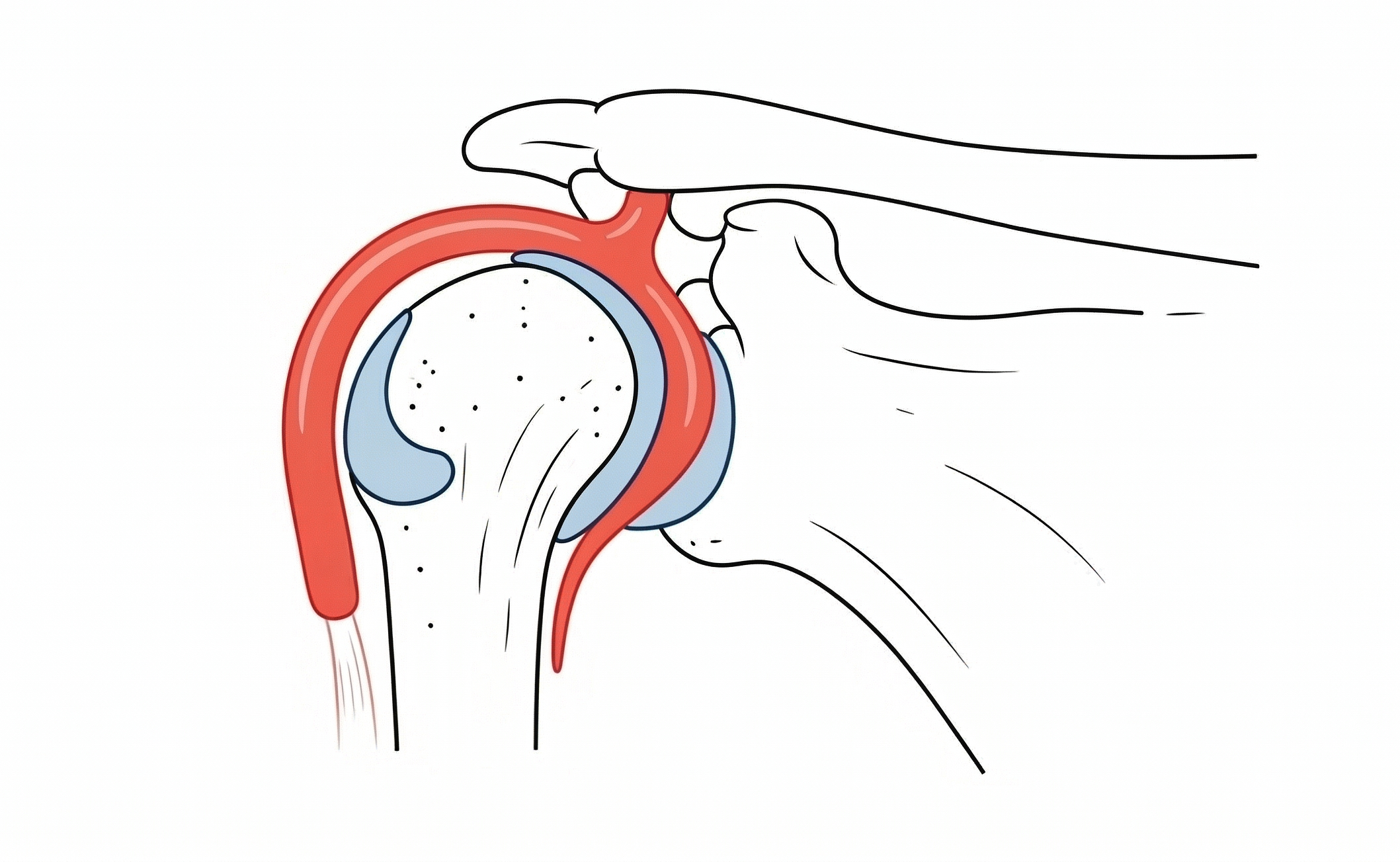
Occurring in less than 2% of your shoulder patients, apropos, there are just two things you need to ID the Buford complex. As Robert J. French, Jr., MD, enumerated for the ARRS Online Course “Expanding the Field: Imaging of Sports-Related Injuries Beyond the Knee,” this normal anatomic variation is defined by an absent anterior superior labrum and a thickened middle glenohumeral ligament (MGHL).
The Details:
- Location: Labrum is missing in the 1- to 3-o’clock position (right shoulder) or 9- to 11-o’clock (left shoulder).
- Reconstitution: Typically, labrum reappears at or below glenoid midpoint.
- MGHL: Hypertrophied, it often appears as a discrete structure—similar in size to long head of biceps tendon.
- Stability: Unlike pathologic lesions, biceps anchor and contiguous superior and anterior inferior labrum remain normal.
Closed for Repairs: Mistaking this variation for a labral avulsion is a common pitfall. In fact, in one surgical error documented in AJR, a cordlike MGHL was unfortunately attached to the glenoid as a “fix,” resulting in severely restricted shoulder motion for the patient.
The Planes:
- Axial: Look for absence of low-signal-intensity labral tissue along anterior superior glenoid rim.
- Sagittal: MGHL can be seen as a linear structure separate from the subscapularis tendon, inserting into biceps anchor.
Bottom Line: If the superior labrum and biceps anchor are intact, yet the anterior superior labrum is missing alongside a thickened MGHL, think Buford complex—not a labral tear.