Dr. Barr is a private practice neuroradiologist with Mecklenburg Radiology Associates PA in Charlotte, North Carolina, and incoming President of the American Board of Radiology.
The five years since I joined the Board of Governors has been a period of remarkable change as the American Board of Radiology (ABR) has evolved in response to new requirements and improved stakeholder engagement. The biggest change was the introduction of Online Longitudinal Assessment (OLA) in 2019 to supplant the previous model of recurring high-stakes exams as part of Continuing Certification. The platform has both formative and summative functions and, as a result, satisfies the parts of our social contract as medical professionals that relate to lifelong learning and self-assessment. It positions the ABR as one of the leaders in adopting the American Board of Medical Specialties (ABMS) Standards for Continuing Certification released last November.
In early 2020, recognizing the challenges resulting from the pandemic, we embarked on an aggressive development plan to deliver our Initial Certification exams in a virtual environment. Our early experience with OLA was crucial in guiding the design and implementation of remote exams. In 2021, we successfully administered over 5,000 exams (including both qualifying and certification exams) across all four disciplines (diagnostic radiology, interventional radiology, medical physics, and radiation oncology) and anticipate this will remain an enduring model for Initial Certification.
In addition to the introduction of remote exams and accelerated exam administration, 2021 saw the implementation of a new residency leave policy designed to balance the need for standardization with flexibility to address life events that individuals face during training. We were fortunate to benefit from the vigorous engagement of numerous stakeholders during the development of this policy, including dozens of conversations with trainees and program faculty. Beginning with the 2021–2022 academic year, residents with total time away from residency averaging less than eight weeks (40 workdays) per academic year are eligible for Initial Certification without an extension of training.
Although the programs mentioned above are the most visible to our candidates and diplomates, the behind-the-scenes efforts of our volunteers have been critical in supporting the continuous improvement of our exam content and delivery. We now offer exam candidates increased flexibility in many elements of the qualifying exams, as well as additional dates for the oral exams in medical physics, radiation oncology, and interventional radiology. Several months ago, we embarked on a comprehensive evaluation of the certification exams for diagnostic radiology; as of this writing, external discussions have provided a broad range of perspectives and extremely useful suggestions for potential modifications.
Our executive team and staff have made significant strides in streamlining our administrative processes and improving efficiency, with the goal of mitigating costs. We have reduced redundancy and non-core initiatives and terminated our lease for the Chicago testing center as part of our transition to remote exams. We’ve reduced the cost of some of our products, particularly subspecialty certification exams, and will continue to focus on fee reduction when possible. We are fortunate to maintain healthy capital reserves, which have helped offset investments in technology and software development during the past few years of transition. We continue to maintain our recognition for financial transparency with Platinum Status (per Candid®, formerly GuideStar®).
As I assume the role of ABR president, I look forward to working with our volunteers, staff, and stakeholders to support the ABR’s mission to provide a credential that indicates a high level of professional achievement and commitment to clinical excellence. The ABR Board of Governors, volunteers, and staff remain committed to improving the relevance and value of our exams and programs while avoiding increased costs and unnecessary complication for our candidates and diplomates.
Department of Radiology, Memorial Sloan Kettering Cancer Center
Lars J. Grimm
Department of Radiology, Division of Breast Imaging, Duke University School of Medicine
Jennifer A. Harvey
Department of Imaging Services, University of Rochester Medical Center
Donna M. Plecha
Department of Radiology, University Hospitals Cleveland Medical Center
Emily F. Conant
Department of Radiology, Division of Breast Imaging, Perelman School of Medicine, University of Pennsylvania
Abbreviated breast MRI (AB-MRI) has been shown to maintain the high sensitivity of longer or full breast MRI protocols while decreasing operational costs. The clinical implementation of an AB-MRI program requires collaboration of multiple stakeholders, including administrative, operational, financial, technical, and clinical providers. Institutions must define patient eligibility and imaging protocols and monitor performance metrics to ensure high-quality patient care. The improved efficiency and maintenance of accuracy of AB-MRI may allow more women to access this important supplemental screening modality.
MRI is the most sensitive imaging modality for breast cancer detection [1], and its role as an adjunct to mammographic screening for women at high risk for breast cancer (i.e., a lifetime risk > 20%) is well accepted [2–5]. Although demographic and genetically based risk assessment models are often used to determine breast cancer risk, increased mammographic density increases breast cancer risk and decreases mammographic sensitivity through the obscuration of cancer by adjacent dense breast tissue [6]. Increasing awareness of the impact of increased breast density on patient outcomes has driven the adoption of state and federal legislation mandating that women be notified of their breast density. In response to this increasing awareness, there is growing interest in supplemental screening for breast cancer with breast MRI, which shows improved breast cancer detection for women with dense breasts and otherwise average risk [7]. To accommodate the increasing demand for supplemental breast MRI screening, abbreviated (or fast) breast MRI protocols have been developed that reduce costs, improve workflow, and increase patient access. This article provides details regarding the current literature supporting the utilization of AB-MRI for supplemental screening and the numerous administrative, operational, financial, technical, and clinical elements that must be considered in the implementation of a clinical AB-MRI program.
Review of Abbreviated Breast MRI Outcome Data
The first AB-MRI study, which was published in 2014 by Kuhl et al. [8], included 443 women with a “mildly to moderately increased risk of breast cancer.” The study showed that a 3-minute AB-MRI acquisition that consists of only one unenhanced and one contrast-enhanced sequence has diagnostic accuracy in breast cancer screening that is equivalent to that of a full breast MRI protocol. Multiple studies have since been published, including a prospective multicenter trial [9] and at least three systemic reviews or meta-analyses supporting the use of AB-MRI [10–13] (Table 1).
These studies confirm that the combination of mammography and MRI screening yields the highest cancer detection rate. In addition, cancers detected with MRI are more likely to be invasive and higher grade, compared with cancers detected with mammography [14], and therefore have the potential for greater impact on patient morbidity and mortality.
Because MRI offers improved cancer detection rates and can detect more clinically relevant disease, AB-MRI has been integrated into clinical practice at numerous institutions. Clinical implementation of an AB-MRI program requires consideration of patient eligibility requirements, imaging protocols, and appropriate performance metrics to ensure high-quality patient care.
Patient Selection and Screening Interval
At present, most supplemental screening with AB-MRI is reserved for women with dense breasts, given the superior sensitivity of breast MRI for cancer detection [15]. This recommendation is supported by multiple studies of women with dense breasts, including women who underwent screening with AB-MRI after having negative or benign mammography and ultrasound findings [8], and by a prospective screening study that showed significantly higher rates of invasive breast cancer detection with AB-MRI, compared with digital breast tomosynthesis (DBT) (11.8 vs 4.8 cancers per 1,000 women) [9]. For women with an average risk of breast cancer who have dense breasts and a normal DBT, AB-MRI has shown a breast cancer detection rate of up to 27.4 cancers per 1,000 women [12]. The possible role of AB-MRI in detecting breast cancer in women with nondense breasts who are at intermediate risk for breast cancer has not yet been established.
Although there currently are no data to guide the frequency of AB-MRI screening, given current screening paradigms and the recommendation that high-risk women should undergo annual MRI screening [16], one could consider screening women of average risk who have dense breasts with AB-MRI every 1–2 years [7]. AB-MRI should be performed in addition to an annual mammography examination, and this screening may be performed at the same time as mammography or offset between mammographic screenings.
Imaging Technique
AB-MRI protocols remain institution-dependent; however, consideration should be given to minimizing the total scanning duration and thus the time that the patient spends on the table (i.e., table time). Published AB-MRI acquisition times range from 1.1 to 12 minutes [17, 18], but additional time not related to acquisition must also be allocated to allow the patient to enter and exit the room and to be positioned on the table. The AB-MRI protocol should use parameters similar to those of the full breast MRI protocol, such as magnet field strength, axis of image acquisition, and patient orientation, to facilitate interpretation and comparisons between full and AB-MRI examinations. Postprocessing of sequences, such as subtracted images, maximum-intensity-projection (MIP) images, and multiplanar reconstructions, does not increase actual scanning time and may be performed after the patient has been taken off the table, further improving table-time efficiency.
Published AB-MRI protocol sequences vary greatly but most commonly use an unenhanced T1- and/or T2-weighted sequence, plus one contrast-enhanced sequence [8–11, 19]. A single contrast-enhanced sequence enables generation of subtracted and MIP images but does not provide kinetic information. Despite AB-MRI protocol variation, a systematic review/meta-analysis showed no significant difference in the sensitivity or specificity of AB-MRI versus full breast MRI in studies with 1–2 years of follow-up [12].
Interpretation
The time needed for interpretation of AB-MRI varies depending on the number of protocol sequences [20]. AB-MRI has higher sensitivity than DBT (95% vs 39%) but lower specificity (87% vs 97%) [9]. Improving specificity through minimizing false-positive results should be prioritized when implementing an AB-MRI program.
For interpretation of AB-MRI, it is advised that one first evaluate the MIP image to assess background parenchymal enhancement (BPE) and the symmetry of the breasts and to identify any unique focal findings. AB-MRI interpretation may be more difficult when BPE is moderate or marked [21, 22]. Identification of a unique finding requiring additional evaluation should be based on the morphology of the finding and whether it differs from surrounding or BPE. If available, comparison with prior MIP images will enable determination of whether a finding is new. Correlation with findings on prior mammograms and ultrasounds may also help determine whether the unique finding is benign.
Recognizing benign patterns of BPE may help improve specificity when interpreting screening AB-MRI. Such patterns include multiple scattered foci of enhancement, symmetric regional enhancement, multiple foci with larger enhancing areas, and a picture frame distribution of enhancement along the periphery of the breast [23]. BPE may be asymmetric or, conversely, increased in patients who recently stopped taking antiestrogen medication [24].
Utilization of a T2-weighted sequence in an AB-MRI protocol can assist in the characterization of foci and masses because increased T2 signal intensity, plus a benign morphology, help support a benign diagnosis [25, 26]. T2-hyperintense masses with benign morphologic characteristics, such as round or oval shape, circumscribed margins, dark internal septations, homogeneous enhancement, or a combination of these characteristics, should at most be assessed as a BI-RADS category 3 finding. Inclusion of a T2-weighted sequence in the AB-MRI protocol can decrease BI-RADS category 3 utilization by 37.7% [8]. This is further supported by a retrospective review of T2-hyperintense masses without suspicious features, which had a malignancy rate of 2% [26]. Given that cancers may also show T2 hyperintensity, biopsy should be recommended if a T2-hyperintense finding shows suspicious morphology.
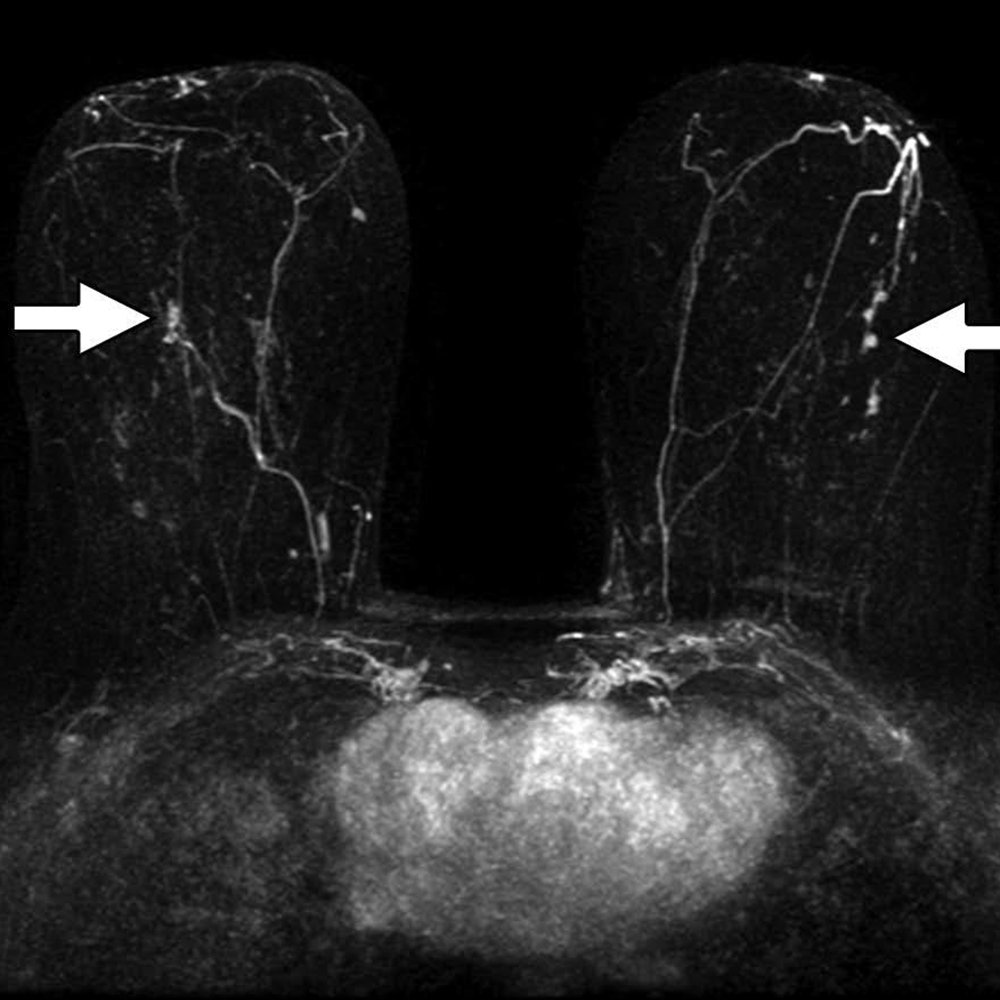
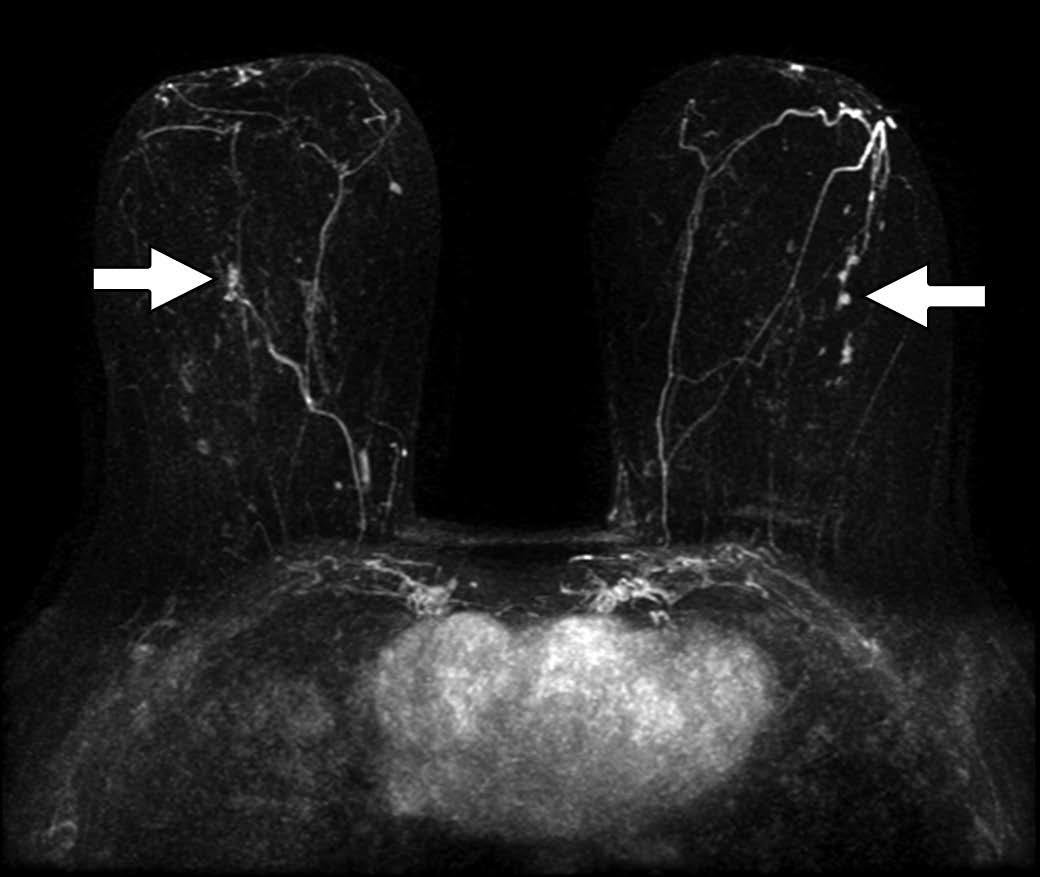
A unique nonmass enhancement (NME) should be biopsied if it is linear, segmental, clumped, heterogeneous, or has clustered ring enhancement (Fig. 1).
Fig. 1—51-year-old with bilateral high-grade ductal carcinoma in situ (DCIS). Axial contrast-enhanced subtracted maximum-intensity-projection image reveals unique, segmental, nonmass enhancement bilaterally (arrows), with pathology from MRI-guided biopsy yielding bilateral high-grade DCIS.
If NME is diffuse or regional with internal homogeneous enhancement with associated T2 fibrocystic changes, it should be considered benign.
Auditing Your Practice
As with auditing any breast MRI practice on the basis of imaging indication (i.e., high-risk screening, diagnostic problem solving, cancer staging), auditing of AB-MRI should be done separately. Performance measures should include, but should not be limited to:
cancer detection rate per 1,000 women;
PPV2 (based on recommendation for tissue diagnosis) and PPV3 (based on results of biopsies actually performed);
outcomes of BI-RADS final assessment categories 0, 3, 4, and 5;
overall sensitivity and specificity.
Complete medical audit data for screening MRI are outlined in BI-RADS 5th edition [27]; however, it is important to note that the benchmarks in BI-RADS 5th edition were based on analyses of prospective, full-protocol screening MRI trials of women with a hereditary predisposition for breast cancer.
In auditing any breast MRI program, BI-RADS category 0 should be used sparingly, reserved for requests of prior imaging that may not have been available at the time of initial interpretation. For example, it may be necessary to correlate MRI findings with those from mammography and/or ultrasound to ensure the stability of MRI findings, such as probable fibroadenomas, lymph nodes, fat necrosis, or a surgical scar. Those MRI findings with benign mammographic or sonographic correlates may be downgraded to BI-RADS category 2 (benign). Careful comparison with prior imaging ultimately helps improves the specificity of MRI and thus patient outcomes.
Although no benchmarks have yet been established for short-term follow-up or the use of BI-RADS category 3 for breast MRI, early outcome data suggest that the limited imaging provided by AB-MRI may increase the rate of short-term follow-up recommendations, compared with full breast MRI protocols [28]. In reporting their first 2 years of experience with AB-MRI, Marshall et al. [28] found that in the first 4 months, their BI-RADS category 3 rate was 14.2%. In an effort to decrease the BI-RADS category 3 rate, they required that all BI-RADS category 3 cases be reviewed by at least two other breast radiologists and that their group would review such cases weekly. After the interventions, the group’s use of BI-RADS category 3 decreased to 8.3% in their first year [28]. As with any breast MRI study, when BI-RADS category 3 is assigned, the next recommendations should clearly be stated in the report.
For cases where an MRI-directed ultrasound is recommended for further evaluation of a mass, the MRI report should provide recommendations for next steps, if a follow-up ultrasound shows no finding. If MRI-directed ultrasound shows a probably benign mass, follow-up of the mass can be performed with ultrasound in 6 months, instead of with MRI. In addition, if follow-up with MRI is recommended, it should be an AB-MRI, not a full-protocol examination, to maintain operational costs and facilitate comparison across similar protocols. A final assessment of BI-RADS category 3 should never be used for an enlarging or new solid mass. Benchmarks are well established for outcomes for BI-RADS categories 4 and 5, as well as for PPV2 and PPV3 [29]. Access to the audit data of each individual reader, as well as to the combined data of the group, is essential, so radiologists can compare their outcomes to those of others and seek additional training as needed.
As expected, there is a learning curve to the interpretation of any new imaging modality or protocol. Auditing allows the identification of outliers among a group of radiologists and may help target individuals for additional training. As with any new imaging modality, a practice may also consider limiting the number of radiologists reading AB-MRI cases early in the implementation, later expanding the number of readers as the volume of examinations increases and a teaching set of images with known outcomes has been collected for sharing across the group. Furthermore, as outcome data from AB-MR studies continue to evolve, benchmarks will be established for best practices.
Financial Considerations
Because there currently is no Current Procedural Terminology (CPT) code for AB-MRI, women must self-pay for their examinations without insurance being billed [15]. According to recent reviews of AB-MRI implementation at sites across the United States, out-of-pocket charges vary from $250 [28] to $500 [30]. When appropriate pricing is considered, the cost of the gadolinium-based contrast agent and table time must be considered [31], as must the costs of any downstream MRI-guided biopsies that may or may not be covered by the patient’s insurance. It should be noted that the out-of-pocket payment may be a barrier for some patients, leading to disparities in access to AB-MRI screening. In a recent survey of 508 patients with dense breasts who were undergoing screening mammography, 67% of patients cited the cost of adjunct screening as the primary deterrent [32], which was independently associated with younger age [33]. A possible solution could include adjustment of the self-payment costs based on financial need.
To determine appropriate pricing based on cost benefit, Mango et al. [34] used a Monte Carlo simulation to analyze a 30-year screening period in which a hypothetical group of 2.5 million women would undergo either digital mammography annually or MRI every 3 years (selected on the basis of no interval cancers being identified during this time frame in another study [35]). At 24 years, MRI became as cost-effective as mammography ($13.02 billion vs $13.03 billion, respectively). When a lower cost of $400 was used for MRI (vs $640 for the full diagnostic protocol), MRI screening became more cost-effective in less than 6 years ($3.41 billion vs $3.65 billion for mammography). However, the comparison of AB-MRI with 2D mammography rather than DBT limits generalizability [34].
Bundled payment models, which include all costs from screening to breast cancer diagnosis over a 364-day period, have been created to control costs and increase value. If AB-MRI reduces overall costs for breast cancer screening (as a triennial examination performed without mammography), compared with digital mammography by 6 years, as suggested by the Monte Carlo simulation [34], bundled payments may be reasonable for incident AB-MRI screening at the cost of $400 per study. The societal costs of screening once every 3 years must also be considered.
With no current insurance coverage for AB-MRI, institutions must engage multiple stakeholders when initiating an AB-MRI program. Certainly, the downstream revenues to the institution from breast cancers detected using AB-MRI are an important consideration. Institutional financial support may be needed, with expectations of downstream revenues.
Implementation of Abbreviated (or Fast) MRI in Your Clinical Practice
A clear protocol that defines which patients should be offered AB-MRI is needed, especially in the early phase of implementation. Additionally, because triage of patients will be needed to ensure appropriateness, it may be prudent to limit the number of schedulers involved in booking AB-MRI examinations, until a smooth process is developed. A telephone script for schedulers can help to ensure that appropriate eligibility is determined before scheduling [7].
Preferably, AB-MRI examinations should be scheduled in time slots that are significantly shorter than the time slots needed for full-protocol breast MRI, which takes longer to perform. To increase operational efficiency for an abbreviated protocol, it will be important to work with MRI technologists to limit the time that patients are positioned on the table to match the abbreviated protocol. For example, it will be important to emphasize that for the greatest efficiency, the processing of reconstructed images (subtracted and MIP images) by technologists should be done after the patient has been removed from the MRI table and imaging room. AB-MRI examinations can also be scheduled sequentially to reduce the time needed to set up and take down the breast coil. This attention to efficient use of the room and table time will optimize operations and allow more rapid turnover of the room for the next patient study, resulting in less downtime for room use [31].
To start a successful program of supplemental AB-MRI screening, it is essential to engage referring health care providers with educational programs that address who may be appropriate for supplemental AB-MRI screening and what the implications of additional screening may be for patients. One of the best methods of educating both patients and providers is lecturing at patient-facing symposia or departmental grand rounds to discuss the implications of increased breast density on both the masking of cancers on mammography and the risk of breast cancer developing. Also, it is helpful to create informational cards on supplemental screening with AB-MRI that can be provided to appropriate patients in either the breast imaging or primary care clinics [7]. As uptake of the new protocol increases and significant results, such as supplemental cancer detection rates and subtypes of cancers detected, become available, follow-up educational sessions should be provided to referring providers and, if possible, consumers.
Future Directions
The imaging sequences for breast MRI protocols, including AB-MRI protocols, are constantly evolving. For example, given the limited temporal information regarding many AB-MRI protocols, several exploratory efforts have included ultrafast sequences [36–39], which may have lower spatial resolution but may include images acquired every 1–10 seconds during the first two minutes after injection of contrast medium. Therefore, while maintaining an abbreviated protocol, measurements of both maximum slope of enhancement and rate of enhancement are possible to help discriminate benign from malignant lesions [39, 40]. There have also been efforts to develop unenhanced abbreviated breast MRI protocols because screening MRI could potentially be performed routinely over many years and because there have been concerns surrounding cumulative deposition of gadolinium [41]. A recent study by Bickelhaupt et al. [42] showed that the performance of unenhanced DWI and AB-MRI was comparable (sensitivity, 0.92 vs 0.85, respectively; specificity, 0.94 vs 0.90, respectively). Although acquisition of DWI is time-consuming, the possibility of DWI replacing contrast imaging is appealing, if performance is maintained [42]. However, according to a recent study that included both DWI and contrast imaging, inclusion of DWI in the abbreviated protocol achieved performance comparable to that of a full protocol (sensitivity, 100% vs 100%, respectively; specificity, 95.0% vs 96.8%, respectively); however, scanning time was extended, and contrast medium was still used [43]. Ideally, DWI will advance so that performance of an abbreviated DWI protocol will rival that of an abbreviated contrast study.
AB-MRI may improve access to high-sensitivity screening breast MRI and decrease overall cost. Successful clinical implementation requires the thoughtful collaboration of multiple stakeholders and ongoing monitoring of performance metrics. Additional data and experience are required to facilitate standardization across institutions. With improved efficiency and maintained accuracy, AB-MRI may enable more women to access this important supplemental screening modality.
A multimodality review—everything from routine ultrasound and mammography to the latest DBT and AI applications—ARRS’ Breast Tumor Imaging Online Course delivers the interpretive, technical, and systems knowledge that practicing radiologists need to provide quality breast cancer screening. Additional lectures address pathology, the BI-RADS lexicon, and even the history and economics of breast cancer, all critical for improving overall care disparities and patient outcomes.
DeMartini W, Lehman C. A review of current evidence-based clinical applications for breast magnetic resonance imaging. Top Magn Reson Imaging 2008; 19:143–150
Sardanelli F, Boetes C, Borisch B, et al. Magnetic resonance imaging of the breast: recommendations from the EUSOMA working group. Eur J Cancer 2010; 46:1296–1316
Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007; 57:75–89
Lee CH, Dershaw DD, Kopans D, et al. Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultra- sound, and other technologies for the detection of clinically occult breast cancer. J Am Coll Radiol 2010; 7:18–27
Mann RM, Balleyguier C, Baltzer PA, et al. Breast MRI: EUSOBI recommendations for women’s information. Eur Radiol 2015; 25:3669–3678
Saftlas AF, Hoover RN, Brinton LA, et al. Mammographic densities and risk of breast cancer. Cancer 1991; 67:2833–2838
Grimm LJ, Mango VL, Harvey JA, Plecha DM, Conant EF. Implementation of abbreviated breast MRI for screening: AJR expert panel narrative review. AJR 2021 Aug 11 [published online]
Kuhl CK, Schrading S, Strobel K, Schild HH, Hilgers RD, Bieling HB. Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection—a novel approach to breast cancer screening with MRI. J Clin Oncol 2014; 32:2304–2310
Comstock CE, Gatsonis C, Newstead GM, et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening. JAMA 2020; 323:746–756
Baxter GC, Selamoglu A, Mackay JW, Bond S, Gray E, Gilbert FJ. A meta-analysis comparing the diagnostic performance of abbreviated MRI and a full diagnostic protocol in breast cancer. Clin Radiol 2021; 76:154
Hernández ML, Osorio S, Florez K, Ospino A, Diaz GM. Abbreviated magnetic resonance imaging in breast cancer: a systematic review of literature. Eur J Radiol Open 2020; 8:100307
Geach R, Jones LI, Harding SA, et al. The potential utility of abbreviated breast MRI (FAST MRI) as a tool for breast cancer screening: a systematic review and meta-analysis. Clin Radiol 2021; 76:154.e11–154.e22
Weinstein SP, Korhonen K, Cirelli C, et al. Abbreviated breast magnetic resonance imaging for supplemental screening of women with dense breasts and average risk. J Clin Oncol 2020; 38:3874–3882
Sung JS, Stamler S, Brooks J, et al. Breast cancers detected at screening MR imaging and mammography in patients at high risk: method of detection reflects tumor histopathologic results. Radiology 2016; 280:716–722
Marshall H, Pham R, Sieck L, Plecha D. Implementing abbreviated MRI screening into a breast imaging practice. AJR 2019; 213:234–237
Monticciolo DL, Newell MS, Moy L, Niell B, Monsees B, Sickles EA. Breast cancer screening in women at higher-than-average risk: recommendations from the ACR. J Am Coll Radiol 2018; 15:408–414
Mori N, Sheth D, Abe H. Nonmass enhancement breast lesions: diagnostic performance of kinetic assessment on ultrafast and standard dynamic contrast-enhanced MRI in comparison with morphologic evaluation. AJR 2020; 215:511–518
Heacock L, Melsaether AN, Heller SL, et al. Evaluation of a known breast cancer using an abbreviated breast MRI protocol: correlation of imaging characteristics and pathology with lesion detection and conspicuity. Eur J Radiol 2016; 85:815–823
Heacock L, Lewin AA, Toth HK, Moy L, Reig B. Abbreviated MR imaging for breast cancer. Radiol Clin North Am 2021; 59:99–111
Harvey SC, Di Carlo PA, Lee B, Obadina E, Sippo D, Mullen L. An abbreviated protocol for high-risk screening breast MRI saves time and resources. J Am Coll Radiol 2016; 13:R74–R80
DeMartini WB, Liu F, Peacock S, Eby PR, Gutierrez RL, Lehman CD. Background parenchymal enhancement on breast MRI: impact on diagnostic performance. AJR 2012; 198:[web]W373–W380
Ray KM, Kerlikowske K, Lobach IV, et al. Effect of background parenchymal enhancement on breast MR imaging interpretive performance in community-based practices. Radiology 2018; 286:822–829
Giess CS, Yeh ED, Raza S, Birdwell RL. Background parenchymal enhancement at breast MR imaging: normal patterns, diagnostic challenges, and potential for false-positive and false-negative interpretation. RadioGraphics 2014; 34:234–247
Li J, Dershaw DD, Lee CH, Joo S, Morris EA. Breast MRI after conservation therapy: usual findings in routine follow-up examinations. AJR 2010; 195:799–807 [Erratum in AJR 2010; 195:1043]
Ha R, Sung J, Lee C, Comstock C, Wynn R, Morris E. Characteristics and outcome of enhancing foci followed on breast MRI with management implications. Clin Radiol 2014; 69:715–720
Grimm LJ, Enslow M, Ghate SV. Solitary, well-circumscribed, T2 hyperintense masses on MRI have very low malignancy rates. J Breast Imaging 2019; 1:37–42
Ikeda DM, Hylton NM, Kuhl CK, et al. BI-RADS: magnetic resonance imaging, 1st ed. In: D’Orsi CJ, Mendelson EB, Ikeda DM, et al. Breast Imaging Reporting and Data System: ACR BI-RADS—breast imaging atlas. Reston, VA: American College of Radiology, 2003
Marshall HN, Plecha DM. Setting up an abbreviated breast MRI program: our two-year implementation experience. J Breast Imaging 2020; 2:603–608
Lee JM, Ichikawa L, Valencia E, et al. Performance benchmarks for screening breast MR imaging in community practice. Radiology 2017; 285:44–52
Berg WA, Rafferty EA, Friedewald SM, Hruska CB, Rahbar H. Screening algorithms in dense breasts: AJR expert panel narrative review. AJR 2021; 216:275–294
Borthakur A, Weinstein SP, Schnall MD, Conant EF. Comparison of study activity times for “full” versus “fast MRI” for breast cancer screening. J Am Coll Radiol 2019; 16:1046–1051
Miller MM, Repich K, Patrie JT, Anderson RT, Harvey JA. Preferences and attitudes regarding adjunct breast cancer screening among patients with dense breasts. J Breast Imaging 2021; 2:119–124
Miller MM, Repich K, Patrie JT, Anderson RT, Har- vey JA. Patient characteristics associated with patient-reported deterrents to adjunct breast cancer screening among patients with dense breasts. AJR 2021;217: 1069–1079
Mango VL, Goel A, Mema E, Kwak E, Ha R. Breast MRI screening for average-risk women: a Monte Carlo simulation cost-benefit analysis. J Magn Reson Imaging 2019; 49:e216–e221
Kuhl CK, Strobel K, Bieling H, Leutner C, Schild HH, Schrading S. Supplemental breast MR imaging screening of women with average risk of breast cancer. Radiology 2017; 283:361–370
van Zelst JCM, Vreemann S, Witt HJ, et al. Multireader study on the diagnostic accuracy of ultra- fast breast magnetic resonance imaging for breast cancer screening. Invest Radiol 2018; 53:579–586
Goto M, Sakai K, Yokota H, et al. Diagnostic performance of initial enhancement analysis using ultra- fast dynamic contrast-enhanced MRI for breast lesions. Eur Radiol 2019; 29:1164–1174
Milon A, Vande Perre S, Poujol J, et al. Abbreviated breast MRI combining FAST protocol and high temporal resolution (HTR) dynamic contrast enhanced (DCE) sequence. Eur J Radiol 2019; 117:199–208
Mann RM, Mus RD, van Zelst J, Geppert C, Karssemeijer N, Platel B. A novel approach to contrast- enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest Radiol 2014; 49:579–585
Abe H, Mori N, Tsuchiya K, et al. Kinetic analysis of benign and malignant breast lesions with ultrafast dynamic contrast-enhanced MRI: comparison with standard kinetic assessment. AJR 2016; 207:1159– 1166
Runge VM. Critical questions regarding gadolinium deposition in the brain and body after injections of the gadolinium-based contrast agents, safety, and clinical recommendations in consideration of the EMA’s Pharmacovigilance and Risk Assessment Committee recommendation for suspension of the marketing authorizations for 4 linear agents. Invest Radiol 2017; 52:317–323
Bickelhaupt S, Laun FB, Tesdorff J, et al. Fast and noninvasive characterization of suspicious lesions detected at breast cancer x-ray screening: capability of diffusion-weighted MR imaging with MIPs. Radiology 2016; 278:689–697
Chen SQ, Huang M, Shen YY, Liu CL, Xu CX. Abbreviated MRI protocols for detecting breast cancer in women with dense breasts. Korean J Radiol 2017; 18:470–475
Department of Radiology, Division of Musculoskeletal Imaging and Intervention Massachusetts General Hospital and Harvard Medical School
The chest wall includes a variety of osseous, cartilaginous, and musculotendinous structures that are vulnerable to athletic injuries. Lesions involving these structures usually can be divided in two main categories:
lesions caused by trauma in which an external force causes direct or indirect injury to bones, cartilage, or soft tissue, leading to fractures, dislocations, and soft-tissue contusions;
lesions caused by mechanical overload from powerful muscle contraction, with or without adequate balance provided by muscle antagonists, leading to myotendinous and muscular lesions and repetitive bone stress changes.
A variety of contact and noncontact sporting activities may have mechanisms that predispose athletes to chest wall injuries. This article summarizes important aspects of athletic chest wall lesions, keeping in mind that many such lesions can occur in nonathletic endeavors, given the similarity of injury mechanisms. General technical aspects for imaging musculoskeletal athletic chest wall injuries are discussed, with most of the focus on CT and MRI, followed by discussions of injuries to the ribs, costochondral cartilage, sternoclavicular joint, and manubriosternal joint. In addition, athletic injuries to select muscles, such as the latissimus dorsi and teres major, are discussed in the context of athletic activities involving throwing.
Technical Considerations
Adequate imaging of chest wall injuries presents technical challenges that are specific to the scanning modality (CT vs MRI) and the targeted structure (rib or costochondral vs soft-tissue lesions). For both CT and MRI, a general recommendation is to perform at least one acquisition with bilateral FOV coverage for comparison purposes. A helpful procedure is to place MRI- or CT-visible skin markers in the area of pain or bracket a zone of discomfort. This allows the radiologist to better focus on specific structures that may be injured but are not clinically or functionally obvious at presentation. Another recommendation regarding MRI includes attempting to minimize respiratory motion by having the patient lie on the affected area (e.g., prone position, if lesion is anterior), which has the combined effect of reducing motion and keeping the structure in contact with the imaging coil. This is, of course, limited by patient comfort, so such decisions may require discretion from the technologist and attending radiologist on a case-by-case basis.
Imaging of bone and costochondral injuries with MRI can be challenging because of the curved anatomy of the chest wall and ribs, which may limit proper visualization of small fractures if nonangled sagittal and coronal planes are used. Obtaining oblique sagittal and/or coronal MR images that are tangential to the abnormality allows identification of the lesion with adequate visualization of the adjacent rib structure and/or costochondral cartilage. Fat suppression is also difficult during chest wall MRI because achieving magnetic field homogeneity often requires the use of more robust techniques, such as STIR pulse sequences. Further, breathing motion and pulsation artifacts may cause image quality degradation, reducing imaging and diagnostic accuracy. The use of fast MRI techniques, such as T2 HASTE, PROPELLER (GE Healthcare), BLADE (Siemens Healthineers), and breath-hold pulse sequences, is desirable, as these approaches mitigate the effect of motion artifacts. On CT, bilateral FOV coverage to compare an affected area with similar contralateral anatomy and the use of thin-slice high-resolution images with bone kernel reconstructions are also recommended. CT allows rapid multiplanar and flexible reconstructions that may be useful when evaluating rib and costochondral fractures, as well as sternoclavicular and manubriosternal joint alignment. Finally, 3D reconstructions are easily obtained from CT images and may prove useful for surgical planning of sternoclavicular joint injuries.
Chest wall muscular injuries are best imaged with MRI, including T1-weighted and T2-weighted fat-suppressed pulse sequences. In the author’s experience, the axial plane is the most important because it provides the best visualization of the pectoralis major, latissimus dorsi, and teres major tendon attachments. Oblique coronal images along the muscle planes can be obtained, though they may provide limited utility for surgical decisions and may be difficult to standardize across multiple sites in an institution. As described for osseous and cartilaginous lesions, the use of fast MRI techniques can help produce images that are less degraded by motion artifact. Bilateral FOV MRI may compromise spatial resolution and should therefore be limited to one to two acquisitions that allow comparison with the unaffected contralateral side.
Sternoclavicular joint injuries are best imaged with CT, especially if clinical signs indicate a posterior dislocation. CT is a prompt imaging method that not only shows the degree of joint malalignment but also evaluates the integrity of upper mediastinum and adjacent great vessels. Manubriosternal joint injuries can be adequately assessed by both MRI and CT, with coronal and sagittal planes being the most adequate to examine for fractures or malalignment.
Ultrasound may prove useful in certain situations. For example, because of the superficial nature of rib and costal cartilage, sonographic detection of fractures is possible and may represent a prompt method to evaluate focal complaints in patients [1]. In this context, the sonographer is able to place the ultrasound probe (preferably using frequencies ≥ 7 MHz) very precisely over the affected area to evaluate for focal osseous or cartilaginous discontinuities. In situations where muscle injuries are suspected, ultrasound is also a reliable imaging method [2]. However, in the author’s experience, it is common for patients with such injuries to present well-developed musculature (e.g., bodybuilders, football players), which may pose a limiting factor for adequate visualization of deep structures, such as tendon attachments. Complementary MRI is required in these cases, with ultrasound serving as a triage tool to be used at the discretion of the medical team. Finally, ultrasound is limited in its capability of assessing malalignments or dislocations of joints, such as the sternoclavicular and manubriosternal joints.
Rib Stress Fractures
Given that ribs are nonweightbearing bones, two main mechanisms can cause rib fractures:
direct impact from an external source, commonly occurring in football, martial arts, and other contact or extreme sports;
stress fractures due to muscular contraction.
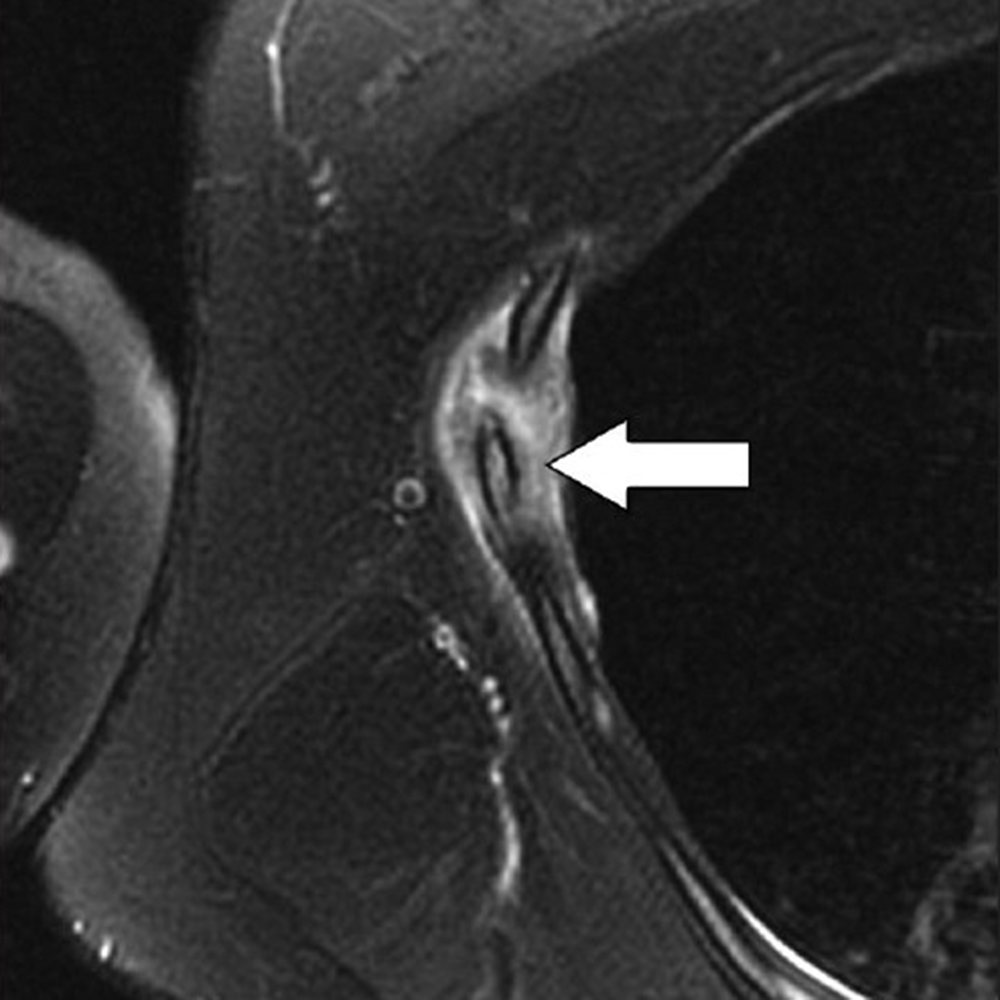
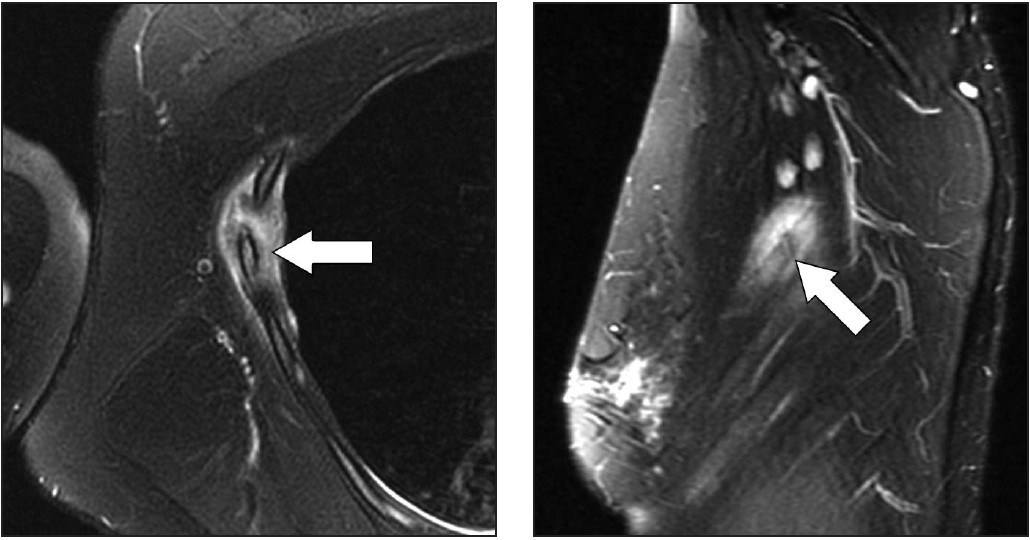
The latter mechanism most often results from strong muscular contraction that is unopposed by a counteracting fatigued muscle. In the case of rib stress fractures, the serratus anterior muscle plays a critical role [3, 4]. The serratus anterior muscle arises from the medial or ventral aspect of the scapula, with multiple slips extending anteriorly that attach to the first through tenth ribs at their middle third. The main role of the serratus anterior muscle is to protract the scapula. Importantly, this action is opposed by the scapular retractors (rhomboid muscles), which stabilize the scapula. In this situation, the serratus anterior muscle will promote an increase in the lateral diameter of the chest cavity. This mechanism can lead to abnormal stress at the middle third of the ribs in sports that involve repetitive contraction of the serratus anterior muscle, such as in elite rowing and swimming. In rowing, stress fractures are relatively common and may affect up to 12% of rowers. The peak contraction of the serratus anterior muscle occurs at the initial phase of the rowing cycle (known as “the catch”), in which the rowing oars are pulled away from the body, causing strong stabilization of the scapula by the rhomboid muscles and serratus anterior muscle. Performed repetitively, this action creates a compressive force vector directed toward the middle thirds of the ribs that can lead to stress fractures, most often affecting the fourth through eighth ribs in up to 86% of cases. If this compression is unopposed by a fatigued serratus anterior muscle, a repetitive stress injury may occur [3, 4]. Stress fractures also affect novice golfers who are still developing their technique and often strike the ground during swing strokes. Frequent ground impact force due to repetitive inaccurate strokes is thought to be transmitted to the chest wall on the leading side, causing stress fractures [5]. Additional sports in which rib stress fractures have been described include baseball, lacrosse, weightlifting, ballet, and gymnastics. MRI findings of rib stress fractures are similar to those seen in the extremities, including a well-defined linear area of low signal intensity surrounded by marrow edema, with the best contrast noted in T2- weighted fat-suppressed images (Fig. 1).
Fig. 1—23-year-old collegiate-level rower with history of midaxillary pain. Left, Axial T2-weighted fat-suppressed MR image shows edema in bone marrow and soft tissues surrounding nondisplaced fracture (arrow) of right fourth rib. Right, Tangential oblique sagittal T2-weighted fast-suppressed MR image shows best view of fracture (arrow).
Edema in the surrounding intercostal muscles and extrapleural space is often noted [6]. As mentioned earlier, such fractures may be better depicted on oblique sagittal or coronal images that are tangential to the fracture and provide context, better showing rib portions adjacent to the fracture itself. Healing of rib stress fractures can be monitored by MRI, showing progressive improvement of marrow edema and bony bridging; however, clinical symptoms may persist even though the fracture appears healed on imaging.
Stress fractures affecting the first rib result from a different proposed mechanism that is a function of the rib’s anatomic features. The serratus anterior muscle attaches to the first rib’s lateral edge at its middle third, whereas the anterior and middle scalene muscles attach to the medial edge at the same level. The anterior scalene muscle attaches at a well-defined bony protuberance, behind which is a biomechanically weak zone of the first rib. This area, through which the subclavian vessels and brachial plexus travel, has been dubbed the “Achilles heel” of the first rib [7]. First rib fractures occur more commonly in throwing athletes, such as baseball players. Throughout the throwing cycle, the most prominent eccentric muscular contraction of the serratus anterior muscle occurs at the arm cocking stage, during which the scapula moves posteriorly, leading to strong opposition by the serratus anterior muscle. This motion, performed repetitively in high-performance athletes, can place undue mechanical stress on the weak zone of the first rib, leading to stress fractures. Such fractures can be treated conservatively but may take a long time to heal (6–12 months) and, if nonunion occurs with a large bone callus, may lead to symptoms of thoracic outlet syndrome. Additional activities for which first rib fractures have been described include jive dancing, basketball, tennis, and weightlifting. First rib fractures can be depicted adequately on MRI, though most studies on such fractures have used CT and occasionally nuclear medicine bone scans [7].
Costal Cartilage Injury
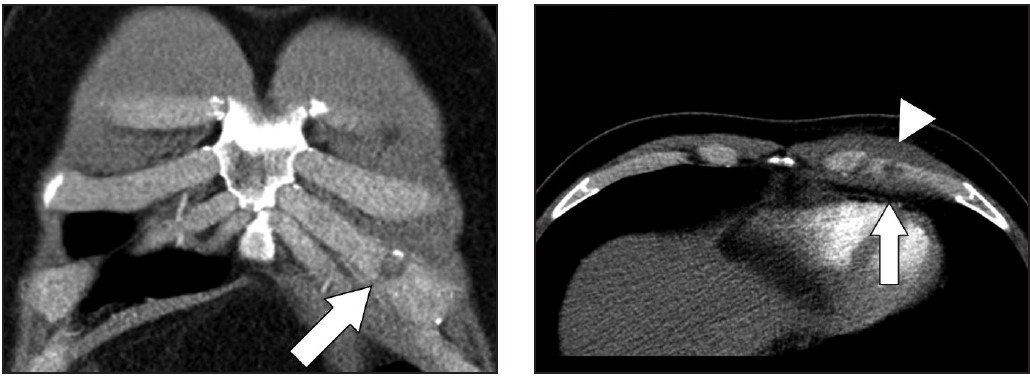
Areas that may be affected by costal cartilage injury include the sternochondral junction, midsubstance of the costal cartilage, and costochondral junction. Most commonly, such injuries affect the relatively immobile upper rib cage (first to third costal cartilages) and are due to rotation injury and/or excessive axial loading (such as in weightlifting). Lesions affecting the lower rib cage (fourth through eighth costal cartilages) typically result from direct impacts, such as seen in contact sports (hockey, football, rugby, and martial arts) [8]. An important anatomic feature of costal cartilage is the presence of a central cavity that is best seen on CT images as a zone of lower attenuation tracking along the structure [9]. A predominance of blood vessels, loose connective tissue, macrophages, and fat exist within this area. Although this zone resembles a bone marrow cavity, no marrow cells or lineage is present. Anatomic studies suggest this central channel in costal cartilage is more akin to nutrient channels because of the dominant feature of high vascularity. The presence of a dense vascular network in this portion of costal cartilage predisposes to significant bleeding in the event of fractures. A common feature in costal cartilage fractures is the presence of an associated hematoma of the chest wall, which can lead to clinician suspicion of neoplastic masses. Scrutiny of the area using thin-slice CT may reveal a linear discontinuity of the costal cartilage adjacent to the suspected mass, increasing the likelihood of a trauma-related cause. Patient history may help direct the radiologist, as a traumatic event related to lifting or direct impact may have occurred, possibly resulting in subsequent pain and a local mass (Fig. 2).
Fig. 2—32-year-old man with sudden pain after lifting. Left, Coronal reconstruction of CT examination shows hypoattenuating cleft (arrow) through left lower costal cartilage. Right, Axial reconstruction of CT examination shows fracture (arrow) with surrounding hematoma (arrowhead).
MRI provides excellent contrast to show costal cartilage fractures, which will appear as linear areas of high signal intensity against a background of low-signal-intensity costal cartilage [8]. Although MRI has superb spatial resolution and contrast, its relatively higher cost and susceptibility to respiratory motion artifacts decrease its effectiveness, when compared with CT. Ultrasound may also prove useful, given the superficial location of costochondral structures, and may show a focal stepoff at the fracture area [1]. As previously mentioned, costal cartilage injuries may occur at the sternochondral or costochondral junctions. At these locations, chondral and adjacent bone marrow edema may be present on MRI and represent the dominant findings related to traumatic injury. Treatment of costal cartilage injuries include NSAIDs, taping and immobilization belts, and rest for 2–3 weeks. In certain situations, such as treatment of professional athletes, pain can be mitigated by local injections of anesthetic [8]. An important differential diagnosis to consider when entertaining the possibility of a costochondral injury is Tietze syndrome. In this rare entity, inflammation of the sternochondral junction (the most common symptom) can occur spontaneously and lead to focal pain without any specific initiating event. The cause of Tietze syndrome is uncertain, and the condition usually affects younger patients (< 40 years old). On MRI, this entity may show edematous change surrounding the sternochondral junction, which is best seen on fat-suppressed T2-weighted images [10]. CT may not provide enough tissue contrast for adequate detection. Given that Tietze syndrome is usually self-limited, its treatment includes rest, NSAIDs, and local anesthetic injections in refractory cases.
Sternoclavicular Joint
Athletic injuries to the sternoclavicular joint may lead to anterior dislocation (more common and less concerning) or posterior dislocation [11, 12]. The latter phenomenon is less frequent, but more concerning, because the clavicular head has the potential to exert mass effect on the great vessels, trachea, esophagus, and recurrent laryngeal nerve (causing vocal cord palsy). Posterior dislocations require 50% more force to occur, compared with anterior dislocations. This is because the capsular structure of the sternoclavicular joint is more robust posteriorly [13]. Posterior sternoclavicular joint dislocations are most commonly related to direct-force injuries seen in football, rugby, martial arts, and motor vehicle accidents (typically motorcycle accidents). Sternoclavicular dislocations can be imaged by CT and/or MRI, both of which may show malalignment at the joint with associated fractures or hematomas from capsular disruption. In the case of posterior dislocations, CT provides excellent delineation of the joint alignment, and use of IV contrast material allows assessment of the integrity of adjacent vascular structures. Alignment of mediastinal structures and possible hematomas are also best seen on CT. The initial treatment of posterior sternoclavicular dislocations includes attempted closed reduction, which is usually performed under sedation as an urgent procedure. If this procedure fails to realign the joint, or if the joint remains unstable, a surgical approach involving open reduction and internal fixation may be necessary.
Manubriosternal Joint
The manubriosternal joint is rarely involved in athletic injuries. Usual mechanisms of injury are classified as either type 1, in which an anteroposterior force is exerted on the sternal body, which moves posteriorly relative to the manubrium, or type 2, in which the anteroposterior force is exerted against the manubrium [14]. The latter mechanism is usually related to forces being transmitted through the arms to the clavicle and sternoclavicular joints, displacing the manubrium posteriorly. In the author’s experience, such lesions are rare and show marrow edema surrounding the manubriosternal joint on MRI, suggesting local bone contusions. Both sagittal and coronal images through the sternum are optimal for this visualization.
Latissimus Dorsi and Teres Major
Injuries to the latissimus dorsi and teres major muscles are most commonly seen in throwing athletes [15–18]. The latissimus dorsi muscle has a broad origin that includes, among others, multiple spinous processes of the thoracolumbar region and iliac crest; the muscle then attaches at the floor of the intertubercular groove of the humerus. The teres major muscle originates at the posterior aspect of the inferior angle of the scapula and inserts at the medial ridge of the intertubercular sulcus of the humerus. In cadaver studies, the latissimus dorsi and teres major tendon attachments were seen as a single structure in up to 83% of cases [15–18]. In the remaining cases, separate tendons attaching to the humerus were visible on axial images. One important action of these muscles is to powerfully adduct, extend, and internally rotate the humerus. During the throwing motion, the latissimus dorsi and teres major muscles are activated as a unit, with maximum levels of eccentric contraction during the arm cocking and arm deceleration stages of the throwing cycle [15–18]. Lesions of the latissimus dorsi and teres major may present along the usual spectrum of myotendinous strain injuries up to avulsions at the humeral attachments. For this reason, MRI is the preferred imaging method, as it can characterize the full gamut of possible lesions, including those affecting the more dorsal portions of the latissimus dorsi muscle. In this situation, the location of the patient’s symptoms should be considered to ensure adequate coverage on imaging. Because the latissimus dorsi covers a large area of the lateral and posterior chest wall, large FOVs may be required, especially if bilateral imaging is being performed. Another important technical point is to ensure that axial images through the humerus adequately cover the footprints of latissimus dorsi, teres major, and pectoralis major tendons, which are usually not fully viewed during standard shoulder imaging protocols. This may require obtaining axial images that extend caudally to approximately the middle third of the humerus to guarantee such coverage in all patients. Regarding treatment, avulsions at the humeral attachment, which have been described in athletes involved in waterskiing, golf, tennis, and bodybuilding, usually require surgical intervention to reattach the tendons [18]. On the other hand, most myotendinous lesions of latissimus dorsi and teres major muscles are treated conservatively.
Imaging of athletic chest wall injuries should be performed while taking into account anatomic considerations and the advantages of specific imaging methods, including CT, MRI, and ultrasound. Because these injuries are likely to comprise a relatively smaller volume of cases at a given imaging facility, predefined workflows are important to tackle targeted anatomic locations. This may require close communication between scheduling staff, technologists, and attending radiologists, who can tailor protocols to obtain the best images of athletic chest wall injuries.
References
Malghem J, Vande Berg B, Lecouvet F, Maldague B. Costal cartilage fractures as revealed on CT and sonography. AJR 2001; 176:429–432
Chiavaras MM, Jacobson JA, Smith J, Dahm DL. Pectoralis major tears: anatomy, classification, and diagnosis with ultrasound and MR imaging. Skeletal Radiol 2015; 44:157–164
Warden SJ, Gutschlag FR, Wajswelner H, Crossley KM. Aetiology of rib stress fractures in rowers. Sports Med 2002; 32:819–836
McDonnell LK, Hume PA, Nolte V. Rib stress fractures among rowers. Sports Med 2011; 41:883–901
Lord MJ, Ha KI, Song KS. Stress fractures of the ribs in golfers. Am J Sports Med 1994; 24:118–122
Taimela S, Kujala UM, Orava S. Two consecutive rib stress fractures in a female competitive swimmer. Clin J Sport Med 1995; 5:254–256; discussion, 257
Coris EE. First rib stress fractures in throwing athletes. Am J Sports Med 2005; 33:1400–1404
Subhas N, Kline MJ, Moskal MJ, White LM, Recht MP. MRI evaluation of costal cartilage injuries. AJR 2008; 191:129–132
Lee S, Choi YW, Jeon SC. Low attenuation areas in normal costal cartilages on CT: clinical implication and correlation with histology. Clin Anat 2012; 25:483–488
Volterrani L, Mazzei MA, Giordano N, Nuti R, Ga- leazzi M, Fioravanti A. Magnetic resonance imaging in Tietze’s syndrome. Clin Exp Rheumatol 2008; 26:848–853
Mirza AH, Alam K, Ali A. Posterior sternoclavicular dislocation in a rugby player as a cause of silent vascular compromise: a case report. Br J Sports Med 2005; 39:e28
Galanis N, Anastasiadis P, Grigoropoulou F, Kirkos J, Kapetanos G. Judo-related traumatic posterior sternoclavicular joint dislocation in a child. Clin J Sport Med 2014; 24:271–273
Spencer EE, Kuhn JE, Huston LJ, Carpenter JE, Hughes RE. Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002; 11:43–47
Hayashi D, Roemer FW, Kohler R, Guermazi A, Gebers C, De Villiers R. Thoracic injuries in professional rugby players: mechanisms of injury and imaging characteristics. Br J Sports Med 2014; 48:1097–1101
Schickendantz MS, Kaar SG, Meister K, Lund P, Beverley L. Latissimus dorsi and teres major tears in professional baseball pitchers: a case series. Am J Sports Med 2009; 37:2016–2020
Ellman MB, Yanke A, Juhan T, et al. Open repair of an acute latissimus tendon avulsion in a Major League Baseball pitcher. J Shoulder Elbow Surg 2013; 22:e19–e23
Escamilla RF, Andrews JR. Shoulder muscle recruitment patterns and related biomechanics during upper extremity sports. Sports Med 2009; 39:569–590
Cox EM, McKay SD, Wolf BR. Subacute repair of latissimus dorsi tendon avulsion in the recreational athlete: two-year outcomes of 2 cases. J Shoulder Elb Surg Am 2010; 19:e16–e19
Over the last few years, we have heard a lot about resilience. What does resilience really mean? How can we develop resilient teams and organizations? Furthermore, how can we help our patients to be more resilient? Resilience is often defined as the capacity to recover quickly from difficulties. Some equate resiliency with toughness. Another definition of resilience is elasticity, the ability to spring back into shape. Psychological resilience is characterized as the ability to cope mentally or emotionally with a crisis or to return to pre-crisis status quickly [1].
While resilience implies bend-but-don’t-break properties, there are a couple of issues to consider:
We don’t always return to our exact pre-crisis or pre-stress configuration;
Resilience can allow for personal growth and help to catalyze the growth of others.
Regarding our return to our original forms after a jolt to the system, we will never be exactly the way that we were previously. We are older, maybe heavier, maybe hungrier, and maybe more tired. Furthermore, we probably learned something from the stress that we just endured. What we learned can lead to personal growth and the ability to share our new knowledge with others. This process of sharing and helping others has the potential to lead to more resilient teams and to help our patients become more resilient.
Historically, we have thought of resilience in terms of personal resilience—at the individual level. There is no question that personal resilience is important, but resilience can also apply to groups and teams. It is important to consider teams, especially in radiology, as most of our activities are team-related. In fact, very few of our activities do not involve teams. Just think of the process on the front end of any imaging study, before it gets to the radiologist for interpretation: there are schedulers, front desk personnel, nurses, physicists, and technologists. How do we make our teams more resilient and more effective?
One of the drivers for engaged, resilient teams is relational energy. Leaders with relational energy create a positive environment with higher levels of engagement, lower turnover rates, and enhanced feelings of well-being [2]. On the other hand, there are leaders who drain energy from the group, and the team members loathe working with an idea-killing, energy-sapping leader. In the book Multipliers: How the Best Leaders Make Everyone Smarter [3], Liz Wiseman discusses two types of leaders: The first group are diminishers, draining intelligence, energy, and capability from the people around them, and the second group are multipliers, leaders who employ their skills to amplify the strengths and the capabilities of those around them.
Multipliers can have a major impact on our teams and organizations in radiology. In this ever-changing, peri-pandemic world, multipliers can make us all more resilient, by doing more with less, by attracting and developing talent, by creating a safe environment that allows for our best thinking, by challenging us to push beyond what we know, by debating decisions, and by instilling ownership and accountability. Furthermore, multipliers do not need to be great at everything. Rather, effective multipliers should have some very solid strengths and few major deficiencies. In addition, effective multipliers often choose to form teams with others who bring complementary strengths to the table [3].
As we navigate the challenges of our topsy-turvy world with a major war in Europe, political divisiveness and the great resignation in the United States, and rising inflation, and as we try to re-equilibrate in the peri-COVID world, we need to be resilient as we continue to move our field forward and deliver top-notch care to our patients. Our patients really need us, not just to read their images and do their procedures, but to advocate for them with empathy and dignity.
When we go to work, it may be a good day, a bad day, or a usual, non-descript day. Often, our patients are seeing us on what may be their worst day ever or what they fear will be their worst day ever. I recently spoke with a patient who was diagnosed with a cervical plasmacytoma in 1994. Soon thereafter, he was shown to have multiple myeloma involving several sites in the cervical, thoracic, and lumbar spine. Despite chemotherapy, radiation therapy, an autologous stem cell transplant, and experimental therapy, he was told that his chances for survival were less than 5%. With each imaging study came the dread that more disseminated disease would be found. Nevertheless, during those encounters, he found front desk personnel, technologists, and physicians to talk to. Even amidst a downward cycle of relapses and remissions, a radiation oncologist suggested that he consider sperm preservation (he was single at the time).
Let’s fast forward to 2022, when the patient is a 30-year survivor of multiple myeloma, leading a foundation to help multiple myeloma patients; he is happily married, and his son is a college graduate! The patient was in a “very dark place” 25 years ago, worried that he would never see or know his son, and now, miraculously, he is a long-term myeloma survivor.
There are countless patients who come to us every day on their journeys of resilience. We have an obligation to engage them, to treat them in a dignified professional manner, and, hopefully, what was anticipated as a very bad day may not be so bad for them.
As we think about building resilient teams and resilient enterprises, it is important that we promote and practice empathetic, patient-centered behaviors. We need to be multipliers for our patients.
Recently, I performed a biopsy on a small right breast mass on a 44-year-old woman. The procedure went smoothly, and the biopsy showed evidence of a papilloma. A few days after the biopsy, the patient’s referring clinician contacted me, informing me that the patient had a 4th ventricle ependymoma resected at age 5 years, and that the patient had diminished mental capacity. Immediately after the biopsy, the patient’s mother had asked to speak to me, but she was told that I was busy and that she should check the electronic medical record. I do not know who communicated with the patient’s mother, but I certainly would have made myself available to talk to her. As we try to be multipliers for our patients, we need to do better each and every day.
As we try to be resilient in this ever-changing world and form resilient radiology teams, we should keep in mind these words from the Cadet Prayer at West Point: “Make us choose the harder right instead of the easier wrong, and never be content with a half-truth when the whole truth can be won” [4]. We need to choose the harder right; our patients are depending on us.
Director of Oncological Imaging; Abdominal Radiology Beth Israel Deaconess Medical Center
Kathryn J. Fowler
Associate Professor of Radiology University of California San Diego Health
Most of us spend more than half of our waking hours at work, where we interact with peers, report to supervisors, and, potentially, manage teams. While work is gratifying to many of us in this specialty, only a minority of radiologists report being happy. In a Medscape survey conducted in 2017, only 25% of radiologists claimed to be happy at work, 47% reported that they experienced burnout and/or depression, and 50% of respondents attributed long work hours as the cause for their burnout. Unhappiness and burnout can lead to downstream impacts. Those experiencing burnout and/or depression report higher levels of exasperation with their team members, as well as decreased levels of engagement. This can lead to a dysfunctional team environment, which, in turn, can further negatively impact professional satisfaction in the workplace.
In contradistinction, being a respected and productive member of a high-functioning team contributes substantially to one’s happiness at work. However, few of us are lucky enough to join a team that naturally functions with reliable precision and success. Creating and maintaining a highly functional team may even seem as elusive as magic.
Magic may not be needed, but skills and effort are required to create a cohesive team. By working to improve social and emotional intelligence, and maintaining a culture of clear and open communication, one can cultivate a hopeful, supportive environment. This, in turn, fosters a growth mindset that allows us to learn from, and not fear or create conflict with, opinions that diverge from our own. Ultimately, with appropriate skills and insights, we can manage adversity and succeed.
One of our favorite examples of managing adversity can be seen in the popular show, Ted Lasso. Ted, an American football coach, is recruited to England to coach a professional soccer team, AFC Richmond. In addition to his ignorance of the game of “proper football,” he faces severe adversity from the team and its inherent dysfunction, as well as deliberate sabotage, in some instances, from superiors. Yet, in the end, Ted triumphs against all odds. Over the course of two seasons, Ted builds a team we all dream of having: driven, united, inclusive, diverse, cohesive, and effective. Ted’s team is one where each member’s unique perspective and talents are valued, where each member is given an opportunity to become the best version of themselves, where each member is supported and lifted up. While such a team sounds too good to exist outside of a TV show, Ted’s off-the-chart emotional intelligence skills, his kindness, his mindset of hope and optimism—if implemented in real life—can bring the environment of our own teams closer to that of AFC Richmond.
The concept of emotional intelligence (i.e., emotional quotient or EQ) is a relatively recent one, yet it is crucial to personal and professional success. Emotional intelligence constitutes several key soft skills (i.e., skills related to one’s function in a team) for understanding and managing emotions of self and others. By recognizing emotions, both positive and negative, and understanding their meaning, you can interpret them as data to help inform actions and ensure your intentions translate appropriately to others. In addition to emotional awareness, empathy and social skills contribute to high EQ.
You may be thinking, “I’m just not good at this stuff!” In response, we will quote Ted Lasso: “Well, when I was a baby, I wasn’t good at walking and talking, but I stuck with it, and look at me now.” Soft skills are crucial to professional success, yet are rarely formally taught. Our 2022 ARRS Annual Meeting Sunday Session, “Sharpening Teamwork and Communication Skills,” will provide a framework to start honing the many soft skills that are important to the success of both individuals and teams, including:
High-yield understanding of the intricacies of team dynamics
Leveraging the psychology of interpersonal communication
Pro tips for sending and receiving effective emails
Acknowledging the interdependence of communication styles and leadership abilities
Expert strategies for combating imposter syndrome
Practical advantages of inclusivity
Following this featured Sunday Session, participants will have a solid understanding of the broad range of soft skills needed to facilitate effective leadership and membership in a team environment. To quote our favorite coach, “Success is not about the wins and losses; it is about [players] becoming the best versions of themselves, on and off the field.”
Associate Professor Department of Radiology, Musculoskeletal Imaging Section UT Southwestern Medical Center
Hillary W. Garner
Assistant Professor of Radiology Mayo Clinic Florida
Some of you may remember the time when your voice recognition stubbornly transcribed “pulmonary edema,” even though you clearly said “bone marrow edema.” One of the co-moderators of our 2022 ARRS Annual Meeting Sunday Session, “Practical Applications of Computational Science in Musculoskeletal Imaging,” was a second-year resident when voice recognition was first implemented in his department. His faculty and co-residents were divided on whether to welcome or resist this new technology. The issue was not about young versus old, or tech savvy versus not, but about whether or not the technology was ready for prime time. Initially, voice recognition was not as accurate as advertised. It took time for the software to mature to its current, more robust form.
Years later, the moderator was taking an online introductory artificial intelligence (AI) course, during which the technology behind voice recognition was explained. Contrary to his early assumption, the software was not trying to transcribe phonemes into the exact words. Instead, it was listening to chunks of speech within sentences and assigning probabilities to what was being said, ultimately displaying the highest probability word(s) related to the overall context. Large amounts of voice and context data were required for the software to be able to achieve high accuracy and allow for appropriate probability models for various users in different subspecialty settings.
Today, we hear about AI and other computational technologies achieving unbelievable feats. We are approached by salespeople who already have FDA-approved software that can perform tasks that were only achievable by the human mind just a few years ago. Some of these computer and data science solutions will be able to stand the test of time. Other solutions will seem incredibly promising but inevitably fail. Regardless of which solutions persevere, very few people in health care have a firm understanding of how these technologies work and what limitations they may have. As physician leaders, we need to narrow this knowledge gap to help contain costs and to better serve and protect our patients. To achieve these goals, we need to improve our ability to judge available solutions, including their potential benefits and drawbacks, as well as their probability of wide adoption and success. Having a basic understanding of how things work in computational science is therefore becoming as necessary as being able to read, write, and do basic arithmetic in today’s rapidly advancing high-tech world.
During “Practical Applications of Computational Science in Musculoskeletal Imaging,” you will hear from fellow physicians on various topics that integrate computer science and musculoskeletal imaging, including automated evaluation of arthritis, use of AI in speeding up MRI acquisitions, automating measurements of bone loss, and performing fat versus muscle mass measurements. Furthermore, we hope to answer some popular questions in the realm of musculoskeletal AI, such as where we are today regarding a completely automated solution in fracture detection on radiographs and what it means for a software solution to be FDA approved, as opposed to FDA cleared. You will also hear about potential pitfalls and biases that AI may introduce. We hope that you will join us in learning more about this exciting and continually evolving aspect of musculoskeletal radiology.
Unlike any prior time period in our history, the contemporary workplace will soon encompass five different generations, distinguished variously, but typically defined and labeled by year of birth. Here, I’m referring to Baby Boomers (1946–1964), Generation X (1965–1980), Generation Y or Millennials (1981–1995), Generation Z (1996–2010), and the forthcoming Generation Alpha (2011–2025). Largely driven by the advertising world, hoping to better target their marketing campaigns, efforts have been made to easily distinguish these groups based on social influences, generational values, behaviors, and preferences.
I suspect that these labels may have complicated matters even further. For example, the COVID-19 pandemic-induced shift to the virtual workplace may well have exacerbated intergenerational tensions in areas where groups are supposed to differ. Think social interactions, communication preferences, work-life integration and wellness strategies, perceptions of technology usage, and willingness to change. These differences must surely have led to breakdowns in communications, team function, and clinical performance, among many others.
On one hand, these age-based delineations can be a helpful reference point, particularly when leading multigenerational teams. There are some proposed defining factors, such as cultural movements, historical milestones, technological advancements, learning preferences, and lifestyle traits for each period that can be interesting to delve into and see whether they resonate with yourself and your teams. These features can be lively conversation starters and help you glean insight into how best to manage morale and burnout, as well as create more inquiry, respect, and open-mindedness among such a diverse population. However, surely additional factors beyond age should be equally impactful; consider background experience and training, levels of maturity, tenure within an organization, and lineage in a role.
Is it possible that the COVID pandemic has influenced societal perceptions of generations, and might the pandemic influence the formation of generational identities for those still in formative years?
It seems to me that this is a very opportune time to work to address and dispel age-associated or generational stereotypes.
Dispel the Myths
That said, it’s so important that we inquire, appropriately and respectfully, about the stories of others to expand upon—and maybe even rebut—marketing matrices.
Upon reflection, I don’t think that people neatly fit into their age-based silo. As I look across the multigenerational tables as a Baby Boomer by age, I certainly have “silo creep” and span several different buckets. You might think World War II, for example, was a defining life event for me, but that wouldn’t be true. Rather, I grew up as a relatively privileged individual during the segregated South African apartheid era, which left an indelible impact on my values, philosophies, and priorities.
I know I’m not alone here. When speaking with a millennial colleague, it became clear that these categories are not cut and dried:
“I think some of these characteristics are pretty broad generalizations. I am part of the millennial category, but it has never quite resonated with me. Millennials are often painted in an unfavorable light, such as when it comes to work ethic, world views, and materialism, just as Baby Boomers can be criticized for not being tech-savvy, and seniors can be stereotyped as dependent and frail.”
“My father, a Baby Boomer, studied computer science as an undergraduate, before it became an official degree program at Boston University. My grandfather, a member of the Silent Generation, ran his final Boston Marathon in 4 hours and 30 minutes at age 72 and continued to participate in road races into his 80s. To me, labels can be tough because they don’t allow for nuance and individuality; they don’t tell the whole story.”
It’s easy to jump on the bandwagon and affirm negative generalizations, but this can be damaging when it comes to building an inclusive team. We must ensure these categories, simply based on a number, don’t serve as a detrimental springboard for misunderstandings about behaviors and preferences.
Seek Data and Understanding
It’s our responsibility as leaders to build diverse teams and foster respectful environments for every member of our workplace and beyond. We can strive to enact change at the national level, such as by communicating the importance of accommodating different learning styles for different generations at major conferences and advocating for educational material that best suits the learner (e.g., didactic talks vs. handouts vs. podcasts, etc.).
Locally, we can commit to better understanding our colleagues on a one-on-one basis. If one generation prefers frequent, regular, unvarnished feedback, provide that. If possible, be willing to adapt traditional annual reviews to meet worker preferences. Support departmental social media initiatives but be respectful of those who might not wish to expand their digital presence at this time. You’ll find that some cohorts might thrive on multitasking, while others prefer to focus on tasks linearly. Take all of these factors into consideration.
Ask, listen, collect data, and repeat. Run a short quarterly communication survey asking how employees prefer to receive information within the department, or whether digital Grand Rounds lectures are meeting their academic needs. Sometimes, simply listening and giving people a choice can make all the difference when it comes to feeling a true sense of appreciation and belonging at work.
Not fully understanding the complexities of our multigenerational workforce has been described as a contributor to workplace stress and burnout. Challenges managing, building, and leading multigenerational teams have been recognized, yet solutions have not. We must first hear from our colleagues directly. For example, you might ask a more seasoned colleague what it was like when they first started out in radiology. How have things changed over time? In their perspective, has it generally been for the better, or have there been obstacles along the way? How has patient care evolved? Older generations might consider asking younger generations about what their highly digital academic training experiences are like today. When an opportunity presents itself, respectfully inquire and listen to build connections and understanding.
Celebrate Our Diversity of Ages
One good aspect of the multigenerational descriptors is that they remind us of the remarkable diversity of values, preferences, and skills that we are so fortunate to have in our workforce. Understanding, embracing, welcoming, including, and being respectfully inquisitive about these differences will serve us far better. Acknowledging that differences exist and committing to learning about them is a lifelong journey.
Starting today, instead of trying to transform one generation to adjust to another, let’s:
celebrate the diversity of ages in our workforce
embrace all skills, expertise, and experiences
focus on intentional inclusion activities
shift the focus away from this single cultural descriptor (age) and build teams that are as diverse as possible
avoid alienating labels and siloes and stereotypes
Never before have four different generations worked together in Beth Israel Deaconess Medical Center radiology, bringing different values, preferences, communication styles, strategies for work-life integration, and wellness approaches into the milieu. The list of differences is extensive and complex. What a terrific and timely opportunity to embrace! A field such as imaging is so dependent on the structure and function of high-performing teams. Therefore, it behooves us to better understand the different generations and explore how best to take advantage of these opportunities.
I would love to hear about how you are tackling this intricate topic at your own institutions. If this subject resonates with you and/or you are inclined to share, please feel free to email me directly: jkruskal@bidmc.harvard.edu.
Assistant Professor of Radiology Wake Forest School of Medicine
Erik H. Middlebrooks
Professor of Radiology Program Director, Neuroradiology Mayo Clinic College of Medicine and Science
The transition from trainee to independent radiologist represents a pivotal time full of opportunities and challenges. In our experience, navigating this transition is often simultaneously exciting and intimidating. Although many of the associated opportunities and challenges are common to both private and academic practice, others may be unique to one’s specific practice environment.
For example, after training, it is important that all radiologists be able to perform high-quality clinical work autonomously and efficiently. Additionally, building trust and earning the respect of referring physicians is advantageous for all radiologists desiring to become a “go-to” imager for challenging cases and difficult clinical problems. However, newly minted academic radiologists are often also interested in developing educational content and research programs, whereas new private practice radiologists may choose to focus on honing their business acumen.
In our experience, most residents and fellows receive outstanding clinical radiology education; however, their non-clinical professional education is commonly more variable. As such, many trainees and junior attending radiologists stand to benefit from educational programming dedicated to the development of important non-clinical professional skills and from the opportunity to interact with and ask questions of knowledgeable experts that may not otherwise be easily accessible. Fortunately, radiology is replete with experts who are more than willing to share their knowledge and experience to help others, particularly for the benefit of young professionals.
This course featured a diverse group of highly successful radiologists representing perspectives from the private and academic practice settings. These radiologists shared practical knowledge and lived experience related to professional challenges frequently encountered by young radiologists that are less frequently covered by traditional residency and fellowship didactic curricula. The selected topics are particularly relevant for young professional radiologists (e.g., residents, fellows, junior academic faculty, and junior private practice associates) preparing for or currently navigating the transition from trainee to independent radiologist, regardless of private or academic practice setting. Faculty emphasized practical pearls they wish they had learned earlier.
More specifically, didactic presentations covered:
the benefits of active participation in radiology societies, like ARRS, for early career success,
critical aspects of personal and practice-related finances,
the importance of and successful strategies for building advantageous professional relationships,
the value of branding for individual and practice success, as well as practical tips for effectively developing and professionally promoting one’s individual and group practice brands
Project Leader, Imaging Physics; Applied Physics Division Codirector, MRI Biomarker Measurement Service National Institute of Standards and Technology, US Department of Commerce
Karl F. Stupic
Director, MRI Biomarker Measurement Service National Institute of Standards and Technology, US Department of Commerce
Kathryn E. Keenan
Project Leader, Quantitative MRI; Applied Physics Division National Institute of Standards and Technology, US Department of Commerce
Medical imaging is rapidly advancing and includes many modalities: ultrasound (US), MRI, radiography, CT, PET, SPECT, and optical coherence tomography. New modalities, such as digital breast tomography and low-field MRI, are being integrated into the clinical workflow. Multimodal imaging, such as PET/CT and PET/MRI, and combined imaging therapy, such as MR linear accelerator, are rapidly expanding. Additionally, the amount of data extracted by radiologists by eye, via complex analysis tools, and using AI-based systems is dramatically increasing. Radiologists require that data are accurate and reproducible. To ensure this, calibrations and standards are needed. Phantoms—imaging calibration structures—are used to ensure scanner accuracy, stability, and comparability. Phantoms need to be readily available, easy to use, and have accurate and traceable components. In addition, imaging and analysis protocols must be rigorously validated, and the fundamental measurands, image-based biomarkers, must be carefully and precisely defined.
Many organizations have programs to assist in making image-based data more precise and reliable, including the Radiological Society of North America Quantitive Image Biomarker Alliance, National Cancer Institute Quantitative Imaging Network, American College of Radiology (ACR), National Institute of Biomedical Imaging and Bioengineering (NIBIB), National Equipment Manufacturers Association, American Association of Physicists in Medicine, International Society for Magnetic Resonance in Medicine (ISMRM), National Physical Laboratory (United Kingdom), Physikalisch-Technische Bundesanstalt (Germany), and the National Institute of Standards and Technology (NIST). NIST, the US national metrology institute, has been assisting clinical, research, and medical device organizations in the development and dissemination of medical standards for over 100 years. An early example from around 1905 (Fig. 1) depicts calibration equipment and commercial medical mercury thermometers.
Fig. 1—Medical mercury thermometers and NIST calibration apparatus, circa 1905. (Courtesy of NIST)
In the early 1900s, getting a universally accepted temperature scale was a critical issue. The need for medical metrology and standards has grown since then, and it is a critical part of our health care infrastructure. Below, we look at some recent NIST activities in standards for quantitative MRI.
Scanner Performance
Understanding and monitoring scanner performance is essential. Critical parameters include geometric distortion, resolution, signal-to-noise ratio, and image uniformity. An example of MRI geometric distortion and image uniformity measurements are shown in Figure 2; the measurements were made using an MRI system phantom developed by NIST and ISMRM. The geometric distortion is due to nonuniform gradients, and it is important to understand both the intrinsic distortion and the efficacy of the distortion corrections, often applied after imaging. A 3D gradient-echo scan can give the accuracy of the gradient calibrations, accuracy of distance and local volume measurements, and presence and efficacy of post-scan corrections.
Fig. 2—Photo and images of MRI system phantom. (A) shows image uniformity map take on 3T scanner using head coil thorough 200 mm spherical volume. (B), (C), (D), and (E) show geometric situation—difference between apparent position of each fiducial sphere and real position (modified from Magn Reson Med with permission from ISMRM).
Figure 3 shows an image of an ACR-type resolution inset, along with a synthetic image: an ideal image for the pulse sequence used. Then, the synthetic image can be modified, by including blurring, to match the observed image. Protocol dependent resolution, scanner resolution, and other nonidealities can be quantified.
Fig. 3—(A) MRI of ACR-type resolution inset, (B) synthetic image (ideal image, given pulse sequence), (C) synthetic image modified to include finite scanner resolution to make synthetic image match observed image, (D) minimization of difference between image and synthetic image (modified from Magn Reson Med with permission from ISMRM).
Intersite Comparisons
Intersite comparisons are critical to determine how accurately image-based biomarkers can be measured. Proton spin relaxation times, T1 and T2, are useful biomarkers to distinguish tissue types and healthy from unhealthy tissue. A recent multisite study comparing MRI T1 measurements shows considerable variation using common protocols, including an inversion recovery protocol, which, albeit too time-consuming for clinical use, is considered a gold standard. Figure 4 shows the deviation in measured T1 from NIST reference measurements, which have a well-defined uncertainty. The uncertainty defines an interval about the measured value within which there is a 97% probability that the real value will lie. One can see that there is considerably more uncertainty in the scanner measurements, and there is a vendor-dependent bias. Being able to define uncertainty intervals in image-based biomarker measurements, with traceability to the international system of units, is an important challenge for our community.
Fig. 4—Results from T1 multisite study showing deviation of measured T1 times using an inversion-recovery protocol from NIST reference values for different scanner vendors. Gray box shows uncertainty interval for reference values (modified from PLoS ONE with permission from Public Library of Science).
Validating Complex Biomarkers
There are many complex MRI-based biomarkers, including proton spin relaxation times, proton density, fat fraction, water diffusion coefficient, diffusion kurtosis, anisotropic diffusion parameters, tissue elasticity, local concentration of metabolites and neurotransmitters, blood flow, and perfusion parameters. Diffusion-based biomarkers are a good example of the challenges encountered getting precise and useful in vivo measurements. There is a hierarchy of parameters that can be measured with increasingly complex models. The more complex models (e.g., diffusion spectral imaging [DSI]) can provide more information about underlying tissue, but validation, standardization, and implementation are more difficult. Simple models, such as extracting the apparent diffusion coefficient (ADC), can be very informative and useful, but limitations of the model must be addressed in the accuracy and uncertainty analysis. The phantom below (Fig. 5) contains both isotropic and anisotropic and diffusion elements to test the accuracy of many different types of diffusion-based measurements, including ADC and DSI parameters.
Fig. 5—Comprehensive phantom with anisotropic and isotropic diffusion components developed for Department of Veterans Affairs to monitor MRI system parameters relevant to brain health. (Courtesy of NIST)
Phantom Lending Library
To assist clinical sites, research centers, scanner manufacturers, and phantom venders, NIST and NIBIB have established a medical phantom lending library containing calibrated traceable phantoms available for short-term loan. MRI system phantoms, diffusion phantoms, breast, and cardiac phantoms are available for loan with associated calibration documents, databases, and analysis software. Incorporation of phantoms into the lending library allows clinical and research sites easy access to phantoms, new imaging and measurement protocols to be validated on a common set of calibration structures, and phantoms to be curated with long-term stability established. Convenient access to standard calibration structures should facilitate the development and validation of improved measurement protocols and establish a framework to provide uncertainty intervals on image-based measurements.
Medical imaging scanners are sophisticated and powerful tools that can be extended to metrology systems, capable of making precise in vivo measurements of many different structural and functional tissue parameters. The work by the many institutions listed here is making this transition possible. Medical imaging metrology and standards are important components of this transition and the US medical/health care infrastructure. They often run in the background, but neither should be overlooked.
The Pelvic Floor Disorders Consortium (PFDC) is a multidisciplinary organization of radiologists, colorectal surgeons, urogynecologists, urologists, gynecologists, gastroenterologists, physiotherapists, and other advanced care practitioners—formed to bridge gaps and enable collaboration between these specialties. Specialists from these fields are all dedicated to the diagnosis and management of patients with pelvic floor conditions, but given the differences in their respective training, they approach, evaluate, and treat such patients with their own unique perspectives.
In a multisociety-endorsed article in the October edition of AJR (published concurrently with Diseases of the Colon & Rectum, International Urogynecological Journal, and Female Pelvic Medicine and Reconstructive Surgery Journal), the 24 members of the PFDC Working Group on MRI reached consensus regarding many clinically relevant considerations for performing, interpreting, and reporting MR defecography (MRD). Based upon the PFDC Working Group’s consensus guidelines, corresponding synoptic interpretation templates were suggested for this unique patient population.
Contrast Medium Considerations
On the basis of the literature and their collective expertise, the PFDC Working Group advised that MRD should be performed with rectal distention, using rectal contrast medium, and with image acquisition during defecation. Rectal distention and defecation are both crucial components of MRD that distinguish the examination from simple dynamic pelvic floor MRI performed with the Valsalva maneuver. Moreover, compared with Valsalva images, prior AJR research has shown larger, more recurrent prolapse on MRD examinations with rectal distention and on defecation images. [4] (Fig. 1).
Fig. 1—59-year-old woman with history of rectal bulge and sensation of incomplete defecation. B = bladder, R = rectum, V = vagina. A–C, Sagittal steady-state images at rest (A), Valsalva (B), and defecation (C) show bladder, vaginal apex (asterisk), and anorectal junction (dashed arrow) at or above pubococcygeal line (PCL) (line) at rest (A). During Valsalva (B), bladder extends below PCL and there is small cystocele (solid arrow), vaginal apex is lower than at rest (asterisk) but remains above PCL, and there is descent of anorectal junction (dashed arrow). During defecation (C), there is significantly larger descent of bladder below PCL and enlargement of cystocele (solid straight arrow), vaginal apex now prolapses below PCL (asterisk), and there is significant descent of anorectal junction below PCL (dashed arrow). There are also anterior (left curved arrow) and posterior (right curved arrow) rectoceles.
Technique and Reporting/Grading of Relevant Pathology
Apropos of so many differing clinical backgrounds, the PFDC Working Group debated which of two grading scales to utilize for internal rectal intussusception: descriptive reporting or the Oxford Grading Scale [5]. After much deliberation, the panel agreed that a uniform description of rectal intussusception as intrarectal, intraanal, or complete external (extraanal) would provide adequate clinical details to be deemed the minimum reporting standard.
Ultimately, these consensus definitions and interpretation templates can be augmented with additional radiologic maneuvers and report elements—specific patient indications, health care provider preferences, local practice patterns, etc.—”but the suggested verbiage and steps should be advocated as the minimum requirements when performing and interpreting MRD in patients with evacuation disorders of the pelvic floor,” the 15 coauthors of this AJR article concluded.