical terms, this means fewer low-yield biopsies without a clinically meaningful increase in missed aggressive cancers.
For rads, this elevates the importance of:
Accurate PI-RADS categorization
Consistent prostate volume measurement
Clear reporting of lesion location and size
Small changes in PI-RADS score can significantly shift nomogram output and clinical decision-making.
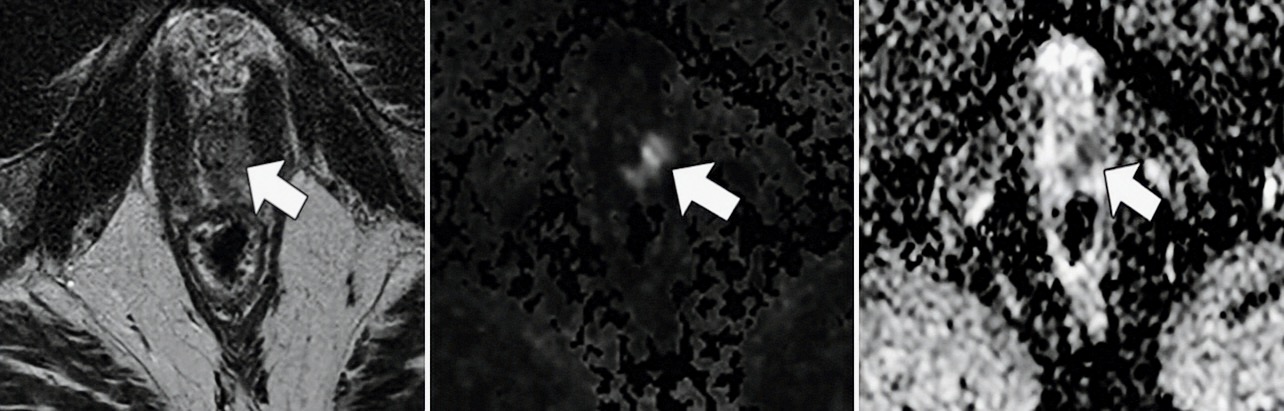
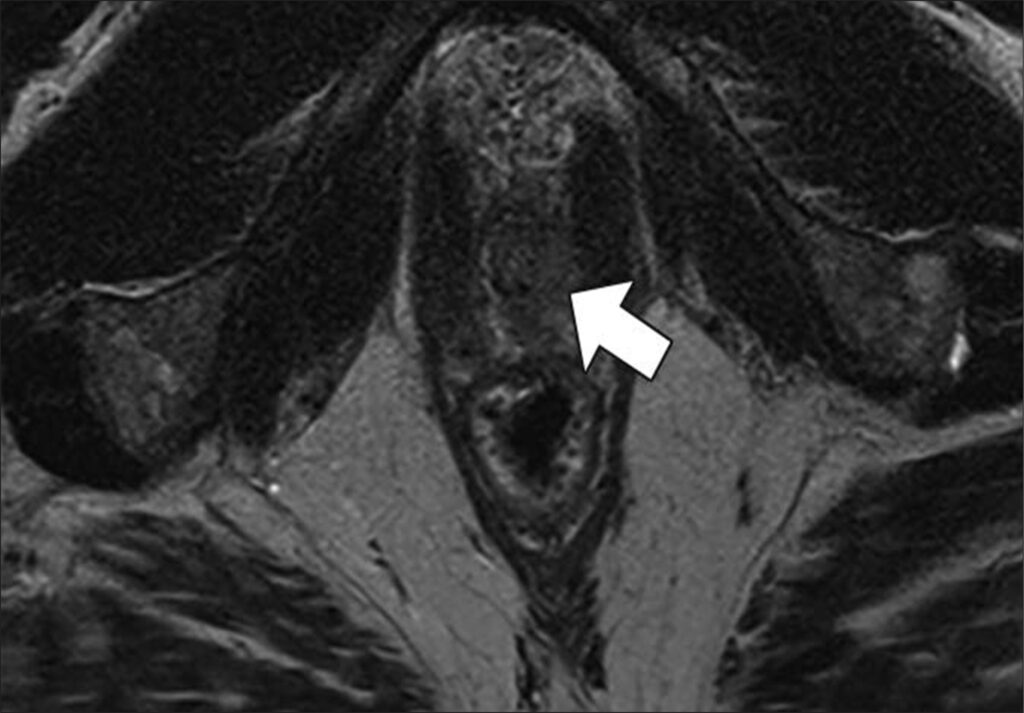
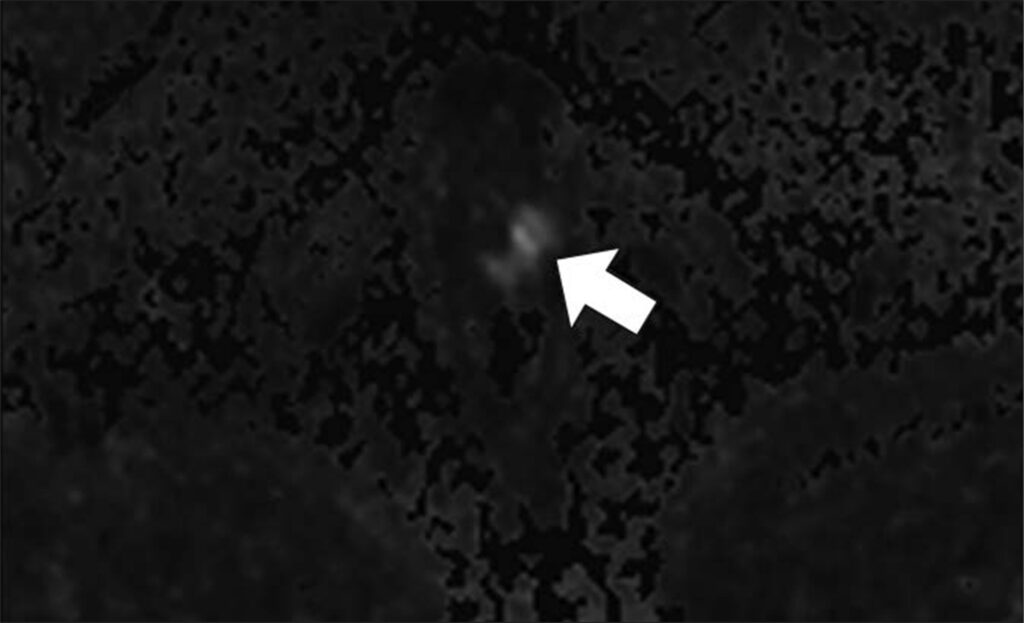
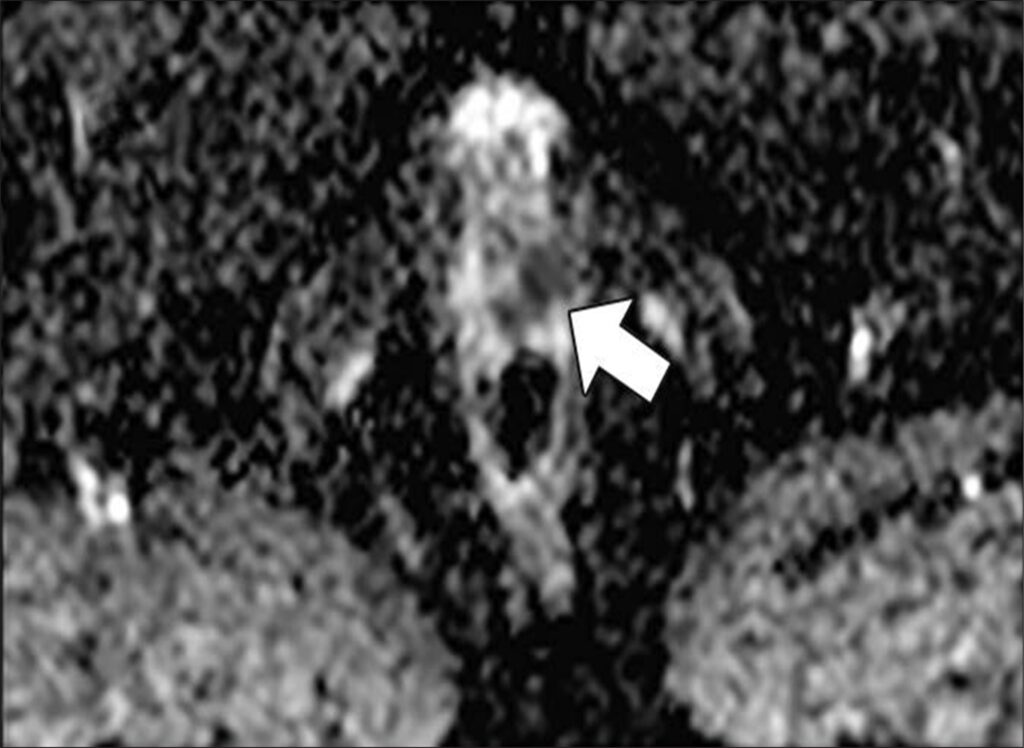
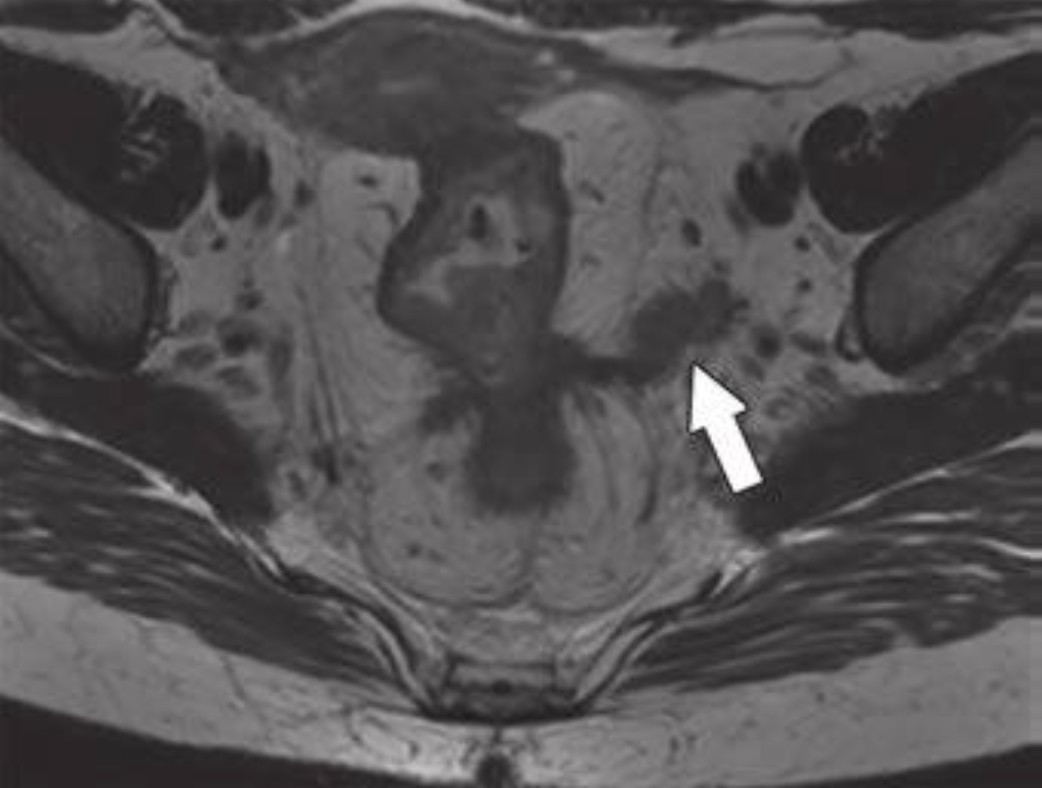
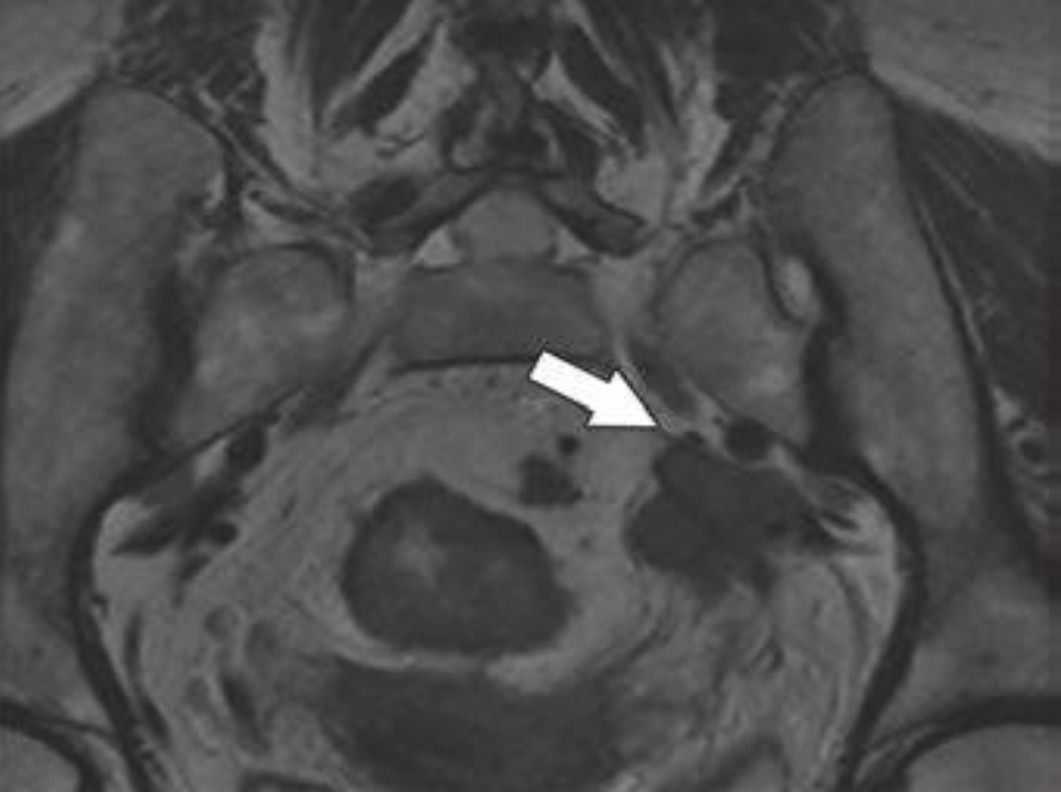
47-year-old man with history of two negative systematic biopsies at another facility and increasing PSA level (most recently, 35.6 ng/mL). Multiparametric MRI was performed for persistent clinical suspicion of clinically significant prostate cancer
Top to Bottom: Axial T2-weighted (Top), axial high-b-value (2000 s/mm2) (Middle), and calculated ADC (Bottom) MR images show left apical anterior central gland lesion (arrow) with very high suspicion of being clinically significant prostate cancer. Lesion is PI-RADS category 5. MRI–transrectal ultrasound fusion biopsy of lesion resulted in pathologic diagnosis of prostatic adenocarcinoma, Gleason 4 + 3 = 7 (grade group 3). Gleason 4 pattern represents 60% of tumor. Prostate volume calculated with MRI is 40 mL.
PSA Density—A Critical Modifier: PSA density (PSAD) is one of the most powerful adjuncts to PI-RADS. In patients with PI-RADS 1–2 or equivocal PI-RADS 3 lesions, PSAD meaningfully improves negative predictive value—often approaching 90%—and helps identify patients who can safely avoid biopsy.
This is especially relevant in biopsy-naïve men, where avoiding the first biopsy carries the greatest downstream benefit.
Matching Nomogram and Patient: No single nomogram fits every clinical scenario. Some are optimized for biopsy-naïve patients, others for men with prior negative biopsy, and some for mixed cohorts. Understanding these distinctions prevents misapplication and overconfidence in a single risk estimate.
Another important limitation is population dependency. Many widely used nomograms were derived from European or predominantly White cohorts. Without external validation, these tools may overestimate risk in Asian populations and other underrepresented groups. Local calibration and clinical judgment remain essential.
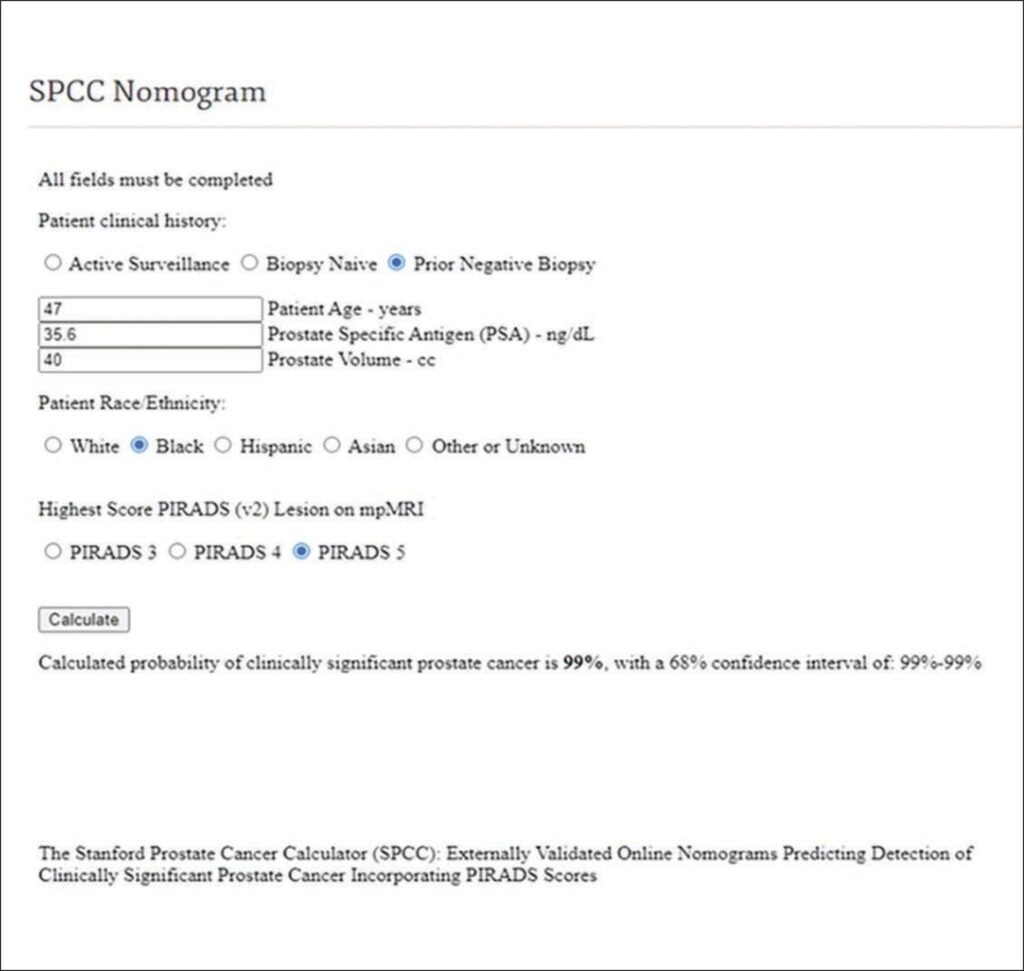
47YO man with two negative systematic biopsies (same patient)
Screenshot of Stanford Prostate Cancer Calculator (SPCC) nomogram calculation shows 99% probability of clinically significant prostate cancer before repeat biopsy. This prediction can be shared with patient during counseling about recommendation for repeat biopsy. Result of repeat MRI– transrectal ultrasound fusion biopsy was consistent with prostatic adenocarcinoma: Gleason 4 + 3 = 7 (grade group 3). Gleason 4 pattern represented 60% of tumor.
What Does This Mean for Rads? Nomograms reposition rads as active participants in prostate cancer decision-making. High-quality MRI interpretation directly influences whether a patient undergoes biopsy, surveillance, or reassurance.
In multidisciplinary care, radiologists who understand nomogram inputs and limitations can:
Explain risk estimates to urologists with confidence
Support biopsy deferral when appropriate
Improve alignment between imaging findings and management
Nomogram / Calculator
Best Use Case
Key Inputs
Strengths
Limitations
MRI-ERSPC RC3 / RC4
Biopsy-naïve patients
PSA, PSAD, DRE, prostate volume, PI-RADS
Strong external validation; good balance of biopsy reduction and csPCa detection
Derived largely from European cohorts
ModRad
Biopsy-naïve patients
PSA, PSAD, PI-RADS, clinical variables
High discrimination; MRI-forward design
Less validated in prior biopsy populations
ModDis
Prior negative biopsy
PSA, PSAD, PI-RADS, biopsy history
Reduces repeat biopsies while maintaining csPCa sensitivity
Less applicable to biopsy-naïve patients
Stanford Prostate Cancer Calculator
Mixed populations
PSA, DRE, biopsy history, MRI findings
Broad applicability; flexible inputs
Slightly lower performance than MRI-specific models
PCPT Risk Calculator
Legacy / screening context
PSA, age, race, DRE
Historically influential
Does not incorporate MRI; lower specificity
ERSPC (non-MRI)
Screening populations
PSA, DRE, prostate volume
Well studied
Outperformed by MRI-integrated tools
Bottom Line: mpMRI-integrated nomograms transform prostate cancer assessment from threshold-based screening to personalized risk prediction. Radiologists who deliver precise PI-RADS scoring and understand how those scores drive nomograms add measurable, patient-level value.
The American College of Radiology (ACR) is sounding the alarm for hospital-based imaging providers: a recent, massive pay increase for Coronary CT Angiography (CCTA) is at risk of being revoked unless facilities change how they bill for these services.
Big Picture: In its 2025 final rule, CMS temporarily moved CCTA (CPT 75572–75574) from a Level 1 to a Level 2 Ambulatory Payment Classification (APC).
The Windfall: Technical fees jumped 104%, rising from $175 in 2024 to $357 currently.
The Catch: CMS made this change “provisionally.” If fewer than 50% of hospitals update their billing to reflect the true resource intensity of CCTA, Medicare will revert to the lower, generic CT payment rates.
CY 2024APC 5571
CY 2025APC 5572
% Change
Hospital Outpatient (OPPS)
$175
$357
+104%
Physician Office (PFS)
$285
$318
+12%
The Friction: Historically, hospitals were forced to use a generic “CT Scan” revenue code (0350), which has a lower cost-to-charge ratio. CMS has now removed the “Return to Provider” edits that blocked hospitals from using more accurate codes.
Action Items:To make the pay hike permanent, the ACR, American College of Cardiology, and Society of Cardiovascular Computed Tomography all recommend:
Update Charge Masters: Map CCTA CPT codes to Cardiology (0480/048x) or Other Imaging Services (040x) revenue codes.
Reflect Intensity: Reporting costs under these specific codes demonstrates the specialized nursing and resource needs that justify the higher APC level.
Monitor Denials: Ensure clearinghouses and private payers accept the updated cardiology revenue codes.
Bottom Line: If facilities continue to report CCTA expenses as identical to generic CT scans, the data will fail to support the higher payment level, and the $182-per-scan “bonus” will vanish.
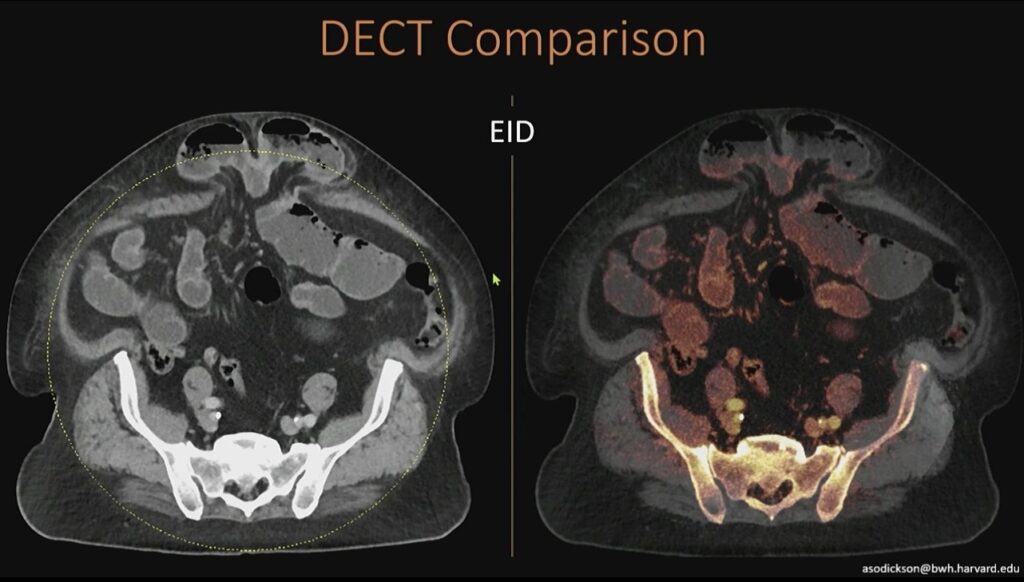
Dual-energy CT (DECT) has become a workhorse in emergency imaging, particularly for iodine mapping and virtual noncontrast applications. But as Aaron Sodickson, MD, reveals in a presentation now available in the ARRS Quick Bytes library, conventional DECT systems come with a quiet limitation: dual-energy information is not uniformly available across the entire field of view. Photon-counting CT (PCCT) changes that.
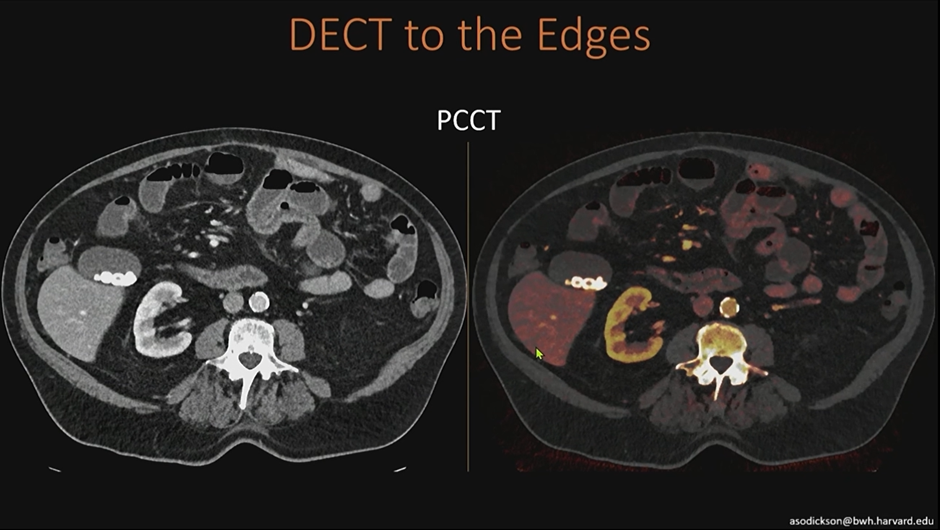
Left: What you see here is that on our existing high-end dual-energy scanners, we have a slight limitation, which is that we don’t get dual-energy information outside this yellow-dotted circle. Right: While we have iodine content centrally, we don’t have anything out in the periphery.
There Are Limits: On many high-end dual-energy scanners, iodine maps are only reliable within a central circular region. Outside that area, dual-energy information is lost. In large patients or peripheral anatomy, this can mean incomplete iodine characterization and diagnostic uncertainty.
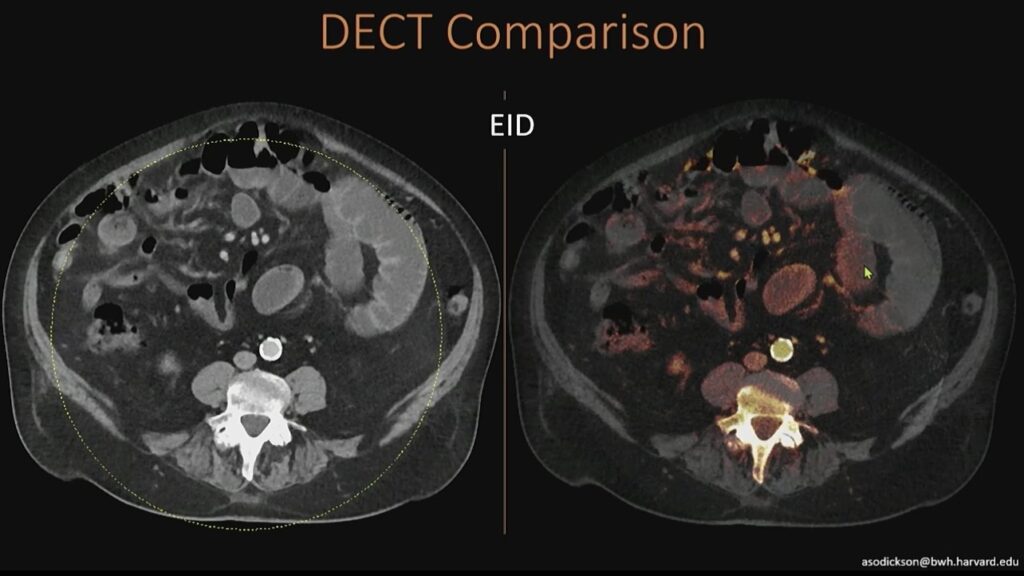
Here’s another example of the same thing, where you can see that we’ve lost our information out at the edges.
In practice, you may see clean iodine signal centrally, but nothing at the edges—simply because the system cannot acquire dual-energy data beyond that geometric constraint.
PCCT Is Built Different: PCCT acquires spectral information directly at the detector. Because it does not rely on paired detector geometries or source-based separation, dual-energy information is available across the entire field of view, meaning:
Iodine maps extend fully to the periphery
Large patients no longer fall outside the dual-energy zone
Edge anatomy benefits from the same spectral data as the center
In the ED, where patient size and positioning are unpredictable, this matters.
On the photon-counting scanner, all of this dual-energy information content is acquired at the detector, so we don’t geometrically need the two CT detectors that are being used in our conventional scanner. Thus, we can get dual-energy information all the way out to the edges, even in large patients outside that field of view.
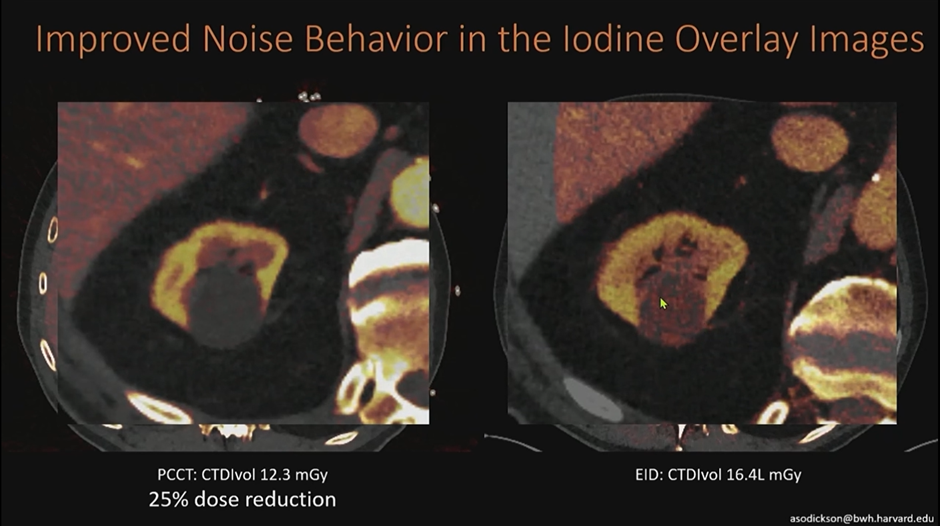
Better-Behaving Noise: Another practical advantage of PCCT is cleaner iodine post-processing. DECT maps may show speckled signal in non-enhancing structures—algorithmic noise that can mimic low-level enhancement.
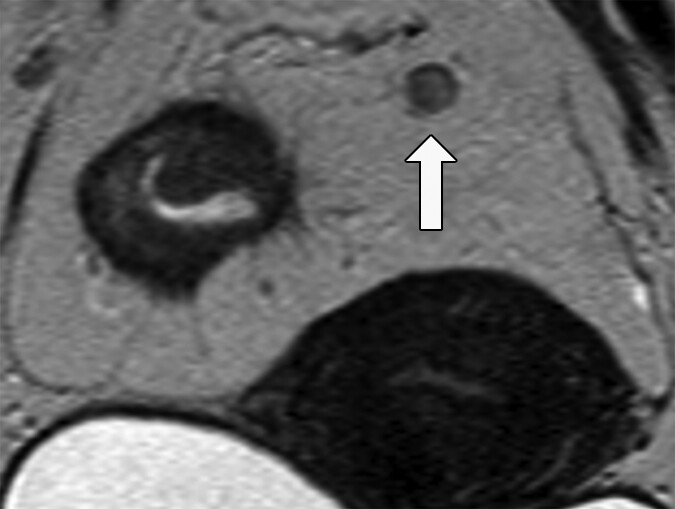
In this example below of a renal cyst, conventional DECT shows scattered orange signal that is not true enhancement. On PCCT, that noise is substantially reduced, allowing confident classification of a benign, non-enhancing complex cyst.
Looking at this renal cyst on a conventional scan, you see some noise in the iodine post-processing content (e.g., green arrow in orange speckle). There isn’t actually enhancement within this cyst; this is noise in the algorithm. On the photon-counting scanner, we’re able to knock down that noise to see much more cleanly that this is a non-enhancing, benign, complex cyst.
Why This Matters in the ED: Emergency radiology rewards speed and certainty; PCCT improves both by:
Preserving iodine data across entire image
Reducing false-positive enhancement
Increasing confidence in lesion characterization
Decreasing need for follow-up imaging
Bottom Line: Photon-counting CT removes the “edge problem” of conventional DECT. By delivering full-field spectral data with improved noise characteristics, PCCT strengthens iodine-based interpretation—exactly where ED imaging needs it most.
Fatty liver has become so common that trainees often see steatosis more frequently than a normal liver. During the latest AJR Forum on Quantitative Ultrasound, David Fetzer, MD, asked Roentgen Fund recipient Theodore Pierce, MD, a practical question regarding liver fat assessment:
Are practices billing for liver fat quantification, and is it performed alone or bundled with other exams?
The Big Picture
Liver fat quantification is increasingly embedded in routine abdominal imaging. But billing practices, reimbursement, and workflow integration vary widely across institutions. Dr. Pierce noted that while they do code and submit billing for fat quantification, reimbursement remains inconsistent at this stage.
Key Takeaways
Billing is performed, even though reimbursement is not yet reliable. Fat quantification is coded whenever performed. Reimbursement is infrequent but expected to improve as adoption grows and payers recognize the clinical value.
Standalone liver fat quantification exists, but it is rarely used. Although offered as its own CPT-coded exam, most clinicians prefer to order it in combination with either a limited right upper quadrant ultrasound or with both RUQ ultrasound and elastography. The combination is determined by the referring clinician and the specific clinical question.
Interpretation requires clinical and imaging context. As Dr. Fetzer emphasized, fat quantification values are interpreted alongside B-mode appearance and elastography stiffness to evaluate steatosis, fibrosis, and inflammation. The combined data provide a more accurate assessment than any single technique alone.
Bottom Line
Liver fat quantification is billable, clinically valuable, and most informative when paired with RUQ ultrasound and elastography. Utilization is increasing, reimbursement frameworks are evolving, and the technique is moving toward becoming a routine component of hepatic imaging.
In smaller hospitals, choosing between ultrasound or upper GI for suspected malrotation can feel high-stakes. During the latest AJR Live Webinar, Jonathan Dillman, MD, and HayThuy Nguyen, MD, tackled a key question:
Should community hospitals perform both ultrasound and upper GI—or is one enough before transferring a child?
The Big Picture
Even though ultrasound for midgut volvulus performs incredibly well in published studies, your institutional comfort and consistency matter. Smaller centers may see fewer neonates, and that affects how confident technologists and radiologists feel with real-time sonographic anatomy.
Dr. Nguyen’s advice: Start with both. Build confidence. Then taper.
Key Takeaways
Ultrasound + Upper GI Can Be Complementary, At First
Even at large centers, both exams are often paired early on.
Not because ultrasound underperforms, but because every institution needs their own “local data.”
Once your team demonstrates consistently accurate ultrasound performance, you can safely drop routine upper GI.
See a Whirlpool Sign? Call Surgery!
A positive whirlpool sign on ultrasound is highly specific. No need to wait for additional imaging; direct referral to pediatric surgery is appropriate.
No Whirlpool, but Symptoms Persist → Consider Upper GI or Transfer
Ultrasound may still be equivocal in some infants. Upper GI remains a helpful confirmatory test when the diagnosis is uncertain but suspicion stays high.
Don’t Forget: CT or MRI Can Make the Diagnosis for Older Kids
Dr. Dillman emphasized that adolescents or older children being scanned for unrelated reasons may still show:
SMV/SMA reversal
Swirling mesentery
Engorged mesenteric vessels
Collaterals
Even a noncontrast CT for renal stone can incidentally reveal the vascular swirl. MRI—especially rapid MR protocols—can also depict abnormal vascular orientation.
Bottom Line
Start with both ultrasound and upper GI, if your institution needs to build confidence. Once your team demonstrates reliable ultrasound performance, ultrasound alone is often sufficient…and a positive whirlpool sign should trigger immediate surgical evaluation.
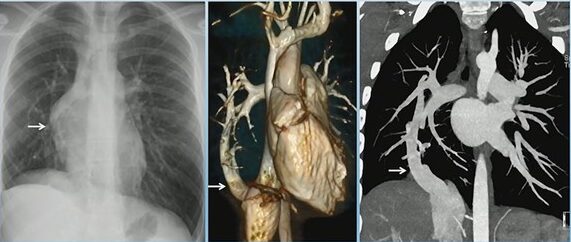
Scimitar syndrome represents a distinctive form of right lung partial anomalous pulmonary venous return. It is classically associated with right lung hypoplasia, abnormalities of the right pulmonary artery, and a characteristic anomalous vein draining into the systemic venous system. As Abbey J. Winant, MD, MFA, illustrates in “Pediatric Thoracic Vascular Disorders: Congenital to Acquired Pathology,” CTA plays a central role in defining venous anatomy and identifying associated anomalies.
What Defines Scimitar Syndrome?
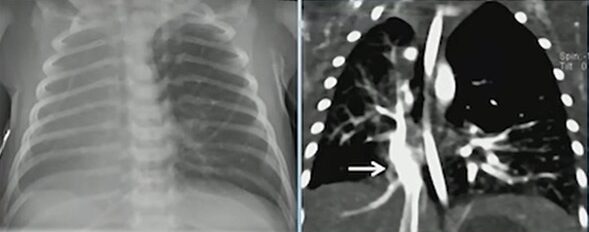
Scimitar syndrome (RLL PAPVR) with R Lung hypoplasia
The hallmark is a right lower lobe pulmonary vein draining anomalously—most often into the inferior vena cava, but occasionally into the inferior right atrium. This vein produces the classic “scimitar” appearance on chest radiography and cross-sectional imaging. Children often have concurrent right lung hypoplasia, which alters airway and vascular proportions.
Scimitar Syndrome (“Scimitar Vein”)
Recognizing Associated Findings
In addition to partial anomalous pulmonary venous return, scimitar syndrome often presents with:
Hypoplastic right lung
Hypoplastic right pulmonary artery
Systemic arterial supply to portions of the right lung
Bronchial abnormalities, including bronchiectasis
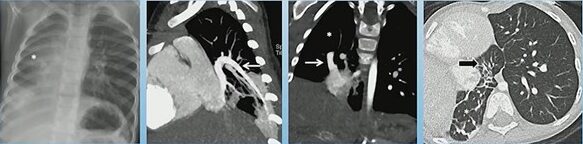
Scimitar Syndrome with Horseshoe Lung: Hypoplastic right lung, PAPVR to RA, horseshoe lung, R lung bronchiectasis
One of the most notable associations is horseshoe lung, seen in approximately 80% of cases. Horseshoe lung consists of a parenchymal isthmus connecting both lungs across the midline, usually posterior to the heart. When present, it further reinforces the diagnosis and alerts the radiologist to search for additional congenital anomalies.
Additional Congenital Abnormalities to Consider
Although not seen in every case, associated developmental abnormalities may include:
Extralobar sequestration
Vertebral anomalies
Diaphragmatic defects
Cardiac malformations
Their presence can significantly influence management, operative planning, and follow-up.
Why Does CTA Matter?
CTA provides the most comprehensive view of the venous drainage pattern, systemic arterial contributions, and bronchial architecture. It allows precise localization of anomalous veins and helps differentiate scimitar syndrome from other types of partial anomalous pulmonary venous return.
Bottom Line
Scimitar syndrome is more than an anomalous pulmonary vein. Its constellation of findings—right lung hypoplasia, anomalous venous return, and frequent association with horseshoe lung—requires careful, structured evaluation. CTA remains the best tool to clarify anatomy and guide clinical management.
Large language models (LLMs) are reshaping radiology, but their integration into the reading room is far from straightforward. 2026 ARRS Annual Meeting Categorical Course Director Yee Seng Ng, MD, outlines the most significant barriers to adoption and why the solutions are more complicated than they appear.
Security Slows Adoption
Most widely available LLMs live on proprietary cloud platforms. Sending protected health information (PHI) outside a hospital network creates immediate compliance issues, and current guidelines from major organizations explicitly prohibit using public LLMs for protected patient information. Even if models claim not to store or reuse data, rads cannot verify how patient information is handled, refined, or monetized.
Private Solutions, But Not for All
Institutions can build private LLM instances behind their firewall, but this requires substantial infrastructure, IT support, and vendor partnerships—resources generally limited to large academic centers. Local installations using open-source models (via interfaces such as webUI) avoid cloud exposure but introduce new challenges: maintenance, computing requirements, and accessibility across the department.
Where Is NLP Already Helping?
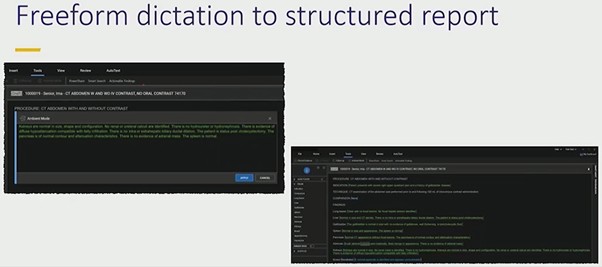
Even though LLMs aren’t widely used at the point of care, rads are already benefitting from improved natural language processing (NLP) embedded in commercial reporting tools, including
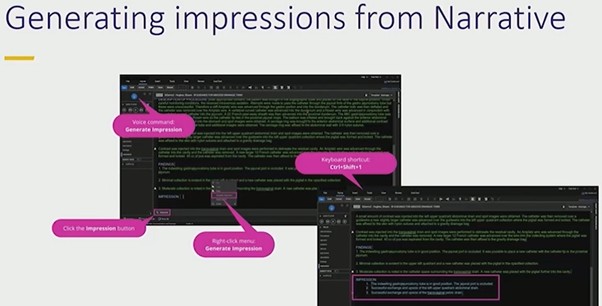
Automated impression generation from narrative text
Converting freeform dictation into structured reports
Organizing sentences under correct headings
These features accelerate reporting and reduce cognitive load without exposing PHI externally.
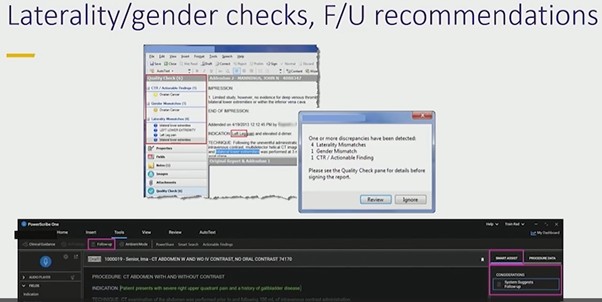
Error Prevention Still Matters
Simple NLP tools remain some of the most valuable. PowerScribe’s laterality and gender checks prevent avoidable mistakes that can undermine confidence in a report. Tools that flag mismatched anatomy—such as referencing a prostate in a female patient—provide immediate, low-friction safety nets that rads consistently appreciate.
Bottom Line
Security and workflow realities remain the biggest obstacles to adopting LLMs for radiology reporting. Until private, institution-controlled LLMs become practical and widely available, rads will continue to rely on integrated NLP tools that improve.
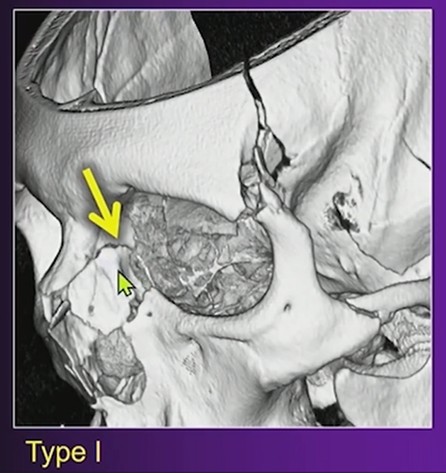
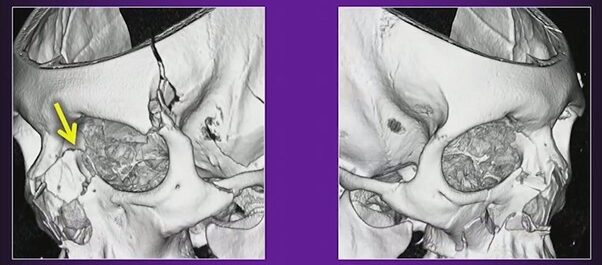
When evaluating orbital trauma, one detail rads should address is the Markowitz and Manson (M&M) classification. As Blair A. Winegar, MD, explains, this system focuses on the degree of comminution in the region of the lacrimal fossa and helps predict whether the medial canthal tendon is likely to be injured.
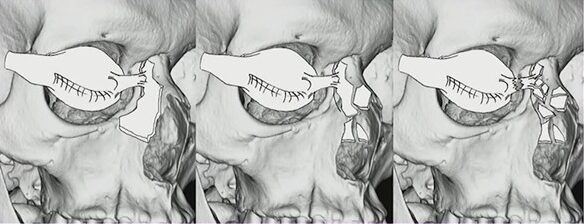
Left:Type I, Intact medial canthal tendon connected to single large fracture fragment; Center:Type II, Intact medial canthal tendon connected to single comminuted fracture fragment; Right:Type III, Disrupted medial canthal tendon with severe comminution about the lacrimal fossa
What M&M Describes
The key question is whether the lacrimal fossa remains intact or is significantly fragmented.
Intact lacrimal fossa: Low likelihood of medial canthal tendon injury.
Heavy comminution in the lacrimal fossa: Higher suspicion for medial canthal tendon disruption, which may require surgical repair.
Why Does It Matter?
The medial canthal tendon anchors at the anterior lacrimal crest. When that region is fractured extensively, the surgical team needs to prepare for possible tendon repair. Including this observation in your rad report sets appropriate expectations and guides planning for reconstruction.
Left:Type I; Right:Type II
Practical Approach
On CT, evaluate the anterior lacrimal crest and adjacent lacrimal sac fossa.
Describe whether this region is intact, minimally displaced, or extensively comminuted. Explicitly link substantial comminution to the potential for medial canthal tendon involvement.
Bottom Line
In orbital trauma, reporting the Markowitz and Manson classification provides actionable information. Identifying comminution in the lacrimal fossa helps surgeons anticipate medial canthal tendon repair and improves communication between rads and the operative team.
Retirement is one of the most unique, fulfilling, and exhilarating opportunities we will ever experience. Yes, I know, some of you may find that hard to believe. So did I, as I saw this major life transition sneaking up over the horizon and then, certainly, as I started to actually live it 10 years ago.
Why wouldn’t this be a major concern, a challenge, a mystery. We’ve been working at medicine and radiology for decades—at least since college or before (most of us finished our education/training in 22nd grade). Only a few vocations require this degree of involvement, so seeing it change or end can be a major shock. But have faith—there is more than hope down the line.
The first big question: “Is it time for me to retire?” There are many factors that determine when we decide, as they say, to put down the stethoscope (that is a piece of instrumentation used before an MRI or PET/CT is ordered). It is deeply personal, involving the interplay of fulfillment, health, finance, stress, and one’s specific life circumstances. Many ask, “What am I going to do in this vast new space?,” “What will give me a sense of purpose?,” and “Will I be able to create new personal connections?”
The good news is that, as radiologists, we are curious, self-motivated, goal-oriented, and like to learn. Whether you are simply contemplating retirement or are well into it (but need a fresh look at who you are and where you wish to be), one approach to retirement (which I prefer to call “rewirement”) is to ask a few questions, such as:
“What gives me satisfaction?”—for me; learning, teaching, being creative and productive
“What am I willing to try (new or reconnecting)?” e.g., writing, volunteering, acting classes, and improving my photography
Unlike prior generations, our next phase will be a more dynamic and fluid process as it may last a quarter of a lifetime. Therefore, self-awareness becomes extremely important in order to have a truly fulfilling and joyful experience,
Several things can make our retirement easier. The first is our “Experienced Brain.” We have learned a great deal about medicine, radiology, and life. It is a wonderful thing to pass this knowledge on to residents or medical students. I have loved voluntarily sharing what I have learned with radiology residents because it makes me stay informed and allows me to be engaged with a younger generation. You may want to teach in a totally different field, bringing to mind one physician who became a grade school teacher.
Another big advantage: If you don’t want to give up imaging entirely, there is always teleradiology, especially if you can set your own level of commitment. As this is still isolating, I would recommend balancing it with other non-medical interests, so that you keep developing and can become part of new communities.
Suffice it to say that when you are absolved of the responsibilities of work, the things you can explore and accomplish are endless. Plus, there are several other advantages that come with retirement, such as freedom from failure and freedom from comparing ourselves to others. The idea is to dive into new interests just for the sake of trying something different. If it is rewarding, keep going; if it is not, just move onto the next thing. No judgment involved. You may want to get back in touch with passions from your past or think about “What would I have done, had I had not become a physician?”
You never know where these new forays may take you. My photography ultimately led to something that gave me great satisfaction – donating my prints to hospitals to create a more welcoming and calming environment for patients, their families, and the staff who care for them. (When you are donating, competition goes out the window.)
So, time to see yourself in a different light and be open to a new, invigorating, and adventure-filled world. Enjoy the journey!
Dr. Agress retired 10 years ago, following a 36-year practice of diagnostic radiology and nuclear medicine. He continues to voluntarily teach at Columbia Presbyterian and Weill Cornell Medical Centers. You can learn more about Next Years Best Years, his resource for personal and emotional well-being, at NextYearsBestYears.com.
With therapies evolving and technology updating, radiologists the world over are ready to rise to the challenge of delivering more precise staging and follow-up for rectal cancer.
On Sunday, April 12 in Pittsburgh, PA, abdominal imaging experts from both hemispheres will convene at the David L. Lawrence Convention Center and online for Rectal MRI, the 2026 ARRS Annual Meeting Global Exchange course featuring faculty from the Royal Australian and New Zealand College of Radiologists (RANZCR).
Codirectors Aliya Qayyum (ARRS) and Kirsten Gormly (RANZCR) are bringing together the field’s finest to share evidence-based insight and technical pearls designed for immediate clinical application. For radiologists seeking to refine staging, elevate posttreatment evaluations, and stay ahead of emerging imaging biomarkers, this expertly curated course offers globally relevant guidance.
Rectal MRI: A Cornerstone of Modern Care
Once an emerging tool, rectal MRI is now the gold standard for staging, enabling assessment of the T stage and detecting key prognostic features such as mesorectal fascia involvement (MRF) and extramural venous invasion (EMVI) (Fig. 1).
Fig. 1—59-year-old patient with rectal cancer with extramesorectal vessel involvement, consistent with T category of T4b. Axial (top) and axial oblique (bottom) T2-weighted images show rectal tumor that extends through extramesorectal vein (arrow), which according to expert opinion warrants classification as T4b.
Dr. James Costello (ARRS) will lead a session on foundational principles of T staging, MRF, and EMVI, emphasizing actionable strategies to refine reports and guide multidisciplinary teams. Building upon Dr. Costello’s foundation, Dr. Verity Wood (RANZCR) addresses the myriad nuances of assessing lymph nodes and how to identify poor prognostic tumor deposits. Pointing out pitfalls left and right, her lecture during the 2026 ARRS Annual Meeting Global Exchange with RANZCR will provide the latest imaging criteria to help radiologists render more confident interpretations.
From Early Detection to Posttreatment Decision-Making
As screening programs detect more early-stage tumors, MRI also has the ability to evaluate these lesions. Dr. Gormly will discuss how to assess early cancers and why acquisition technique for high-resolution T2-weighted images directly impacts interpretive accuracy for all rectal MRI parameters (Fig. 2).
Fig. 2—Morphologic features of metastatic mesorectal nodes on MRI and potential pitfalls in assessment. 58-year-old woman with rectal adenocarcinoma. Oblique axial T2-weighted MRI (left) shows apparently spiculated node (arrow). Graininess of image is related to poor signal-tonoise ratio (SNR). Coronal T2-weighted MRI (right) shows that same node is homogeneously T2 hyperintense with dark capsule (arrow), which is typical of reactive mesorectal node. This image has superior SNR. Suboptimal images can lead to erroneous assessment of nodal morphologic features. This patient proceeded directly to surgery. Total of 38 lymph nodes (0.3–1.3 cm) were harvested. Eleven of larger lymph nodes were serially sectioned before submission for histologic processing. Final pathology revealed T3N0 disease.
Of course, staging is only part of the story. With the emergence of total neoadjuvant therapy (TNT) and “watch and wait” (W&W) protocols, radiologists play an increasingly vital role in posttreatment imaging. Dr. Raj Mohan Paspulati (ARRS) will outline W&W strategies in the United States, comparing tumor regression grading (TRG) systems and illustrating how MRI supports individualized care plans that may spare patients surgery.
The ability of MRI to predict patient outcomes can be considered more important than direct pathological correlation. Dr. Gormly will close the 2026 ARRS Annual Meeting Global Exchange course with her experiences in assessing emerging imaging biomarkers such as the “split scar sign,” aiming to improve patient selection for W&W, following a detailed explanation of how to assess residual tumor on high-resolution T2-weighted images. This is a key part of any posttreatment assessment system and is the cornerstone of the mrTRG system—the most validated MRI-based grading method globally.
Alliances Advancing Imaging
The mission of the ARRS Global Partner Society Program is to build long-standing relationships with key leaders and organizations in the worldwide imaging community—increasing awareness of our society’s services in specific nations, while raising the stature of Global Partner Societies among ARRS members. Every year, the ARRS Annual Meeting Global Exchange incorporates one partner society into the educational and social fabric of our meeting. ARRS members then reciprocate at the partner society’s meeting that same year.
Founded in 1949, RANZCR promotes and continuously improves the standards of training and practice in radiology and radiation oncology for the betterment of the people of Australia and New Zealand.
Rectal MRI not only reflects the robust collaboration between ARRS and RANZCR but also celebrates the global standardization of rectal MRI protocols.
And as Dr. Gormly told InPractice, “Australia and New Zealand’s early and ongoing partnerships with global leaders like Professor Gina Brown have positioned our region at the forefront of rectal MRI innovation. And this course is about sharing those insights with the world.”
Deborah A. Baumgarten, MD, MPH 2025-2026 ARRS President
For our next installment of serendipity here in InPractice, we’re jumping ahead pretty far in time, as you’ll note by the color photograph of Professor Torsten Almén. As a young radiologist from Malmo, Sweden (not far from Copenhagen, Denmark), he was concerned about the pain of injected iodinated contrast, especially when it was administered arterially.
The father of non-ionic iodine contrast media: oboist Torsten Almén (1931-2016)
Dr. Almen’s serendipitous contribution is that he was struck by how little his eyes stung when swimming in the relatively isotonic Baltic Sea, as compared to the more hypertonic North Sea. He then wondered if a patient’s pain had anything to do with the tonicity of the contrast material that was administered. In 1967, Almen went to Temple University in Philadelphia, PA as a postdoctorate fellow and was given the choice on working on a steerable catheter that he’d helped design or working on this notion of toxicity and tonicity of contrast. Fortunately, he chose the latter. Almen was able to show in a bat model that his theory was correct, but he had to go about designing something that could be utilized in humans—a more ideal contrast agent. He wasn’t a chemist, so he bought some textbooks, taught himself the basics of organic chemistry, and tried to get someone interested in producing this theoretical compound. He finally persuaded Nygard, which later became Nycomed, to produce his low osmolar contrast material metrizamide in 1969. It was released several years later, quickly followed by other contributions to low osmolar contrast: Isovue by Bracco in 1981, Omnipaque by GE in 1982, and Optiray by Mallinckrodt in 1989.
I dare say this gentleman is at least as recognizable as our society’s namesake, Wilhelm Conrad Roentgen. Sir Godfrey Newbold Hounsfield has had such a profound effect on our field. It was during an outing in the country when the idea came that he could determine what was inside a box by taking x-rays from all angles around the object, then somehow combine the different shadows the x-rays would produce to form an image of that object.
Sir Godfrey Newbold Hounsfield (1919-2004)
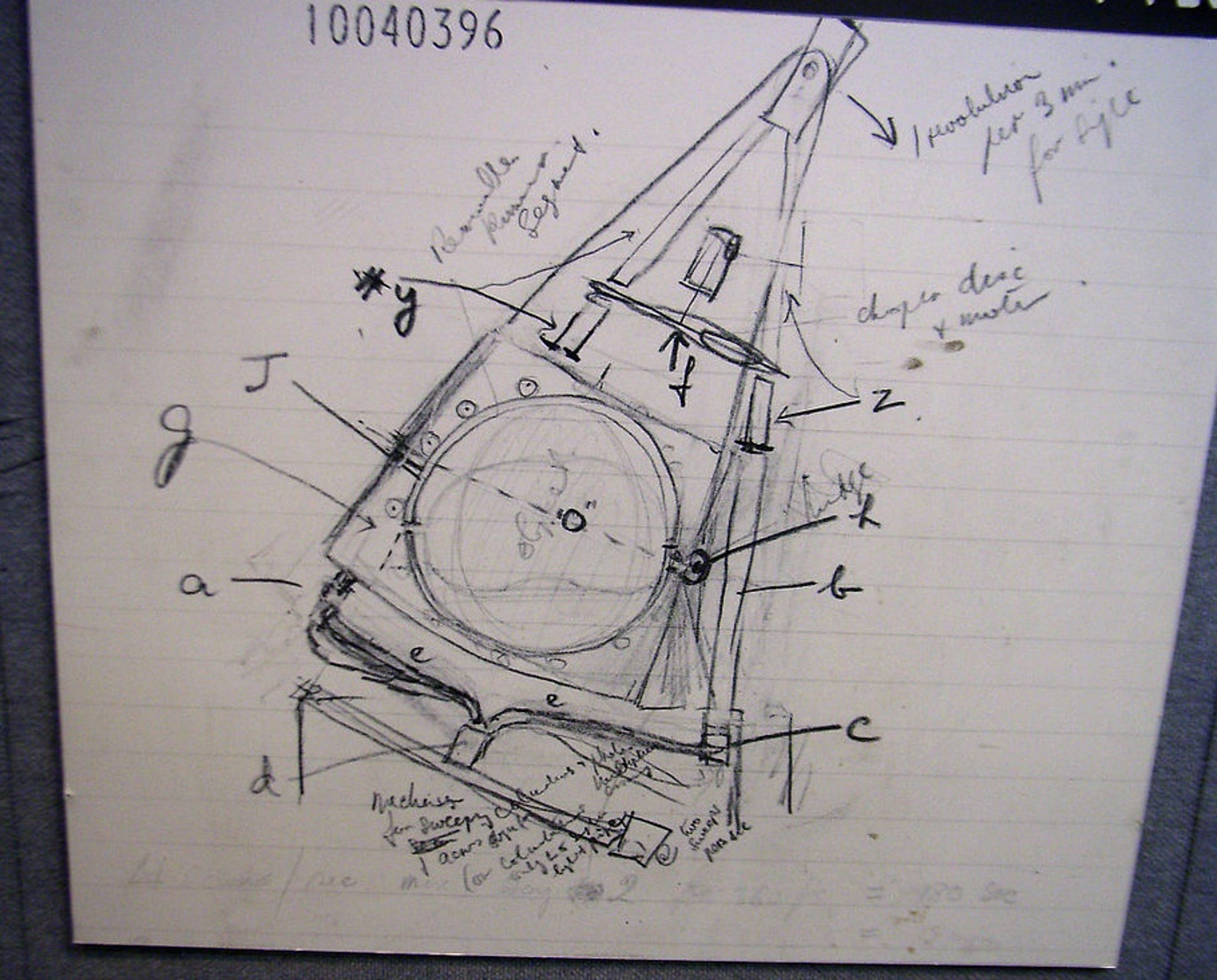
This is a sketch of his first idea of the CT scanner and the prototype. It’s one thing to formulate the idea of using x-ray readings, of course. But it was Dr. Hounsfield’s open mind that allowed him to realize not only the potential, but the necessity of using computers to analyze the data generated by taking all of the x-ray angles needed to create a CT image.
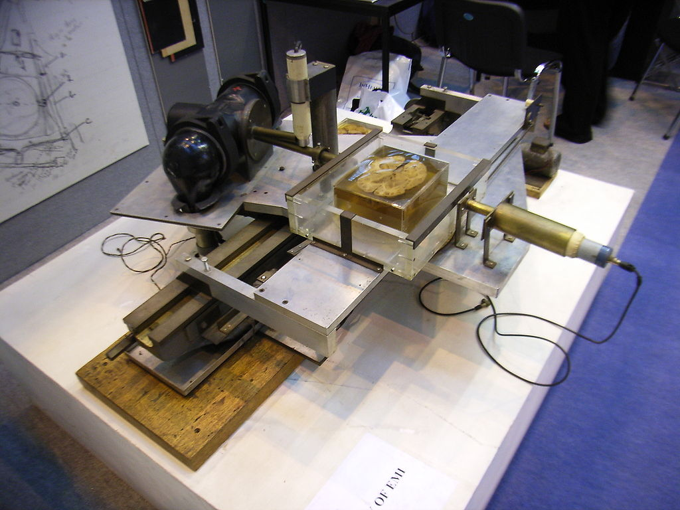
Hounsfield’s sketch of his CT scanner…
. . . compared to his prototype!
The following quotation by Dr. Louis Pasteur is particularly appropriate in this particular case: “In the field of observation, chance favors only the prepared mind.” Doctors Allan Cormack and Hounsfield shared the 1979 Nobel Prize in Physiology or Medicine for their work in CT.
Moving away from radiological discoveries for a moment, I love this quotation: “Eureka, I found what I wasn’t looking for!” This is associated with a book called Happy Accidents by a renowned abdominal radiologist named Dr. Mort Meyers, who spent his career at the State University of New York at Stony Brook. Again, emphasizing that the open mind is primed to take advantage of serendipity, how many of you know that the invention of the microwave oven had its origins when an engineer working with radar sets had a candy bar melt in his pocket, realizing it must’ve been from emitted radio waves? Or that Viagra was discovered by Pfizer when looking for a drug that increased blood flow to the heart, only to find that it increased blood flow a little lower? Or the discovery of artificial sweeteners by Constantin Fahlberg, a chemist working on coal tar derivatives, came from his inadvertent tasting of saccharine? Aspartame’s discovery came later, thanks to James Shaler, a chemist working on anti-ulcer drugs. Sure, their tasting of unfamiliar lab compounds is completely not up to today’s standards, but we can excuse them for that.
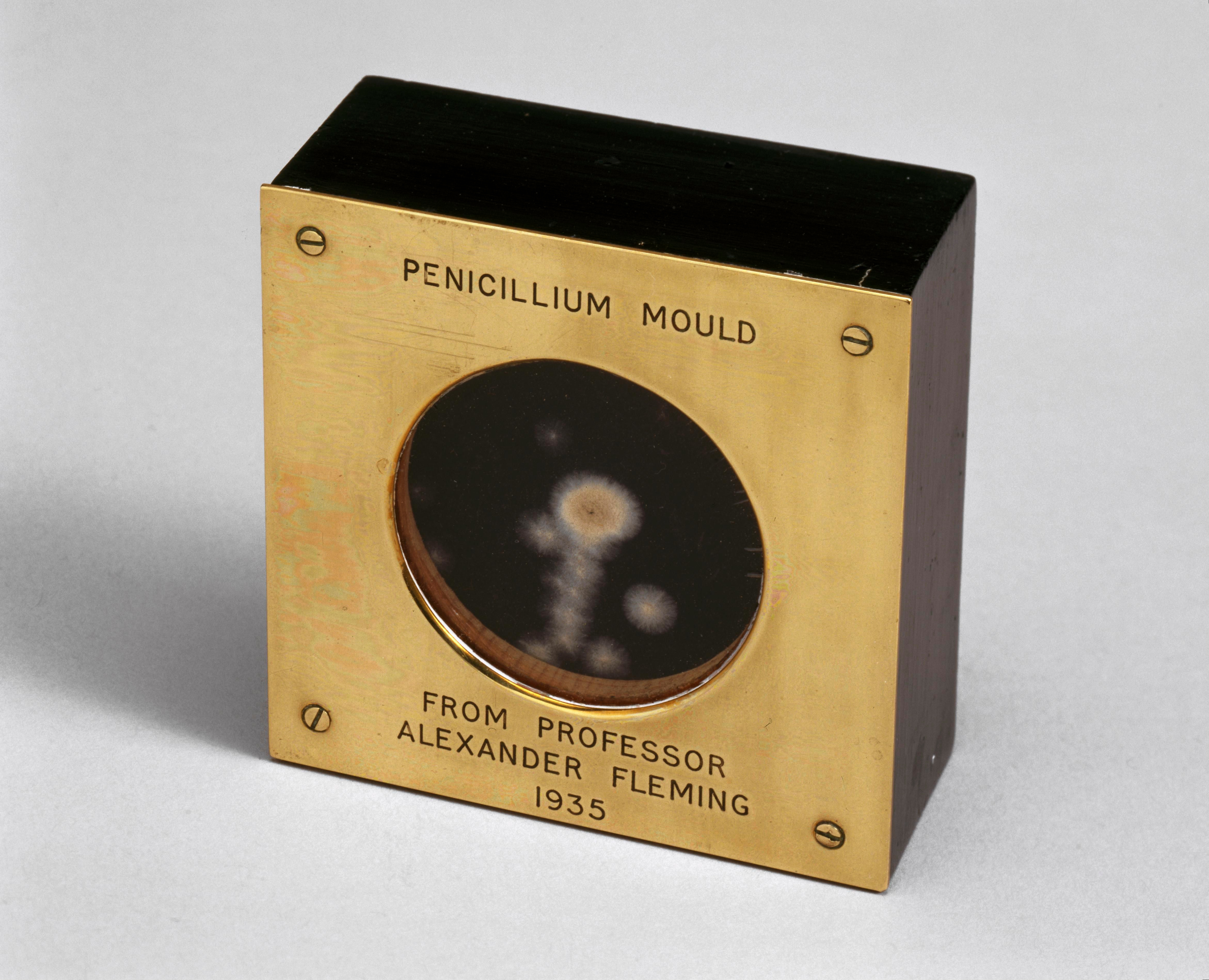
There are so many more examples of serendipity in science. Sir Alexander Fleming‘s discovery of penicillin came while working on compounds to inhibit bacterial growth, serendipitously noting one plate that had some mold on it seemed to be doing better than the other ones. Or veterinary pathologist Frank Schofield‘s discovery that spoiled sweet clover hay led to a hemorrhagic illness in cows, eventually leading to the isolation of dicoumarol, or Warfarin. Or the serendipity of the population in the United Kingdom erroneously getting a half-dose of the Oxford AstraZeneca COVID-19 vaccine before a second full dose that gave a 90% effectiveness rate against COVID-19, as compared to the 62% when two full doses were tested in Brazil and South Africa.
British biologist and pharmacologist Dr. Alexander Fleming gave this sample of penicillium notatum to a colleague at St. Mary’s Hospital, London, in 1935.
Physiologist Menko Victor “Pek” van Andel at the University of Groningen in the Netherlands studies serendipity patterns in knowledge and discovery, and he’s categorized three main types of serendipity. Positive serendipity is when a surprising fact is seen and followed by a correct interpretation (e.g., x-rays). Pseudo-serendipity is to discover something you were looking for, but in a surprising way. An example that van Andel uses is penicillin. Meanwhile, negative serendipity is when a surprising fact is seen, but not optimally investigated. And I’d like to think Dr. Donald Cameron never pursuing sodium iodine salts would be that kind of negative serendipity, although it was found positively later by Dr. Earl Osbourne (see Part I here).
Pek van Andel was one of the first researchers to extract serendipity patterns for accidental unsought knowledge discovery.
Others have built on van Andel’s work, including Darbellay et al., who published a paper titled “Interdisciplinary Research Boosted by Serendipity.” Their contention is that getting rid of the silos that house most of our disciplines and opening one’s mind to the unexpected are fundamental to the work of researchers who position themselves between and beyond disciplines. That serendipity itself is an important part of interdisciplinary research. As a creative process, serendipity is foundational in interdisciplinary collaboration, boosting the exchange of ideas to exploit the unexpected.
Examples of this interdisciplinary research aided by serendipity mentioned by Darbellay and colleagues include a team at Dow Chemical tasked with inventing a chemical compound for protecting the windscreens of airplanes. Upon application of substance 401, the researchers realized they could no longer remove the measurement device that they were utilizing on the windscreen. The team was worried because this was very costly equipment, so they called their boss, Harry Coover, who had a doctorate in chemistry. When faced with this unexpected effect of the substance 401, he realized the researchers had unknowingly and unintentionally discovered superglue, which was a substance that could bond metal and glass. Under Coover’s initiative, Dow abandoned trying to find something better for windscreens, channeled its efforts into developing superglue, and began marketing the product so many of us use today. Other accounts dispute Darbellay et al.’s retelling of this discovery, instead noting that Coover discovered superglue (cyanoacrylate) at the Eastman Kodak company, where he realized clear plastic gun sights stuck to everything. He first rejected the substance but later recognized its potential as an adhesive, so serendipitous no matter the origin!
Ironically, the near complete opposite of superglue was also a serendipitous discovery. Spencer Silver and colleague Arthur Fry stumbled upon the idea for Post-it® notes while working at 3M. Silver discovered an adhesive that sticks permanently without a permanent bond and only does so in one direction, allowing an object to be repositioned. Fry’s contribution was finding use for the adhesive while singing in his church choir and lamenting that his bookmarks kept falling out of hymnals—his own eureka moment when he remembered Silver’s invention. The original yellow? Also, an accident; it was the color of a scrap of paper in an adjoining lab.
Art Fry, 93, in Saint Paul, Minnesota
Switching gears for just a moment, how about looking at serendipity on a more personal level? I’ve always been fascinated by the role of luck in my life and in the lives of others. When I was a child, whenever anything good in my life happened, I would tell my mom “I got lucky,” to which my mom would say, “we make our own luck.” This phrase has stuck with me for a very long time, and may be my own definition of serendipity: being open to possibilities when they happen and taking advantage of them. In one sense, I could describe my ascent to becoming president of the American Roentgen Ray Society as luck. Again, lucky in the sense that I repeatedly said “yes” to volunteer opportunities, even if that opportunity wasn’t glamorous or meant a lot of work.
So, here is what I conclude about serendipity. For those of you already well involved in research, getting your feet wet in research, or wanting to become involved in research, know that chance, luck, serendipity—whatever you want to call it—will play a role in your career. Keep an open mind, expect the unexpected, then turn it on its head. Seek out ways to collaborate with people who are in unrelated fields. Take advantage of the opportunity to network and build your community at meetings such as ARRS with those outside of your chosen field or discipline and those inside your chosen field or discipline. There will be so many more serendipitous discoveries in our lifetime and many lifetimes to come. It’s what keeps our field and so many others so very interesting. I understand everybody’s time is limited and valuable, but truly consider an opportunity before saying “no.” You never know which opportunities will lead to something bigger, so keep an open mind about saying, “yes.” You never know who will be touched by your words and actions, who will change your life with a chance encounter, or whose lives will be changed by a chance encounter with you.
References:
Nyman U, Ekberg O, Aspelin P. Torsten Almén (1931-2016): the father of non-ionic iodine contrast media. Acta Radiol 2016. 57:1072–1078