Tanya Moseley Professor of Diagnostic Radiology Department of Breast Imaging University of Texas MD Anderson Cancer Center
The ultimate game-changer in the breast biopsy world, stereotactic-guided breast biopsies allow breast imagers to offer their patients an amazing alternative to surgical biopsy. Not only is there a shorter recovery time compared to invasive surgical biopsies, but stereotactic core biopsy also leaves little to no scarring on the breast.
From theory to application, workshop participants will acquire a comprehensive understanding of breast biopsy indications, breast lesion characteristics, and modern breast imaging modalities. Whether you are an experienced practitioner or just commencing your breast biopsy voyage, our Featured Session will provide every tool you need to confidently and deftly navigate difficult scenarios, including both deep and superficial breast lesions, as well as patients with small, thin, or augmented breasts.
For emerging or unfamiliar technology, nothing beats a live demonstration of it—a proof of concept and the processes that make it easier to grasp everything. Instead of relying solely on textbook teaching or typical lecture-and-slides didactic session, our “Ready, Set, Stereotactic-Guided Breast Biopsies” presentation will allow radiologists to witness several really cool aspects of stereotactic core breast biopsy . . . up close!
An effective live demo, though, leverages its innate interactivity, welcoming everyone to become active participants in the continuing educational process. To that end, our esteemed subspecialized faculty have also prepared specific case-based examples to showcase this minimally invasive procedure for breast lesions only visible on imaging.
What further sets “Ready, Set, Stereotactic-Guided Breast Biopsies” apart is ARRS’ commitment to real-world knowledge, bridging the gap between abstract idea and practical implementation. Exploring the fascinating connections among anatomy and pathology, technique and technology, we will remain focused on the everyday nuances that arise in private, academic, and in-training breast imaging. Leaving no clinical stone unturned, you will leave us knowing how to best audit your own practice.
Fun and educational alike, our Featured Session and live demonstration on Sunday, May 5 satisfies two of the three hours of Category 1 CME for radiologists qualified as an interpreting physician under the Mammography Quality Standards Act.
Department of Internal Medicine, San Juan City Hospital, Puerto Rico
Efrén J. Flores
Department of Radiology, Massachusetts General Hospital
Despite the advancements in diagnosis and treatment, lung cancer (LC) remains the leading cause of cancer-specific mortality with an estimated 235,760 new cases and 131,880 deaths in 2021 [1]. Although LC affects all races and ethnicities, disparities in LC outcomes and mortalities exist. Barriers related to medical and sociodemographic factors, including language, access to smoking cessation resources, LC stigma, and health literacy, among other social determinants of health, are factors that play a role in the existing disparities in the LC care continuum [2, 3]. Lung cancer screening (LCS) can serve as a pillar to bridge disparities in LC outcomes through primary risk reduction with smoking cessation and secondary risk reduction with LCS [4]. However, despite the proven benefits of LCS in reducing LC mortality, only a fraction of the eligible population has been screened, and the proportion of individuals eligible for LCS among underserved populations is likely to be lower [5]. The ongoing COVID-19 pandemic, which has exacerbated health disparities among racial/ethnic minority communities and other underserved communities, has resulted in diversion of medical resources to address immediate needs [5, 6]. The effects of postponing nonurgent medical care, including LCS, because of the pandemic are unknown. Without targeted outreach, the low participation rates and delays in LCS will widen existing disparities in LC outcomes among underserved communities [6].
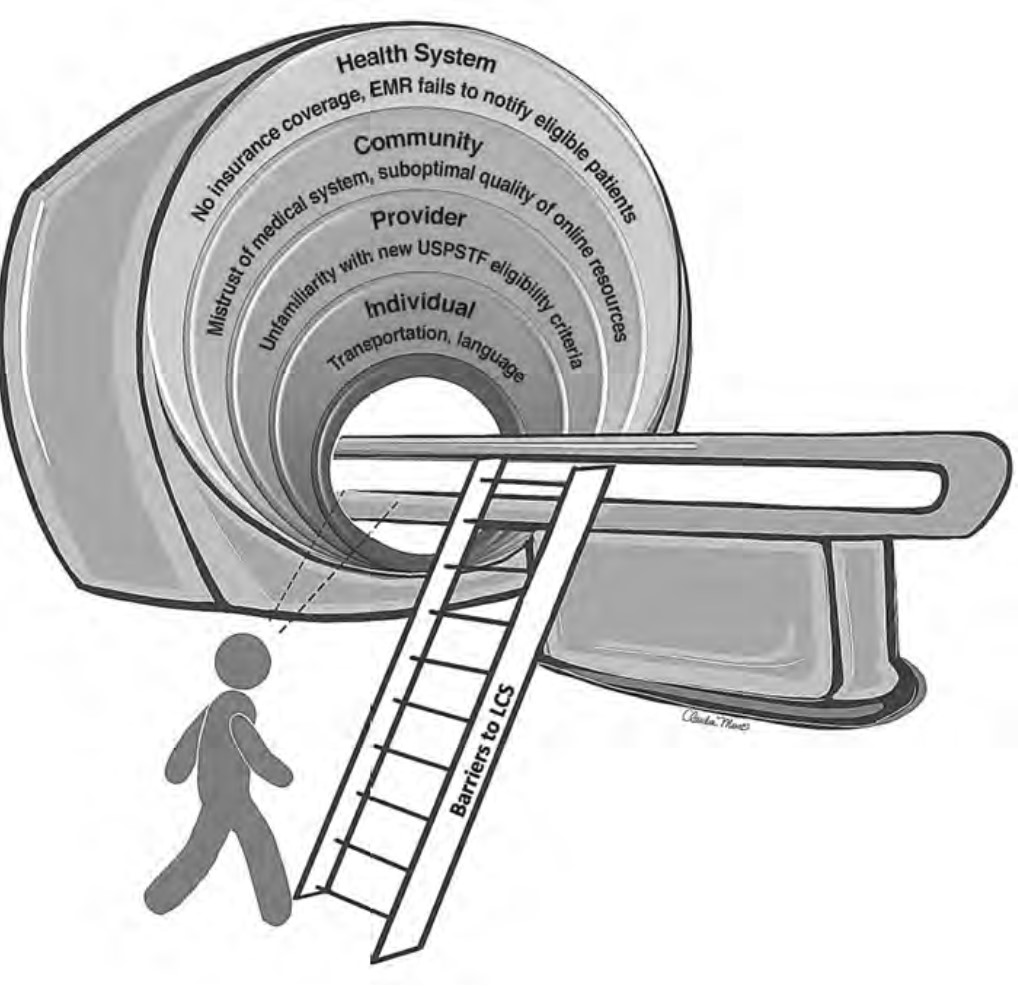
The recent update in the U.S. Preventive Services Task Force (USPSTF) LCS eligibility guidelines lowers the required smoking history to 20 pack-years and age to 50 years [7]. This provides an opportunity to improve overall LCS participation rates among diverse patient populations through tailored approaches that consider barriers related to social determinants of health. Therefore, it is vital that we take steps to understand barriers to LCS and develop targeted multilevel outreach interventions to increase LCS participation rates. The purpose of this InPractice piece is to use a modified social-ecologic model of barriers to LCS (Fig. 1) to discuss multilevel interventions and advance equity in LCS uptake among diverse patient populations by increasing awareness, opportunities, and participation in LCS (Table 1). This framework can be adapted to advance equity in LCS among radiology practices in different settings.
Fig. 1—Drawing shows social-ecologic barriers to lung cancer screening (LCS) that many patients encounter before undergoing LCS at individual, provider, community, and health system levels. EMR = electronic medical record, USPSTF = U.S. Preventive Services Task Force.
Barriers to and Facilitators of Lung Cancer Screening Awareness
Barriers
At the individual level, some of the barriers to awareness include unfamiliarity with LCS as a health preventive service tool (Fig. 2), unawareness of the new USPSTF and Centers for Medicare & Medicaid Services (CMS) recommendations for LCS, unfamiliarity with insurance coverage and costs, uncertainty about available accredited LCS programs, lack of culturally appropriate information, and lack of information at an appropriate health literacy level [8–10].
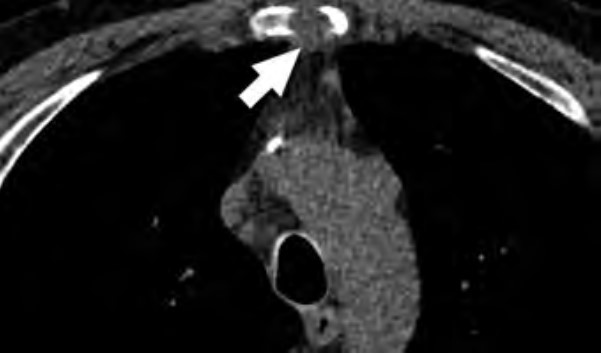
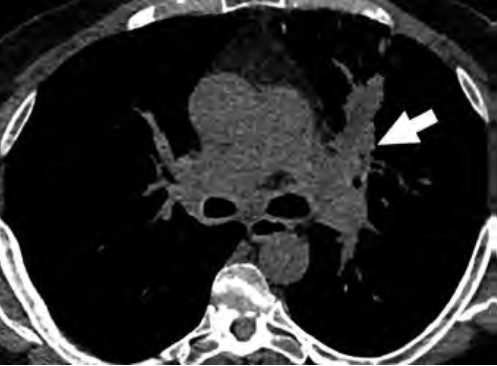
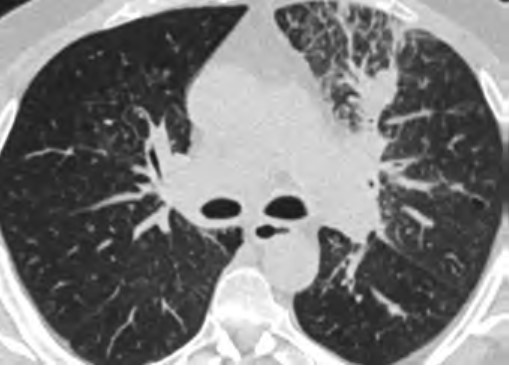
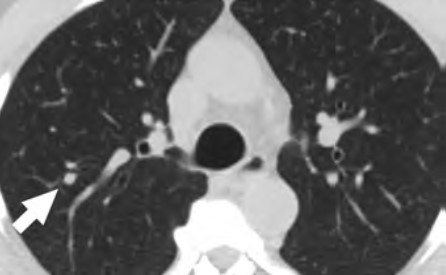
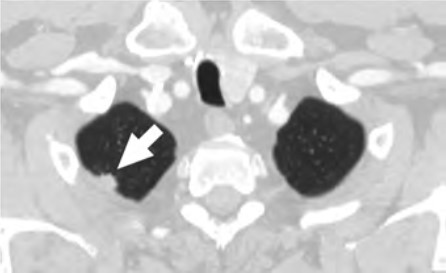
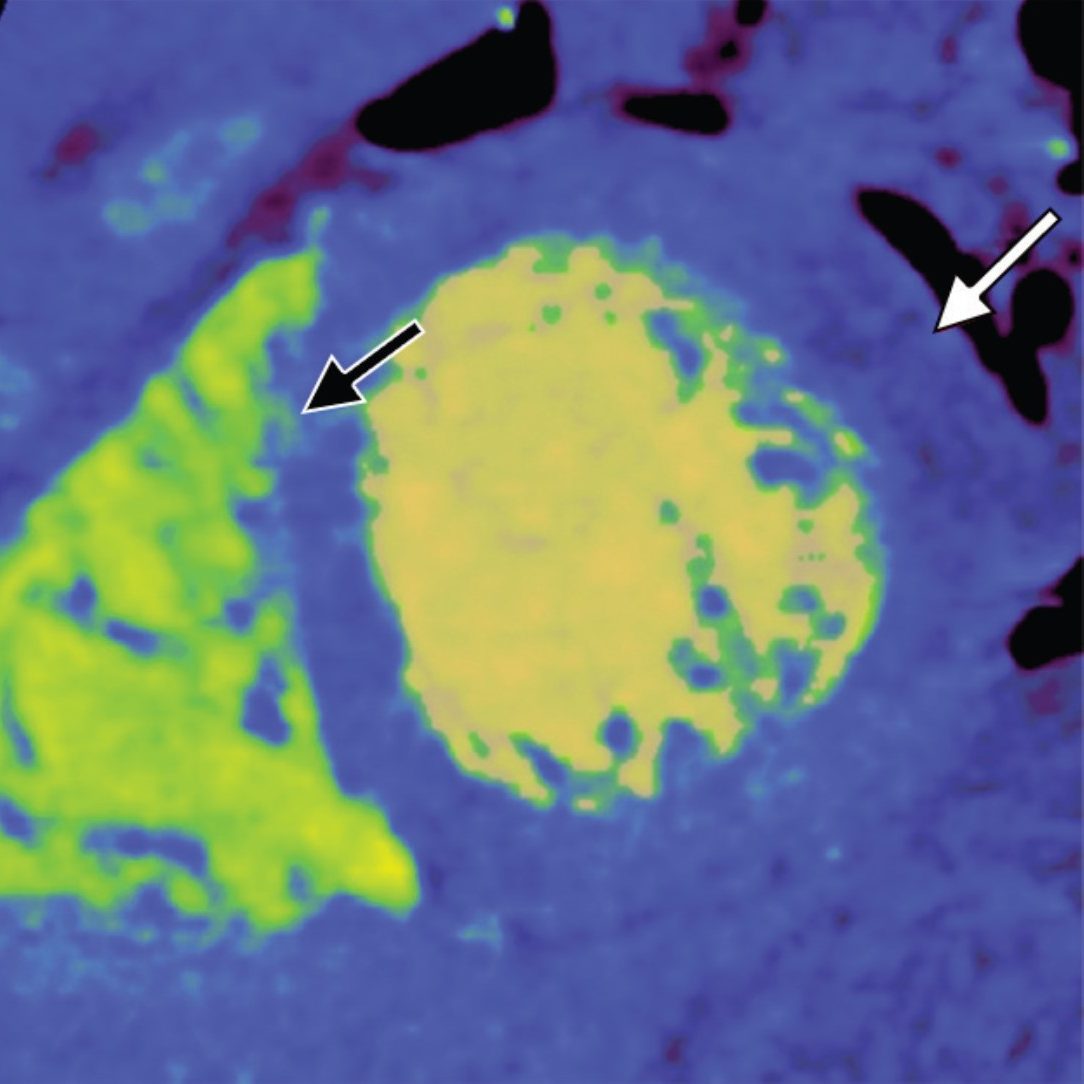
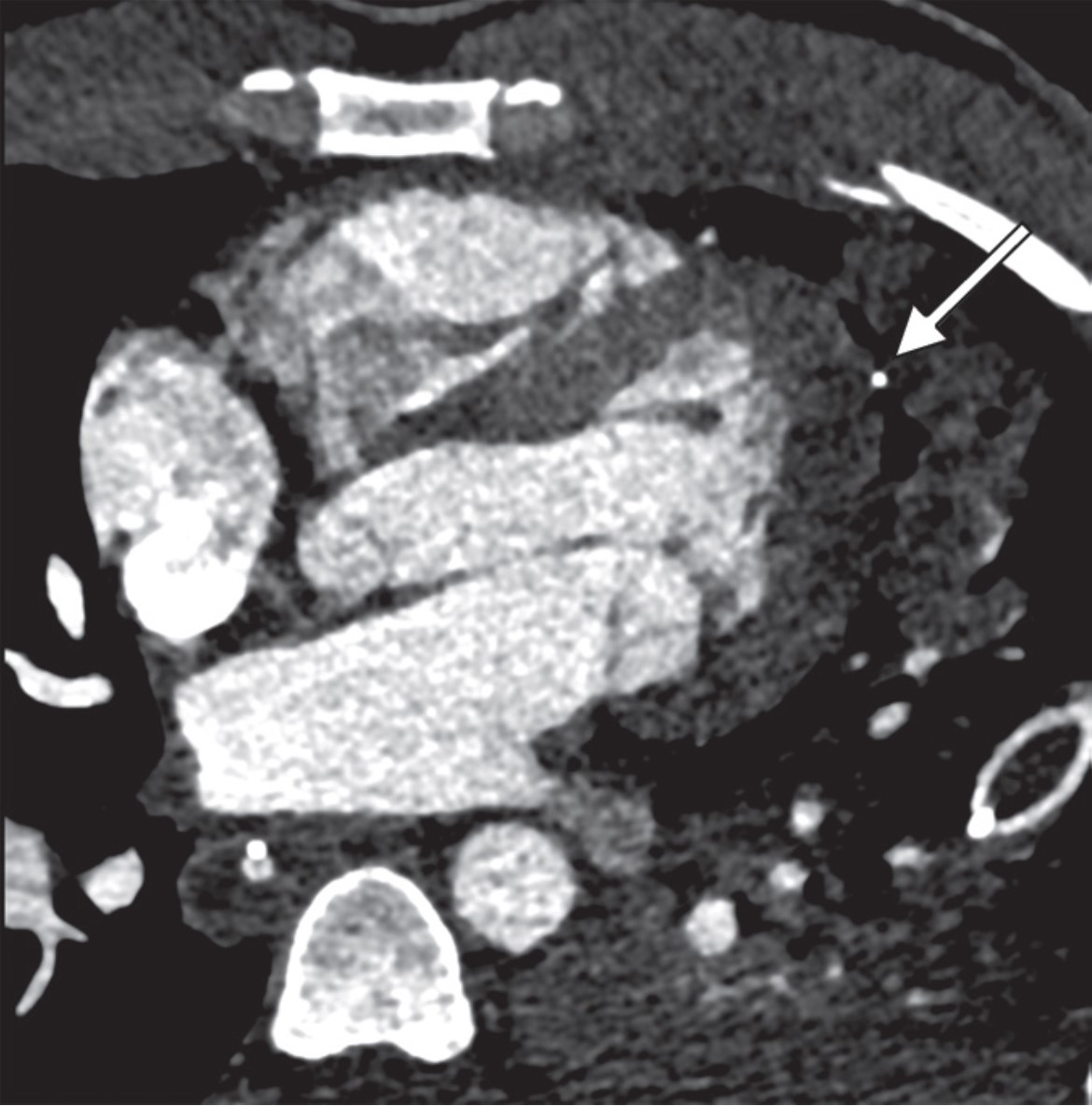
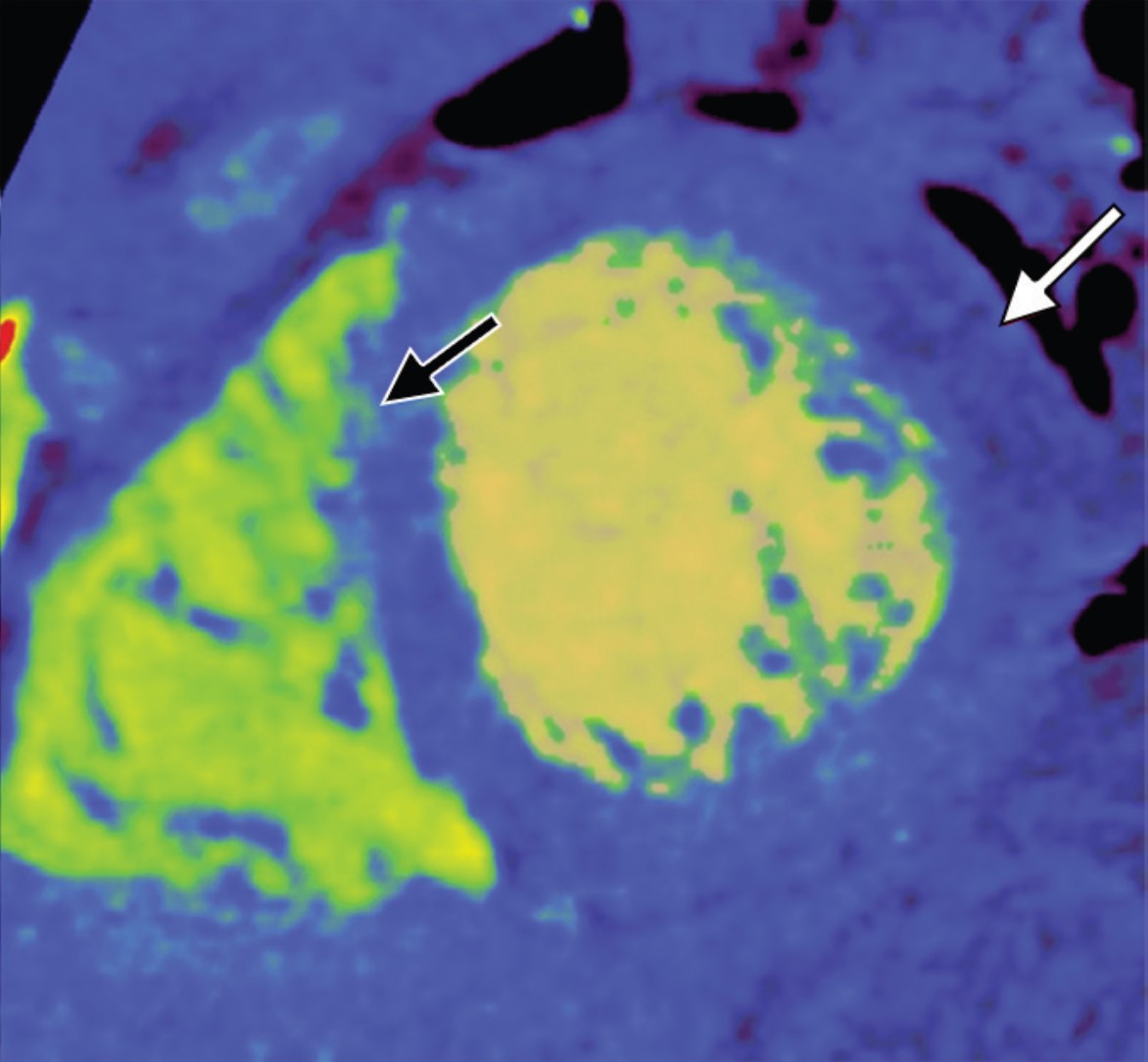
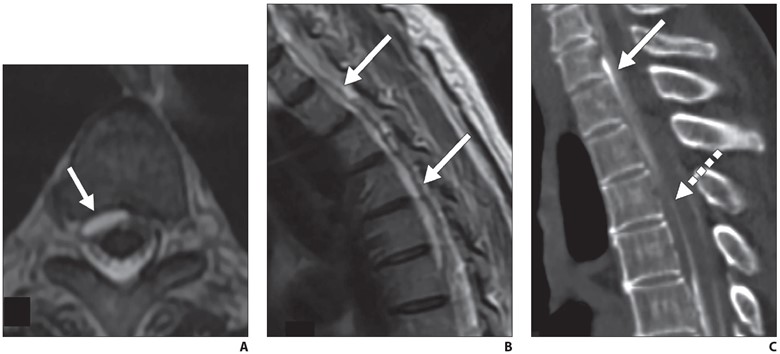
Fig. 2—Awareness barriers to lung cancer screening (LCS). 57-year-old man with limited English-language proficiency who was referred for LCS. He was initially referred for LCS 2 years earlier, at age 55 years old, but he missed that appointment because he did not have additional information resources in other languages about steps to undergo LCS. During annual physical examination 2 years after that initial referral, patient was referred again to LCS. CT images show left upper lobe mass with hilar lymphadenopathy (arrow, Left), surrounding lymphangitic carcinomatosis (Middle), and bony metastasis in sternum (arrow, Right).
At the provider level, unfamiliarity with the new USPSTF and CMS recommendations and identifying patients who are eligible under the new guidelines for LCS are substantial barriers reported in the literature [9–11]. Other barriers at the provider level include unfamiliarity regarding where to refer patients; unfamiliarity with insurance coverage; lack of knowledge about available resources for management of abnormal LCS findings and follow-up of incidental findings; and skepticism about the benefits of LCS, given that clinical trials recruited predominantly White non-Hispanic patients with a higher socioeconomic status than that of the general U.S. population [10].
At the community and health care system level, suboptimal quality of institutional information about LCS (i.e., information not tailored for the surrounding communities) and a lack of institutional social media presence or engagement through social media campaigns to disseminate information about LCS are barriers to LCS [12, 13]. Furthermore, electronic medical records (EMRs) that are not optimized to automatically notify providers of eligible patients have been reported as a barrier [10].
Facilitators
At the individual level, facilitators for LCS are creating patient-centered, culturally tailored educational content to increase interventions to raise awareness and increase health literacy about the new guidelines and fostering non-stigmatizing language and guidelines from national organizations such as the International Association for the Study of Lung Cancer (IASLC) [4, 10, 12, 14]. An effort must be made to inform patients about the importance of early LC detection through LCS, the availability of insurance coverage, and the location of nearby LCS centers using websites such as the “Lung Cancer Screening Locator Tool” [10, 15]. Community health fairs, conventional media, social media, educational brochures, and mailed invitations are examples of how LCS educational information can be disseminated in multiple settings [10]. The educational material can be tailored to focus on hope based on the advancements in LC treatment by including patient testimonials about their experiences with LCS and by tailoring the education to fit the needs and capacities of diverse populations [10, 16]. Online content can provide information and details about LCS programs in multiple languages at the recommended health literacy levels [13]. The Internet and the use of social media can play a key role in the dissemination of information regarding LCS [17]. Prior studies have shown that digital awareness strategies leveraging social media were effective in increasing LCS engagement [17].
At the provider level, unfamiliarity with expanded eligibility criteria and where to refer patients for LCS can be addressed through educational webinars, institutional online resources, and provider-specific educational material that offers continuing medical education credits [18–21]. All these resources will address unfamiliarity with eligibility criteria, skepticism about the benefits of LCS, lack of awareness about LCS insurance coverage, and concerns related to the management of LCS findings [9, 10].
At the community and health care system level, an important facilitator to LCS is updating EMR systems to identify patients who are eligible for LCS under the new guidelines. This information can be incorporated into EMR systems with alerts for eligible high-risk patients, autopopulated referral tools, and lists of certified LCS centers that will help identify eligible patients and promote uptake among diverse patient populations [10, 22]. Online content can facilitate LCS by providing information about LCS programs that is tailored for the local communities served by radiology practices and health care institutions [10, 12]. Furthermore, implementing institutional social media campaigns that emphasize the expanded new eligibility criteria will help overcome knowledge gaps and barriers to awareness [23].
Barriers to and Facilitators of Lung Cancer Screening Opportunities
Barriers
At the individual level, some of the barriers include decreased opportunities to provide accurate smoking history in the EMR, cost concerns related to insurance coverage of LCS and subsequent followups (Fig. 3), challenges to understanding LCS results when examinations show abnormal findings, fragmentation of care for management of abnormal LCS results and incidental findings, and difficulties navigating the complexities of health care systems [4, 8, 10]. Cost transparency and cost concerns are areas of active research, because cost influences how patients access and use health services [2]. For example, a recently published study evaluated the out-of-pocket cost of invasive procedures after LCS and showed that the rates of invasive procedures in commercially insured populations exceed those of invasive procedures in clinical trial participants [2].
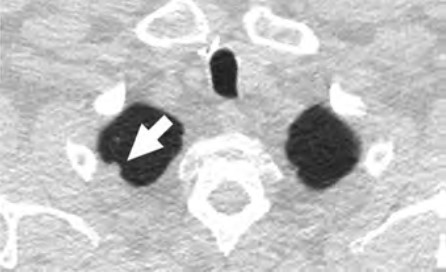
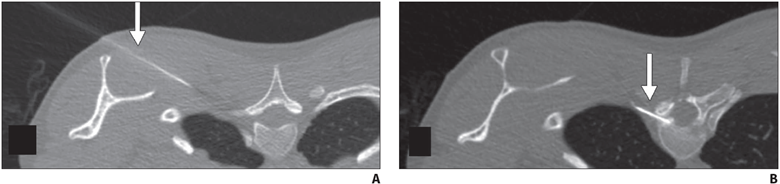
Fig. 3—Insurance barriers to lung cancer screening (LCS) opportunities. Left, CT image of 58-year-old man who initially underwent LCS in 2019 shows right upper lobe lung nodule (arrow) that was interpreted as Lung-RADS 3, and 6-month follow-up was recommended. Before follow-up, patient lost his job and employee-sponsored insurance due to COVID-19 pandemic. LCS follow-up was delayed because patient did not have insurance. Right, Follow-up CT image obtained 2 years later shows interval growth of right upper lobe nodule (arrow), which was biopsy-proven carcinoid.
At the provider level, some of the barriers include difficulty identifying patients who meet eligibility criteria, understanding the influence of comorbidities on the LCS eligibility criteria, and lack of assistance with following up on results [4, 10]. Additional barriers at this level include inconsistent documentation of smoking history, insufficient time to conduct shared decision-making because of other medical responsibilities, difficulty accessing multilingual decision-making aids, and anticipation of patient emotions about participating in LCS [4, 9, 10].
At the community and health care system level, some of the barriers are lack of health insurance coverage for LCS under the new USPSTF guidelines and barriers to telemedicine and broadband Internet access for conducting shared decision-making telehealth encounters. Uncertainty in defining the population-level health data of patients who meet eligibility criteria and would benefit from LCS, the absence of American College of Radiology (ACR)–accredited radiology practices performing LCS in communities, and a lack of community-based strategies to increase participation among underserved communities are additional barriers at this level [4, 5, 8, 10].
Facilitators
At the individual level, facilitators of opportunities for LCS include increasing the opportunities to provide an accurate smoking history through educational campaigns and additional opportunities in other health encounters to capture LCS eligibility information [24]. For identifying LCS-eligible patients, leveraging teachable moment and care coordination strategies during existing routine appointments can be effective. A previous study showed that among women undergoing screening mammography who were given a brief survey to assess LCS eligibility, only a small fraction of LCS-eligible women had undergone LCS [25].
Facilitating care coordination and overcoming transportation barriers can provide additional opportunities for patients to undergo LCS [4, 26]. For example, same-day screening appointments at the time of other medical appointments have been shown to be beneficial to patients who have trouble with transportation, taking time off from work, and finding assistance with dependent care, and this strategy could be expanded to be offered to patients eligible for LCS [27]. Concerns about the costs of LCS can be alleviated by providing information about expected costs related to LCS and by offering information about diverse financial support options provided by institutions. People who are uninsured or have concerns about out-of-pocket expenses related to LCS can be referred to community health care workers and patient navigators who can assist patients in identifying grant funding and institutional financial assistance programs to cover LCS among patients who do not have insurance or have a low income [22, 28]. Health care workers can also assist patients in navigating the complexities of the health care system and clarify additional questions related to their LCS results [22].
At the provider level, LCS can be leveraged as an opportunity to advance early LC detection and tobacco cessation. Primary care providers can benefit from training on shared decision-making encounters for the initial enrollment in LCS to gain further knowledge and expertise about tobacco cessation; the safety of tobacco cessation medications; and additional benefits of LCS with low-dose CT, such as coronary artery calcium scoring and evaluation of emphysema, among others [16, 29]. Prior studies have shown that additional findings such as interstitial lung disease, severe coronary artery disease, thyroid cancer, and renal masses can have clinical implications among patients undergoing LCS [29, 30]. Other facilitators are explaining the LCS results to the patient by identifying and addressing most concerning factors to them and incorporating an assessment in the decision-making process with a patient-centered approach [31]. In addition, creating EMR-based dashboards and alert systems that assist primary care practices in identifying patients who are eligible for LCS, particularly under the updated USPSTF guidelines, will provide additional opportunities for patients and providers to engage in conversations about participating in LCS [10]. Other facilitators can be addressing the importance of consistent documentation of smoking history, multilingual decision aids, and educational workshops or seminars to optimally manage incidental findings and address patient concerns related to undergoing LCS [24].
At the community and health care system level, facilitators of opportunities include the development of system-level policies that combine the updated USPSTF guidelines for LCS and consider social risk factors affecting patients and their communities to promote equitable LCS use and advocacy efforts that increase telehealth and patient portal access by increasing broadband Internet access points and digital patient navigators among underserved communities [5, 7, 10, 12, 17]. Including social risk factors in the calculation used for new LC risk models and LCS eligibility criteria can potentially benefit racial and ethnic minority groups and other underserved patient populations [4]. Increasing access to information about local accredited LCS centers and optimizing EMR systems to identify population-level health data of eligible patients under the new guidelines are additional facilitators to aid in removing these barriers [10, 15, 22].
Barriers to and Facilitators of Lung Cancer Screening Participation
Barriers
At the individual level, barriers to participation include conflicting personal and health schedules, such as medical appointment times that conflict with working hours, dependent care schedules, understanding the importance of adherence to annual LCS and recommended follow-up (Fig. 4) for the detection of early LC, anxiety and stigma about LC diagnosis, concerns about radiation exposure, and access to primary care services to get LCS referrals [4, 9, 10, 26].
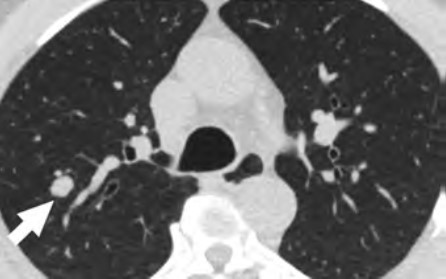
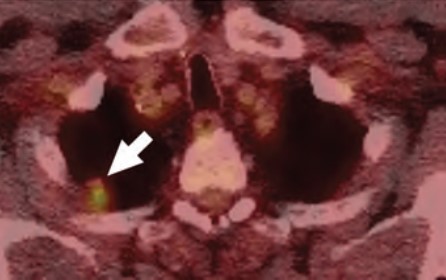
Fig. 4—Knowledge barriers to participation in recommended lung cancer screening (LCS) follow-up. Top Left, CT image of 74-year-old patient who presented for initial LCS in 2018 shows right upper lobe nodule (arrow) that was interpreted as Lung-RADS 2. Top Right, Patient missed annual LCS appointment 1 year after Top Right and returned for LCS 2 years after Top Right. CT image shows interval increase in size of right upper lobe nodule (arrow), which was interpreted as Lung-RADS 4X. Bottom, PET/CT image, also obtained 2 years after Top Right, shows intense uptake within right upper lobe nodule (arrow), which was biopsy-proven lung adenocarcinoma.
At the provider level, barriers to participation include a lack of locally accessible LCS centers or LCS centers outside the health care system that do not offer a streamlined referral and follow-up process, lack of public transportation access to get to appointments, and lack of systemwide patient navigators or health care workers who can aid primary care providers in ensuring patients undergo LCS and help track adherence to recommended follow up of results [4, 10, 26].
At the community and health care system level, barriers include EMR-based LCS appointment reminders that are not available in multiple languages or that are available only through patient portals, decreased availability of system-based dashboards that will alert patients and providers about adherence to follow-up of abnormal LCS examinations, lack of accessible smoking cessation services for patients who smoke, and lack of access to multidisciplinary lung nodule clinics to assist patients in management of abnormal LCS findings [4, 10, 32].
Facilitators
At the individual level, facilitators of participation for LCS include providing schedule flexibility by offering off-hours appointments during weekends and evenings or collaborating with community organizations to offer resources and promote screening during social events in the communities [28, 33]. Providing transportation to LCS appointments, such as ride sharing or cab vouchers, or providing access to mobile LCS units can assist patients in overcoming transportation barriers that could lead to missed LCS appointments [10]. To improve participation, providers can collaborate with radiology practices in communicating the importance of LCS and can promote follow-up through reminders sent to patients, which have been shown to increase LCS adherence [34]. The ACR National Lung Cancer Roundtable (NLCRT) launched a campaign to decrease the stigma associated with a LC diagnosis and decrease concerns about radiation exposure [35–37]. Increasing access to LCS clinics that offer an integrated approach to LCS in collaboration with primary care practitioners can assist in overcoming barriers related to a lack of access to primary care practitioners [38, 39].
At the provider level, facilitators include increasing the availability of community health care workers and patient navigators who can aid primary care practices to assist patients in participating in LCS [40].
Patient navigators can assist primary care providers in conducting shared decision-making, identifying and confirming LCS eligibility of patients, and assisting patients in clarifying additional steps or concerns needed to engage in LCS [40]. Collaboration between radiology and primary care practices can lead to offering integrated LCS programs that have streamlined referral pathways for LCS independent of practice location [38, 39]. In addition, LCS radiology programs that collaborate with primary care providers and community organizations to offer LCS, smoking cessation services, and screening for other cancers can be opportunities to increase participation in LCS and meet other population health preventive service goals [41, 42].
At the community and health care system level, facilitators of opportunities include EMR-based LCS appointment reminders available in multiple languages and through additional services other than patient portals, updating population-level health dashboard alerts of patients who are eligible or overdue for LCS under the new USPSTF guidelines, and creating system-based alerts to notify providers about newly eligible patients [10, 34]. Studies that have evaluated LCS adherence rates, patient characteristics associated with adherence, and diagnostic testing rates after screening revealed that underrepresented racial/ethnic minority populations and individuals who currently smoke are less likely to remain in the program [32]. Patients who undergo LCS and are currently smoking can benefit from the integration of smoking cessation counseling services into part of their LCS encounters, and participation in LCS increases adherence to a smoking cessation program [43]. Interventions that combine promoting participation in LCS and connecting patients who are current smokers with an evidence-based intervention composed of a web-based program and text messaging, are examples of a coordinated approach that increases participation in both LCS and smoking cessation [43, 44]. Finally, for assisting patients who have abnormal LCS results, improving telehealth access, increasing the capacity of smoking cessation services, and implementing a tailored approach with multidisciplinary lung nodule clinics for the management of abnormal LCS results and EMR dashboards that automatically track adherence to follow-up and outcomes can provide a system-based care coordination that will aid these patients in accessing LC care [38, 45–47].
To advance equitable participation in LCS and achieve the population health goal of improving LC outcomes for all patients through early detection, it is paramount that multilevel interventions are tailored to fit the needs and capacities of diverse patient populations served by all types of community practices. To achieve this goal, transdisciplinary system-based programs and interventions are key to address systemic barriers, improve access and uptake of LCS, and improve LC outcomes primarily among underserved patient populations. As radiologists and promoters of the health and well-being of our patients, partnering with patients, community organizations, and other medical specialties to assist patients in overcoming multilevel barriers to LCS will allow us to design sustainable programs to promote awareness of, opportunities for, and participation in LCS for all patients.
References
NIH website. SEER Program. Cancer stat facts: lung and bronchus cancer. seer.cancer.gov/statfacts/html/lungb.html. Published 2021. Accessed November 12, 2023
Febbo J, Little B, Fischl-Lanzoni N, et al. Analysis of out-of-pocket cost of lung cancer screening for uninsured patients among ACR-accredited imaging centers. J Am Coll Radiol 2020; 17:1108–1115
Wang GX, Pizzi BT, Miles RC, et al. Implementation and utilization of a “pink card” walk-in screening mammography program integrated with physician visits. J Am Coll Radiol 2020; 17:1602–1608
Flores EJ, Irwin KE, Park ER, Carlos RC. Increasing lung screening in the Latino community. J Am Coll Radiol 2021; 18:633–636
Doubeni CA, Simon M, Krist AH. Addressing systemic racism through clinical preventive service recommendations from the US Preventive Services Task Force. JAMA 2021; 325:627–628
Van Haren RM, Delman AM, Turner KM, et al. Impact of the COVID-19 pandemic on lung cancer screening program and subsequent lung cancer. J Am Coll Surg 2021; 232:600–605
U.S. Preventive Services Task Force. Final recommendation statement: lung cancer—screening. www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung-cancer-screening. Published March 9, 2021. Accessed November 12, 2023
Ford JG, Howerton MW, Lai GY, et al. Barriers to recruiting underrepresented populations to cancer clinical trials: a systematic review. Cancer 2008; 112:228–242
Trauth JM, Jernigan JC, Siminoff LA, Musa D, Neal-Ferguson D, Weissfeld J. Factors affecting older African American women’s decisions to join the PLCO Cancer Screening Trial. J Clin Oncol 2005; 23:8730–8738
Wang GX, Baggett TP, Pandharipande PV, et al. Barriers to lung cancer screening engagement from the patient and provider perspective. Radiology 2019; 290:278–287
Wang GX, Neil JM, Fintelmann FJ, Little BP, Narayan AK, Flores EJ. Guideline-discordant lung cancer screening: emerging demand and provided indications. J Am Coll Radiol 2021; 18:395–405
Coughlin JM, Zang Y, Terranella S, et al. Understanding barriers to lung cancer screening in primary care. J Thorac Dis 2020; 12:2536–2544
Gagne SM, Fintelmann FJ, Flores EJ, et al. Evaluation of the informational content and readability of US lung cancer screening program websites. JAMA Netw Open 2020; 3:e1920431
International Association for the Study of Lung Cancer (IASLC) website. IASLC language guide. www.iaslc.org/IASLCLanguageGuide. Published May 2021. Accessed November 12, 2023
American College of Radiology (ACR) website. Lung cancer screening locator tool: screening location finder. www.acr.org/Clinical-Resources/Lung-Cancer-Screening-Resources/LCS-Locator-Tool. Published 2021. Accessed November 12, 2023
Flores EJ, Neil JM, Tiersma KM, et al. Feasibility and acceptability of a collaborative lung cancer screening educational intervention tailored for individuals with serious mental illness. J Am Coll Radiol 2021; 18:1624–1634
Jessup DL, Glover Iv M, Daye D, et al. Implementation of digital awareness strategies to engage patients and providers in a lung cancer screening program: retrospective study. J Med Internet Res 2018; 20:e52
American College of Radiology (ACR) website. Lung cancer screening resources. www.acr.org/Clinical-Resources/Lung-Cancer-Screening-Resources. Accessed October 7, 2021. Accessed November 12, 2023
American College of Radiology (ACR) website. Lung CT Screening Reporting & Data System (Lung-RADS). www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Lung-Rads. Published 2021. Accessed November 12, 2023
LuCa National Training Network website. Enhancing provider education on lung cancer care. lucatraining.org. Published 2021. Accessed November 12, 2023
American College of Radiology (ACR) website. National lung cancer roundtable lung cancer screening webinar series. pages.acr.org/2021-NLCRT-Webinar-Series.html. Published 2021. Accessed November 12, 2023
Percac-Lima S, Ashburner JM, Rigotti NA, et al. Patient navigation for lung cancer screening among current smokers in community health centers a randomized controlled trial. Cancer Med 2018; 7:894–902
Wang GX, Narayan AK, Park ER, Lehman CD, Gorenstein JT, Flores EJ. Screening mammography visits as opportunities to engage smokers with tobacco cessation services and lung cancer screening. J Am Coll Radiol 2020; 17:606–612
Cardarelli R, Roper KL, Cardarelli K, et al. Identifying community perspectives for a lung cancer screening awareness campaign in Appalachia Kentucky: the Terminate Lung Cancer (TLC) study. J Cancer Educ 2017; 32:125–134
Lopez DB, Flores EJ, Miles RC, et al. Assessing eligibility for lung cancer screening among women undergoing screening mammography: cross-sectional survey results from the National Health Interview Survey. J Am Coll Radiol 2019; 16:1433–1439
Bieniasz ME, Underwood D, Bailey J, Ruffin MT 4th. Women’s feedback on a chemopreventive trial for cervical dysplasia. Appl Nurs Res 2003; 16:22–28
Healio website. ‘I’ve never been treated so well’: same-day cancer screening program helps reduce barriers. www.healio.com/news/hematology-oncology/20210907/ive-never-been-treated-so-well-sameday-cancer-screening-program-helps-reduce-barriers. Published September 7, 2021. Accessed November 12, 2023
CancerCare website. Financial assistance program. www.cancercare.org/financial. Published 2021. Accessed November 12, 2023
Fan L, Fan K. Lung cancer screening CT-based coronary artery calcification in predicting cardiovascular events: a systematic review and meta-analysis. Medicine (Baltimore) 2018; 97:e10461
Hatabu H, Hunninghake GM, Richeldi L, et al. Interstitial lung abnormalities detected incidentally on CT: a Position Paper from the Fleischner Society. Lancet Respir Med 2020; 8:726–737
Schapira MM, Aggarwal C, Akers S, et al. How patients view lung cancer screening. the role of uncertainty in medical decision making. Ann Am Thorac Soc 2016; 13:1969–1976
Barbosa EJM Jr, Yang R, Hershman M. Real-world lung cancer CT screening performance, smoking behavior, and adherence to recommendations: Lung-RADS category and smoking status predict adherence. AJR 2021; 216:919–926
CDC website. Offering flexible hours and locations. www.cdc.gov/cancer/nbccedp/success/hours-locations.htm. Published 2021. Accessed November 12, 2023
Hirsch EA, New ML, Brown SP, Baron AE, Malkoski SP. Patient reminders and longitudinal adherence to lung cancer screening in an academic setting. Ann Am Thorac Soc 2019; 16:1329–1332
American Thoracic Society (ATS) website. American Thoracic Society and American Lung Association implementation guide for lung cancer screening. www.lungcancerscreeningguide.org. Accessed November 12, 2023
International Association for the Study of Lung Cancer (IASLC) website. Feldman J, Faris NR, Warren GW. Ending stigma in lung cancer: the IASLC participates in a collaborative summit held by the National Lung Cancer Roundtable. www.iaslc.org/iaslc-news/ilcn/ending-stigma-lung-cancer-iaslc-participates-collaborative-summit-held-national. Published October 15, 2020. Accessed November 12, 2023
Christiani DC. Radiation risk from lung cancer screening. Chest 2014; 145:439–440
Okpala P. Increasing access to primary health care through distributed leadership. Int J Healthc Manag 2021; 14:914–919
Joseph AM, Rothman AJ, Almirall D, et al. Lung cancer screening and smoking cessation clinical trials: SCALE (Smoking Cessation within the Context of Lung Cancer Screening) Collaboration. Am J Respir Crit Care Med 2018; 197:172–182
Denver Health website. Module 3: healthcare team—community health workers and patient navigators. https://www.denverhealth.org/patients-visitors/community-voices-patient-navigators. Published 2011. Accessed November 12, 2023
Headrick JR, Morin O, Miller AD, Hill L, Smith J. Mobile lung screening: should we all get on the bus? Ann Thorac Surg 2020; 110:1147–1152
Atrium Health website. Levine Cancer Institute launches nation’s first mobile lung CT unit to improve care for region’s underserved and rural patient. atriumhealth.org/about-us/newsroom/news/2017/03/levine-cancer-institute-launches-nations-first-mobile-lung-ct-unit-to-improve-care-for-regions-unde. Published March 20, 2017. Accessed November 12, 2023
Lococo F, Cardillo G, Veronesi G. Does a lung cancer screening program promote smoking cessation? Thorax 2017; 72:870–871
Graham AL, Burke MV, Jacobs MA, et al. An integrated digital/clinical approach to smoking cessation in lung cancer screening: study protocol for a randomized controlled trial. Trials 2017; 18:568
Massachusetts General Hospital website. Pulmonary nodule clinic. www.massgeneral.org/cancer-center/treatments-and-services/pulmonary-nodule-clinic. Published 2021. Accessed November 12, 2023
MD Anderson Cancer Center website. Lung cancer screening clinic. www.mdanderson.org/patients-family/diagnosis-treatment/care-centers-clinics/cancer-prevention-center/lung-screening-clinic.html. Published 2021. Accessed November 12, 2023
American College of Radiology (ACR) website. ACR designated lung cancer screening center. www.acraccreditation.org/centers-of-excellence/lung-cancer-screening-center. Published 2021. Accessed November 12, 2023
What does the general public hear about lung cancer screening (LCS) from newspapers here in the United States of America? And why does what the public hears about LCS in the papers matter? Mass media is an important source of medical information for the public at large. Print sources, radio, television, online, and social media platforms all influence public knowledge of medical topics, but especially so for older adult populations, print media remains a truly trusted resource [1].
Public perception of LCS is particularly critical, since eligible individuals may not be aware of LCS opportunities, as well as the benefits and risks of screening with low-dose CT (LDCT). In-office discussion is often limited by time constraints; in a JAMA study from 2018, practitioners spent, on average, less than 1 minute discussing LCS [2]. According to findings from the U.S. National Lung Screening Trial, LCS with LDCT was associated with a 20% reduction in lung cancer-specific mortality [3], yet despite so many additional trials providing further support, LCS uptake continues to represent too small a fraction of the eligible population. Could the composition of coverage concerning LCS help to shape public understanding and influence the opinions of those eligible for LDCT screening?
For AJR, my colleagues and I analyzed 12 years’ worth of LCS coverage in U.S. newspapers to assess the volume, tenor, and scope of that coverage [4]. The good news? Most of the coverage, itself, was good. And in could-be-better news, although many articles mentioned at least one benefit of LDCT LCS, additional important benefits were uncommonly included. The worst news, though? Critical logistics were seldom mentioned, and radiologists were infrequently interviewed.
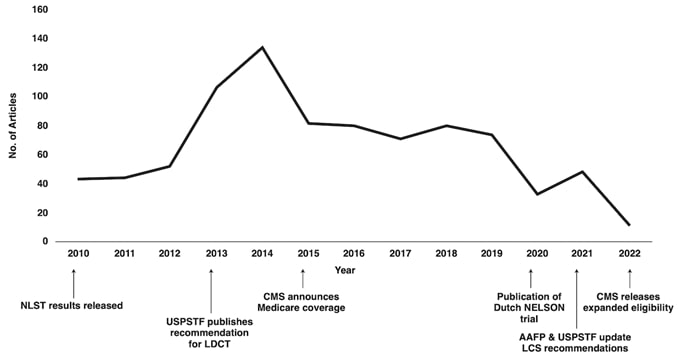
From 2010 to 2022, a total of 859 articles mentioning LCS were included across a range of local, regional, and national newspaper sources. Weekly circulation sizes ranged from a low of 713 readers for one local paper to 1.2 million for the New York Times and 1.5 million for the Wall Street Journal. Annual article volume ranged from a high of 130 in 2014 (15% of the total) to a low of 33 (4% of the total) in 2020. Unfortunately for data, 2022 proved to be an incomplete year (Fig. 1).
Fig. 1—Line graph depicting number of U.S. newspaper articles covering LCS by year of publication, 2010–2022. Key developments in lung cancer screening are annotated by year. Study period included only first 3 months of 2022, resulting in lower number of articles for that year. LCS = lung cancer screening. NLST = National Lung Screening Trial, USPSTF = U.S. Preventive Services Task Force, LDCT = low-dose CT, AAFP = American Academy of Family Physicians.
The nadir of LCS coverage in 2020 coincided with the onset of the novel coronavirus disease (COVID-19) pandemic. Understandably, COVID-19 dominated the news that year, comprising about 25% of frontpage news articles for 2020 [5].
Of all articles, 25% were published during the month of November, Lung Cancer Awareness Month. It is gratifying to see LCS information so well disseminated during this month of greater public awareness, but such clustering reminds us: more sustained coverage throughout the year might be beneficial.
For a majority of articles, 76%, sentiment towards LCS was positive; moreover, negative sentiment comprised just 3% of the total. However, a higher proportion of negative sentiment (8%) came from articles on the highest quartile of weekly circulation (i.e., the most widely read newspapers).
Full articles appeared most commonly (65%), but short news briefs—often a small paragraph within a collection of multiple news items—accounted for a large proportion of the total article number (31%). Typically, these news briefs were limited in scope (e.g., an announcement for a screening program).
Most articles (64%) mentioned at least one benefit of LCS: early detection and mortality reduction (49%). (Meanwhile, other benefits, such as the ease of LDCT or low radiation dosage, were rarely stated.) And we found it was a minority of articles (23%) that mentioned at least one potential risk.
Logistical aspects of LCS were infrequently stated, including updated recommendations for an annual CT examination until eligibility criteria are no longer satisfied (27%) and participation in a smoking cessation program (28%).
Although many eligible individuals had questions regarding the potential cost or insurance coverage of LDCT LCS, we found it was a minority of articles (33%) that broached these subjects.
Importantly, despite playing a leading role in LCS programs, radiologists were mentioned or interviewed in a minority of articles (9%). Low media representation may be a missed opportunity to illustrate the importance of radiologists—and the field of imaging—to early cancer detection and management.
Brenner AT, Malo TL, Margolis M et al. Evaluating shared decision making for lung cancer screening. JAMA Intern Med 2018; 178:1311–1316
National Lung Screening Trial. U.S. Department of Health and Human Services’ National Institute of Health, National Cancer Institute website. www.cancer.gov/types/lung/research/nlst. Accessed October 19, 2023
Zippi ZD, Cortopassi IO, Johnson EM et al. U.S. newspaper coverage of lung cancer screening from 2010 to 2022. AJR 2023; 221
Krawczyk K, Chelkowski T, Laydon DJ. Quantifying online news media coverage of the COVID-19 pandemic: text mining study and resource. J Med Internet Res 2021; 23:e28253
The American Roentgen Ray Society (ARRS) is pleased to announce Francis Baffour of Mayo Clinic in Rochester, MN, as the 2024 Melvin M. Figley Fellow in Radiology Journalism. ARRS also recognizes Hyun Soo Ko of the Peter MacCallum Cancer Centre and Epworth Medical Imaging in Melbourne, Australia, as the 2024 Lee F. Rogers International Fellow in Radiology Journalism.
Supported by The Roentgen Fund® and named for two distinguished Editors Emeriti of ARRS’ own American Journal of Roentgenology (AJR), the Melvin Figley and Lee Rogers Fellowships offer practicing radiologists an unparalleled opportunity to learn the tenets of medical publishing via “the yellow journal”—the world’s longest continuously published radiology journal. Through hands-on experience with ARRS staff and AJR personnel—as well as personal apprenticeship with AJR’s 13th Editor of Chief, Andrew B. Rosenkrantz—Drs. Baffour and Ko will receive expert instruction in scientific writing and communication, manuscript preparation and editing, peer review processes, journalism ethics, and both print production and digital publication.
Founded in 1907, AJR is one of the specialty’s leading peer-reviewed journals, publishing clinically oriented content across all imaging subspecialties and modalities relevant to radiologists’ daily practice. Overall, “the yellow journal” garnered 35,480 citations in 2022, ranking AJR fourth among all radiology journals.
Since 1990, The Roentgen Fund has granted millions of dollars to hundreds of imaging professionals for both research pursuits and professional development. Today, through six vital scholarship and fellowship programs, the generosity of The Roentgen Fund’s donors is channeled to every corner of the globe—establishing dual foundations in innovation and leadership for a true diversity of radiology’s next generation.
Francis Baffour practices as a diagnostic radiologist with expertise in advanced MRI and CT techniques for musculoskeletal imaging. His clinical and research interests align with his goal of identifying novel applications for advanced imaging technologies, then rapidly translating these discoveries into practical patient care. As associate medical director of the CT Clinical Innovation Center in Mayo Clinic Rochester’s department of radiology, he supports the mission of facilitating high-impact imaging innovations with direct effect on patients, such as radiation dose reduction techniques, novel CT technologies, and quantitative assessment of disease activity. Dr. Baffour earned his M.D. from the Albert Einstein College of Medicine in New York City and a B.A. in biochemistry from Vassar College in Poughkeepsie, NY.
A German and Australian board-certified radiologist with over 20 years of international experience, currently, Hyun Soo Ko practices at Peter MacCallum Cancer Centre and Epworth Medical Imaging in Melbourne, Australia, holding affiliations with the University of Melbourne and University of Bonn in Germany. Her expertise is diverse, with specialized fellowships in breast imaging (Melbourne), imaging research (Toronto), and pediatric radiology (Heidelberg, Germany). Dedicated to advancing translational medicine, her research focuses on AI and radiomics to discover predictive imaging biomarkers. She is an active member of the Royal Australian and New Zealand College of Radiologists (RANZCR) Advisory Committee on Artificial Intelligence and the German Roentgen Society (DRG) Working Party Methodology and Research. As a clinician researcher, Dr. Ko remains committed to mentoring and supporting emerging radiologists, firmly believing multidisciplinarity and inclusiveness are key elements for equitable progress and impact.
From May 5–9, 2024, Drs. Baffour and Ko will attend the 2024 ARRS Annual Meeting in Boston, MA, where they will co-present the AJR Year in Review Sunday Session and participate in the Editor’s Forum.
More about the Figley and Rogers Fellowships
Melvin M. Figley (1920-2010) assumed the editorial mantle of AJR with the January 1976 issue. Hiring a full-time professional staff and, for the first time, a managing editor, he appointed associate editors to facilitate the peer review process. Publication accelerated, and the quality of illustrations improved, leading to the AJR Pictorial Essay. Dr. Figley was also central to the partnership between ARRS and the American Society of Neuroradiology, including the founding of the American Journal of Neuroradiology in 1980. After more than a decade of dedicated service to “the yellow journal,” Dr. Figley retired in 1985.
Lee F. Rogers, the distinguished musculoskeletal radiologist and longtime chair of imaging at Northwestern University Medical School, was named AJR’s chief editorial officer in 1996. Highlights from Rogers’ tenure at the journal included more contemporary design, introducing of a medicolegal column, authored by Dr. Leonard Berlin, and his popular editor’s notebook. Both the quality and the variety of papers published in AJR remained quite high, as the information revolution propelled “the yellow journal” into new formats, such as CD-ROM, and frontiers, like the internet.
Five prior Melvin M. Figley Fellows of The Roentgen Fund® will also present during the 124th ARRS Annual Meeting in Boston, MA:
In radiology, whether you work in a large or small private practice, remotely by yourself, an academic department in a medical center, or part of a mega radiology practice, there has been a palpable shortage of radiologists. This shortage is fueled by a trend toward exclusive subspecialization with declining numbers of radiologists who can handle general work, ever-increasing expectations for service to our patients, referring doctors, hospitals, and health care systems. We have been stretched thinner. There is a desire by radiologists to have more flexible work hours or, simply stated, to work less hours overall compared to years past. There is a concern about what role artificial intelligence and machine learning will play; will we be displaced? Reimbursement has been decreasing relative to inflation and compared with other specialties. As a result of these realities and others, there is clear evidence of burnout among radiologists, similar to health care workers in other specialties. On top of that, sometimes, we find that the leaders in our organizations may be distant, or too corporate, or suffer from “toxic positivity,” which may be worse than “toxic negativity.”
There has been a steady headwind for years, but it now feels like a gale force wind. And a lot of this feels out of our control. So, goodness, how do we manage all of this? Hold on, let’s take a breath. One strategy that we can embrace and control is to develop a culture of teams within our workplaces. In fact, I have titled this series “The Teamwork Imperative” because we must establish teamwork as a core value within the radiology workforce. I believe that if we foster a culture of teams, we can mitigate and shield ourselves from some of these headwinds.
Let me be clear. Here, when I say teams, I am specifically not referring to the “macro teams” that many of us find ourselves in. For example, at Duke Health, it is said that the 30,000-plus employees are my “teammates.” That very well may be true. But no, I am referring to your local and focal team. I am referring to the individuals that you rely on daily or weekly to deliver your work product. It’s the folks you huddle with. And the teams develop where you huddle. If you are in training, I am referring to your team of co-residents, your chief residents, maybe your program director or program coordinator who you lean on. If you are in a private practice, I am referring to those that you share physical space with, or perhaps switch call with, or the individuals you show difficult cases to, or the referring docs you have developed close relationships with, and who rely on you to deliver care. In an academic environment like mine, it might be the members of your subspecialty division. If done well, the division pulls together as a team to deliver care, service, teaching, and research.
Those divisions that have a culture of team are far more effective than those who are unable to act as a team. If you are lucky enough to have these local and focal teams (and these often form and evolve organically), many challenges at work open up and become more manageable and attainable. The clouds begin to lift. Specifically, your deliverables, whatever they may be, are far more easily and effectively achieved if you have your team and approach your work from the perspective of that team.
Work becomes more efficient and fulfilling and, frankly, more fun. The work becomes more manageable, with more aspects under your control. You become more engaged. And that then becomes an antidote to burnout. Teams, therefore, contribute to retention.
Coaches discuss this all the time. I’ll borrow here from Mike Krzyzewski, the legendary Duke University men’s basketball coach. “Coach K” famously talked about the five keys to an effective team, likening them to the fingers on a hand. Each finger is individual and can stand alone, but when the five fingers of communication, trust, responsibility, caring, and productivity come together into a fist, the fist proves to be much stronger than the sum of the individual fingers.
Communication
Yes, of course, communication is about sharing news back and forth, accurately and honestly, but more importantly, communication is to be able to probe, to be able to respectfully question, and to be able to expect honest answers from your teammates. Sometimes, the questions aren’t easy, and the answers may not be easy either. To foster an effective team requires the ability and the safety of pointing out the opportunities—those ones are easy. More importantly, it is to have safety in pointing out deficiencies—those are more difficult. It is critical for teammates to be able to receive and internalize the information coming from within the group, whether it is a kudo, an observation, or a deficiency or a criticism.
You have to talk to each other. Actually talk. And in a world of remote work and texting, we don’t talk enough. Maybe the talking occurs in a partner meeting, defined clinical case conference, resident meeting, or division or department meeting. Maybe it is your team taking a coffee break or going for a midday walk to achieve “step” goals. Hopefully, the team dynamics are such that one can tap a teammate on the shoulder and engage in an effective and safe conversation.
Communication needs to be practiced. That is why I think standing, regular, in-person meetings, even if the agenda is light, are very important. The opportunity to come together regularly promotes the importance and expectation of communication. And it is habit forming. You get better at it.
Trust
Trust means telling the truth, and telling it sooner rather than later; knowing that within a team, that can be hard. It can be hard because so many of us struggle with confrontation and conflict and try to avoid them. But consider it this way, from the perspective of the iconic University of Tennessee women’s basketball coach, Pat Summitt. She said, “The absolute heart of loyalty is to value those people who tell you the truth, not just those people who tell you what you want to hear. In fact, you should value them the most, because they have paid you the compliment of leveling with you, assuming you can handle it.”
Honest and fair difficult conversations almost always produce results. If you can get through the first thirty seconds of a difficult conversation, often the clouds lift and a very productive conversation follows. For me, I need to write down the key first few sentences for that opening thirty seconds and the rest flows. If difficult conversations don’t produce results, you have learned something.
Collective Responsibility
A coach might say, “We win together, we lose together, there is no “blame game.” In the workplace of radiology, the collective responsibility is the pulling together to deliver on our various missions. Everyone does not play the same role. One partner may be a fast and efficient reader, that’s great. Her partner is slower because he spends a lot more time consulting and discussing with referring docs. Both these individuals are important to the team. Or in an academic environment, one may be more focused and skilled clinically, another may be more focused on teaching. In a team where there is collective responsibility, they complement one another and each can be proud of each other’s successes. Indeed, the light of their success shines on the other teammates, on the entire team.
Caring
This is also about humanity and human connections and colleagueship. Caring in a team reflects time spent with each other and sharing aspects of ourselves, in this case the women of Duke Radiology. The caring strengthens the interconnective web between team members, in this case at our annual Fall Gathering. It makes the team softer in a positive way, and more personable, yet, at the same time stronger.
Here is where I worry about remote work. I get it. The pandemic has shown that we can do radiology effectively, even remotely. People like it and expect it. And we have learned that we can teach remotely. Sort of. But it seems far more difficult to foster a genuine, caring environment when work is dispersed in many geographic locales and individuals work essentially independently, free of meaningful, direct interactions with other teammates, other humans. To me the same applies to Zoom meetings. All the nuanced talk and greetings pre- and post-meeting are lost. The body language is lost. The sense of community is lost, or at least different. And I think the effectiveness of the meeting suffers. Indeed, on a Zoom meeting, you can’t even have real eye contact. I worry that with remote work, the culture of our teams maybe eroded. We do need to incorporate the best aspects of some remote work, but incorporate it in a fashion that fosters caring.
Pride/Productivity
Coach K says, “Everything we do has our own personal signature on it…and if we all sign off on everything we do, then we have a chance to be great.”
And your teammates all do have the chance to add their personal touch and signature. Collectively then, we have the opportunity to harness the best of what we can be, and to be great, even with all that is facing us and challenging us in our current and future work environments. “And it is going to be hard; we all wait in life for things to get easier…when we are well staffed, when I pass the Boards, when I make partner, when the kids are older, when the pandemic is over … it will never get easier. What happens is, you handle hard better.” As pointed out by Kara Lawson, Duke women’s basketball coach.
Each of these domains, communication, trust, collective responsibility, caring, and pride; the five individual fingers are important. But when the five fingers are formed into a fist, a true team, the collective strength is much greater than the sum of the individual parts. When these five areas can be applied to our teams in radiology, we can become more effective and efficient. As individuals alone, we are relatively weak. Together as a team, we are stronger. And this is something within our control.
To me, there is an imperative to create, sustain, and grow teams in our workplace.
Colleagues, I personally invite you to join us for ARRS 2024, either in Boston or online. This exceptional event brings together top radiologists from around the world to share new knowledge shaping our field.
Our Annual Meeting is renowned for its cutting-edge education, providing clinical information you can put into practice right away. We are excited to share the latest advancements in radiology, along with comprehensive review lectures to stay sharp on core topics.
Whether you attend in person and immerse yourself in the vibrant atmosphere of Boston, or choose our convenient online option, ARRS 2024 promises to be a remarkable experience. Your participation and engagement will help us connect, learn, and advance radiology together.
Department of Radiology and Biomedical Imaging University of California, San Francisco
Brett M. Elicker
Department of Radiology and Biomedical Imaging University of California, San Francisco
The diagnosis of interstitial lung disease (ILD) involves multidisciplinary collaboration among radiology, pulmonary medicine, rheumatology, and anatomic pathology disciplines. Imaging findings play a major role in the diagnosis of a variety of diffuse lung diseases, and the radiologist’s input into the ultimate diagnosis is often substantial [1]. Imaging is of critical importance in the diagnosis of ILD, although the accurate interpretation of characteristic high-resolution CT (HRCT) findings can be challenging. This InPractice article will review common pitfalls for those tasked with interpretation of CT in the diagnosis of ILD with a focus on avoiding common errors, identifying distinguishing features of specific diagnoses, and recognizing entities with which CT has limited sensitivity.
Overdiagnosis of Usual Interstitial Pneumonia Pattern
The goals of the radiologist in the evaluation of a patient with suspected pulmonary fibrosis are to determine whether a diffuse lung disease is present, determine the pattern of fibrosis, and provide an appropriate differential diagnosis. Usual interstitial pneumonia (UIP) pattern of pulmonary fibrosis is the most common ILD. UIP is most frequently idiopathic, but can also be secondary to connective tissue disease, medications, or exposure to asbestos [2]. Given the pervasiveness of this diagnosis, radiologists participating in the multidisciplinary diagnosis of patients with suspected ILD are frequently asked whether CT findings support a UIP diagnosis.Fortunately, guidelines can increase the confidence of radiologists in correctly identifying patients with UIP. The American Thoracic Society guidelines for the diagnosis of UIP pattern break down CT findings into four categories: UIP, probable UIP, indeterminate for UIP, and alternative diagnosis. The CT findings indicative of UIP pattern include subpleural and basal predominant fibrosis in addition to honeycombing, with or without traction bronchiectasis (Fig. 1).
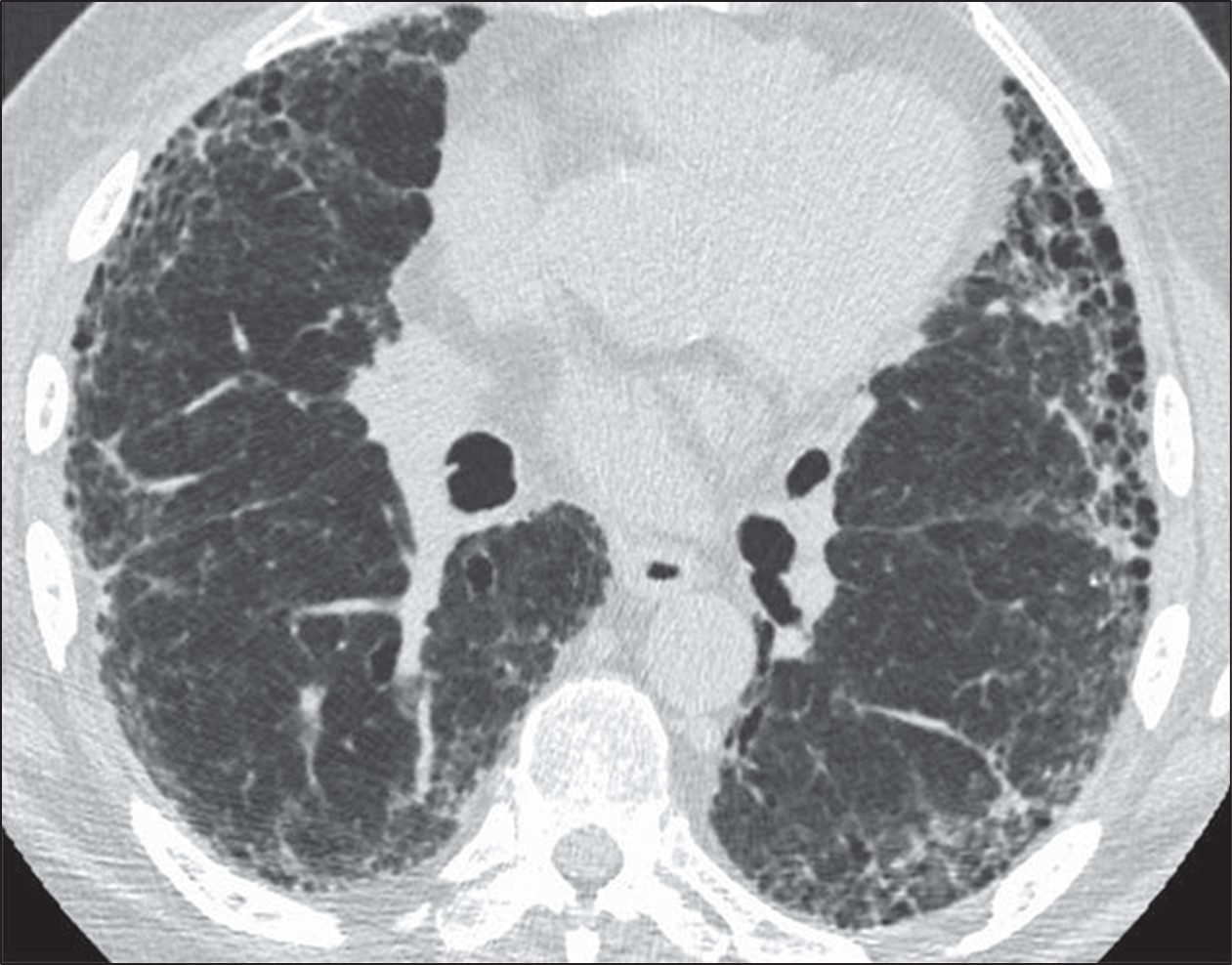
Fig. 1—73-year-old man with idiopathic pulmonary fibrosis. HRCT scan shows usual interstitial pneumonia pattern of fibrosis characterized by subpleural and basal distribution of fibrosis with honeycombing.
This is to be distinguished from the probable UIP pattern, which is characterized by the same distribution of fibrosis including reticulation and traction bronchiectasis, but the absence of honeycombing [3].
The PPV of UIP pattern on CT for histologic UIP at surgical lung biopsy exceeds 90%, and as such, surgical lung biopsy is rarely performed when a confident diagnosis of UIP pattern can be made from imaging [3, 4]. For this reason, a diagnosis of UIP should only be made when the radiologist is confident that the imaging findings are consistent with this pattern, because often further diagnostic testing will not be pursued, potentially depriving the patient of the opportunity to receive the correct diagnosis. This distinction is not trivial; those diagnosed with UIP may be treated with antifibrotic medications and thus be subject to the side effects thereof. Not surprisingly, patients treated with antifibrotics for UIP will not be given immunosuppressive therapy, which could be a more appropriate treatment in the setting of another histologic diagnosis (e.g., nonspecific interstitial pneumonia) nor will an extensive search for exposures be pursued (e.g., as is done with patients with hypersensitivity pneumonitis).
Given the importance of correctly making a diagnosis of UIP and avoiding overdiagnosis of this entity, radiologists interpreting HRCT should be mindful of the potential pitfalls described in the following sections.
Correctly Distinguish Honeycombing From Mimics
Honeycombing can be confidently diagnosed when there is a group of round clustered air-filled cysts in a row or cluster in the subpleural lung [5]. The subpleural involvement in honeycombing is critical in distinguishing it from other abnormalities. Multiple layers of cysts increase the reader’s confidence in honeycombing but are not required for diagnosis. Honeycomb cysts usually range in size from 3 to 10 mm and have relatively thick, well-defined walls [6]. In general, there is moderate agreement among radiologists for the presence of honeycombing, with kappa values ranging from 0.4 to 0.6 in one series comparing 43 different observers. There was disagreement on the presence of honeycombing in 29% of these cases [7]. Use of the above general rules for the features of honeycombing is helpful when distinguishing from common mimics. The most frequent findings mistaken for honeycombing include traction bronchiectasis, cystic lung disease, emphysema, and subpleural reticulation [8].To distinguish traction bronchiectasis from honeycombing, the shape of the air-filled structure should be noted. Airways in traction bronchiectasis are tubular in shape, which may be best seen on multiplanar reformatted images. Additionally, air-filled structures in the central or peribronchovascular lung are not consistent with honeycombing and are very likely a result of dilated airways (Fig. 2).
Fig. 2—Patient with scleroderma and fibrotic nonspecific interstitial pneumonia. Left, HRCT scan shows traction bronchiectasis mimicking honeycombing. Right, HRCT scan shows that air-filled structures spare subpleural lung.
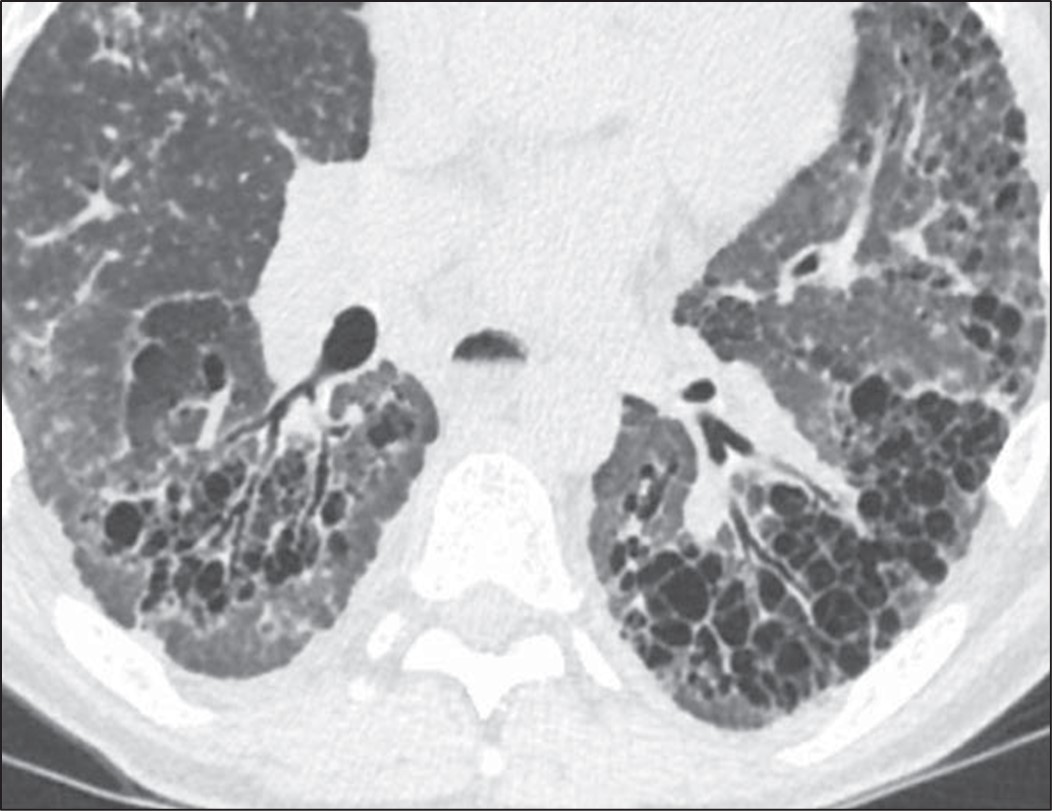
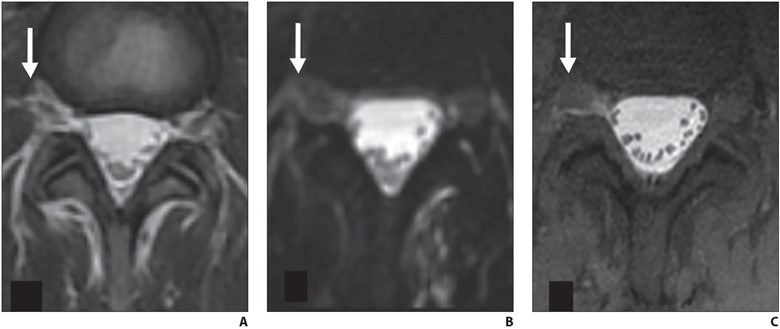
Destruction of airspaces in patients with emphysema can lead to the presence of air-filled structures in the subpleural lung; however, these structures can be distinguished from honeycombing by the overall size of emphysematous spaces that in general are larger than honeycombing cysts, the presence of paper-thin walls in emphysema in contrast to thicker walls of honeycombing, and the absence of other findings of fibrosis such as reticulation and traction bronchiectasis in patients with emphysema [9] (Fig. 3).
Fig. 3—HRCT scan shows patient with paraseptal emphysema with extensive involvement of subpleural lung, but without well-defined walls or other findings of fibrosis.
Cystic lung disease can be distinguished from honeycombing given that the cysts are often larger, scattered throughout the lung rather than clustered, and not subpleural in distribution. Shape can also be helpful in distinguishing cystic lung disease from honeycombing in that honeycomb cysts are round, whereas several cystic lung diseases are characterized by either oblong or elliptical cysts (Birt-Hogg-Dubé syndrome) or irregularly shaped cysts (Langerhans cell histiocytosis) [10].
Reticulation or fine lines in the subpleural lung can also be mistakenly identified as honeycombing. To avoid this pitfall, radiologists should ensure that the subpleural abnormality is air density rather than lung density (Fig. 4).
Fig. 4—HRCT scan shows thin lines in subpleural lung in patient with pulmonary fibrosis characterized by diffuse reticulation. Abnormality in subpleural lung is lung density (same as more central lung parenchyma) rather than air density (for example in trachea), which is helpful in confirming that these findings do not represent honeycombing.
Identify Whether the Distribution of Fibrosis Is Subpleural and Basal
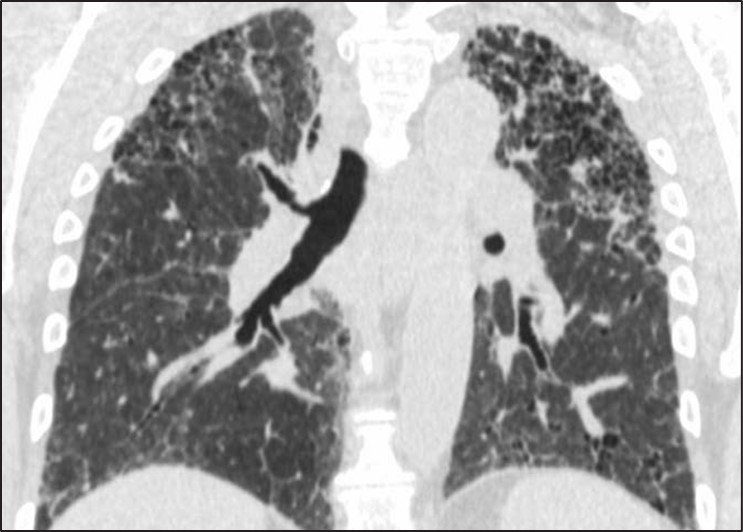
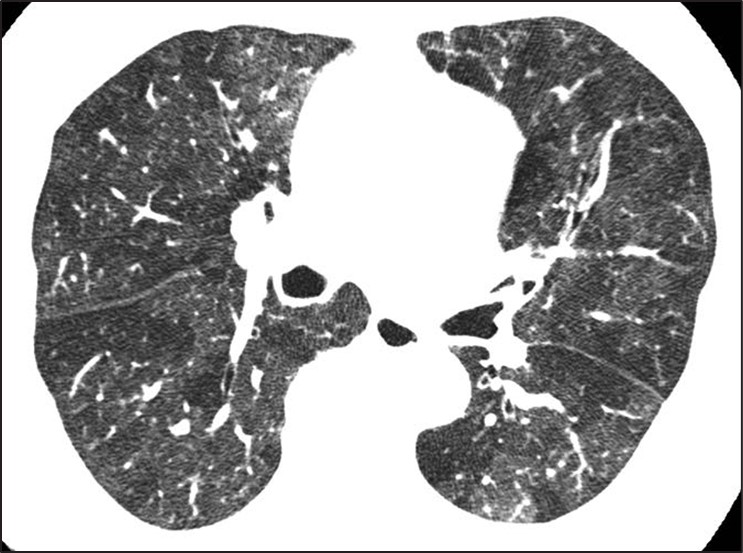
Fig. 5—Fibrosis with honeycombing in atypical distribution. Left, Axial HRCT scan shows diffuse fibrosis in association with ground-glass opacity. Diagnosis was hypersensitivity pneumonitis. Right, Coronal HRCT scan shows upper lobe–predominant fibrosis. Diagnosis was sarcoidosis.
Fibrosis that is diffuse in the axial plane or predominately in an upper lung, central, or peribronchovascular distribution may indeed be associated with honeycombing but nonetheless be caused by other entities such as nonspecific interstitial pneumonia, sarcoidosis, or hypersensitivity pneumonitis [11, 12]. Subpleural and basal distribution of fibrosis is essential to describing a pattern of fibrosis consistent with UIP at imaging. A percentage of cases with atypical distributions of fibrosis and honeycombing may be subsequently identified as UIP after biopsy; however, these cases are exactly those that benefit from surgical lung biopsy because there is a relatively high chance (70%) that another diagnosis will be found [12, 13].
Identify Inconsistent Findings
Numerous CT findings are of a diagnosis other than UIP pattern including the presence of significant ground-glass opacity, marked mosaic attenuation, nodules, and consolidation [13]. Each of these findings points the radiologist toward a diagnosis other than UIP. Patients with nonspecific interstitial pneumonia (i.e., ground-glass opacities), hypersensitivity pneumonitis (i.e., mosaic attenuation), sarcoidosis (i.e., nodules), and organizing pneumonia (i.e., consolidation) can all be identified by the presence of these features, and the presence of honeycombing should not detract from the CT findings that indicate these alternative diagnoses.
Overdiagnosis of Cystic Lung Disease
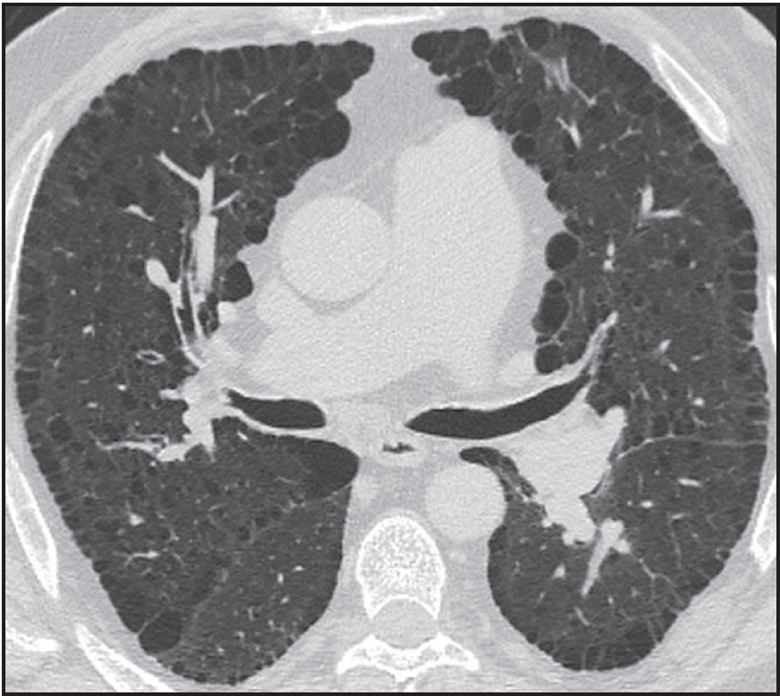
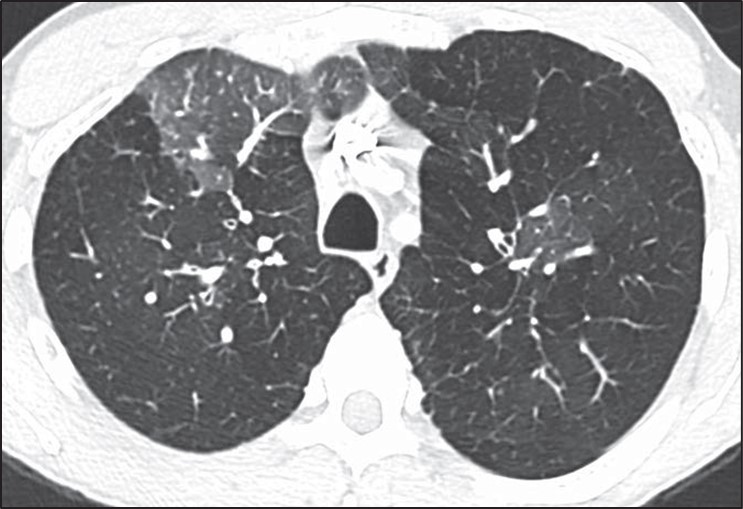
Many of the pitfalls in correctly identifying honeycombing and distinguishing honeycombing from mimics can also be applied to the correct diagnosis of cystic lung disease. When considering a potential diagnosis of cystic lung disease, it is important to again identify mimics: honeycombing, dilated airways and bronchiectasis, and emphysema. The extent of abnormality, from mild to severe, is also important to consider in this context. A few scattered pulmonary cysts may be considered in the spectrum of normal, particularly for older patients, and are most likely postinfectious rather than indicative of a cystic lung disease [14].Whereas the primary features of bronchiectasis (i.e., tubular shape) and honey- combing (i.e., thick walls, clustered, subpleural) make distinguishing these entities from cystic lung disease more straightforward, correctly distinguishing cystic lung disease from emphysema can be challenging. This challenge is in part because both entities can have very thin or imperceptible walls and can occur on a spectrum from mild to severe. The presence of the “central dot” sign in which the centrilobular artery is seen within an emphysematous space can be helpful in correctly distinguishing centrilobular emphysema from a cystic lung disease; however, this finding is not reliably seen in all regions of emphysema [15] (Fig. 6).
Fig. 6—Axial HRCT scan shows “central dot” sign in patient with centrilobular emphysema.
In general, pulmonary cysts are fewer in number, noncentrilobular in distribution, and have thicker or more perceptible walls compared with centrilobular emphysema [16]. Paraseptal emphysema and panlobular emphysema are less frequently mistaken for cystic lung disease because of their strongly subpleural distribution and overall extent respectively.
Distinguishing cystic lung diseases from one another can also be challenging; however, several key features including cyst shape, number, distribution, and classic demographic factors and associated findings can aid the radiologist in providing an appropriate differential diagnosis. Using these features allows the radiologist to narrow the differential diagnosis for a particular case to fit the specific CT features seen rather than including a long differential diagnosis consisting of all cystic lung diseases [17]:
Female sex, renal angiomyolipoma Pneumothorax, renal mass Cysts and nodules Smoker Ground-glass opacity, connective tissue disease
The presence of associated features may also be helpful in correctly identifying the presence and cause of a cystic lung disease when the abnormalities are mild and nonspecific.
Pitfalls in the Interpretation of Mosaic Attenuation and Small Airways Disease
Small airways disease may present a significant challenge in HRCT interpretation and typically manifests on HRCT as two main categories of findings: nodules or mosaic attenuation. Nodules may correspond to any of the following histologic findings: inflammation within the lumen of the airways, alveolar disease centered on the airway, or peribronchiolar interstitial inflammation. Diseases categorized by nodules are generally detected on HRCT with high sensitivity and are typically straightforward to classify.
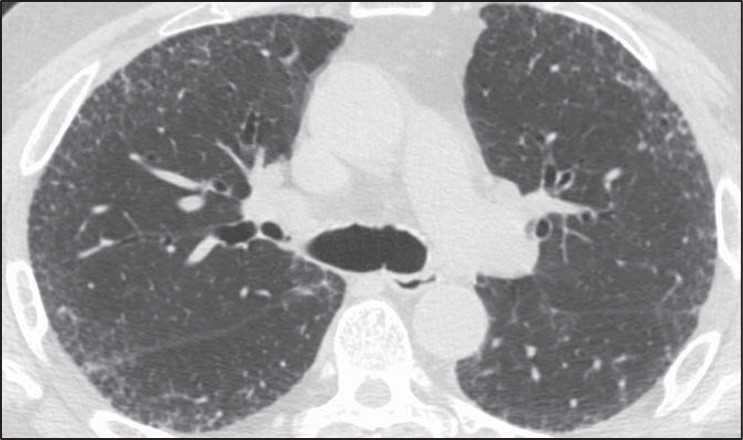
Small airways obstruction causes hypoxia distal to the area of obstruction, resulting in regional areas of reflex vasoconstriction. Given that approximately 50% of lung attenuation is due to blood flow, regional reductions in perfusion result in a decrease in lung attenuation. These regional areas of decreased lung attenuation are described as “mosaic attenuation” or “mosaic perfusion.” More precisely, mosaic attenuation is a more general term and describes the presence of geographic areas of different lung attenuation but does not make a determination as to which lung is abnormal, whether the opaque or lucent lung. Mosaic perfusion, on the other hand, implies specifically that the lucent lung is abnormal and is the finding that most precisely corresponds to airways obstruction with reflex vasoconstriction [18].
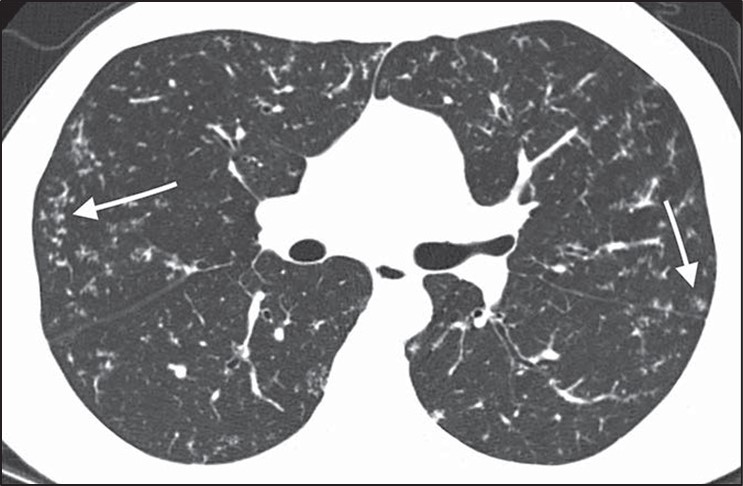
The differential diagnosis of mosaic perfusion is broad and encompasses a wide variety of both small airways diseases and pulmonary vascular diseases. It may be associated with other findings (e.g., nodules) or may be seen in isolation. The presence of mosaic perfusion is most helpful in formulating a differential diagnosis when seen in isolation, in which case it may be due to pulmonary vascular disease (mainly chronic thromboembolic disease), constrictive bronchiolitis, asthma, and hypersensitivity pneumonitis [19].Diseases characterized by isolated mosaic perfusion may present a significant challenge for several reasons. First, mosaic perfusion is a finding that is sometimes difficult to detect on HRCT. The subtle difference in attenuation frequently seen between the normal and more lucent lung is better observed when a narrow window is applied to the HRCT examination, accentuating the attenuation differences (Fig. 7).
Fig. 7—Mosaic perfusion and importance of windowing in high-resolution CT (HRCT). Left, Standard lung window in HRCT shows heterogeneous lung attenuation with subtle difference between opaque and lucent lung. Right, More narrow window accentuates difference between two lung attenuations and increases sensitivity for detection of mosaic perfusion.
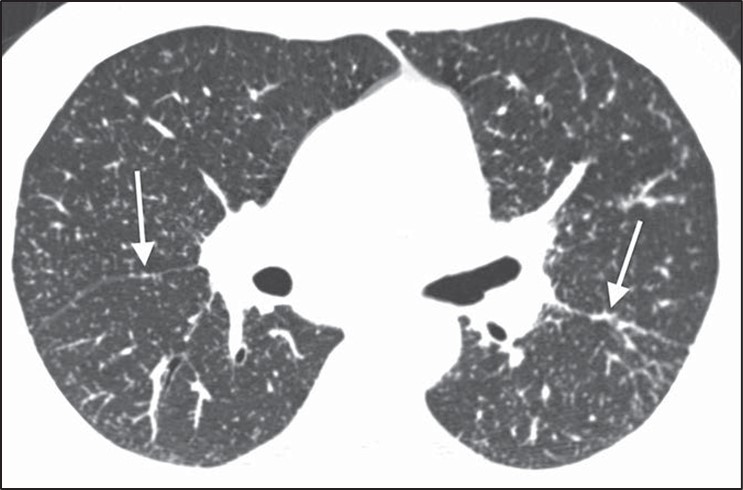
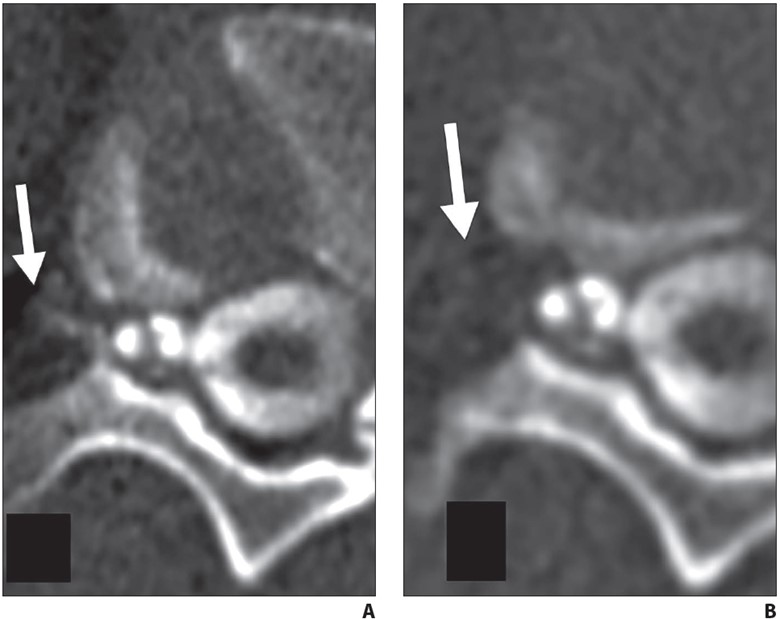
Second, when small airways or vascular diseases are diffuse in nature they result in a global and uniform decrease in lung perfusion. A diffuse HRCT abnormality is difficult to identify because there is no normal lung with which to compare the abnormality. This is most commonly seen in severe constrictive bronchiolitis [20]. Additionally, diffuse air trapping on expiratory CT is difficult to distinguish from poor timing or an inadequate respiratory effort. In these cases the HRCT scan may appear normal despite profound dyspnea and marked obstruction on pulmonary function tests. The diffuse but subtle decrease in lung attenuation is often not detected given its homogeneous nature.Mosaic perfusion (i.e., abnormal lucent lung) should be distinguished from ground-glass opacity (i.e., abnormal opaque lung), however, this distinction also has several pitfalls. Features that favor mosaic perfusion include sharp borders between the two regions of lung, smaller vessels in the lucent lung, and air trapping on expiration in the areas that were lucent on inspiration that only present in small airways disease (Fig. 8).
Fig. 8—Features of mosaic perfusion on high-resolution CT (HRCT). First two images, Axial HRCT scans show typical features of mosaic perfusion including sharp borders between opaque and lucent lung (first), larger vessels in normal more opaque lung (second), and air trapping on dynamic expiratory images. Third and fourth image, Paired inspiratory (third) and expiratory (fourth) HRCT images show heterogeneous lung attenuation on inspiration and air trapping on expiration.
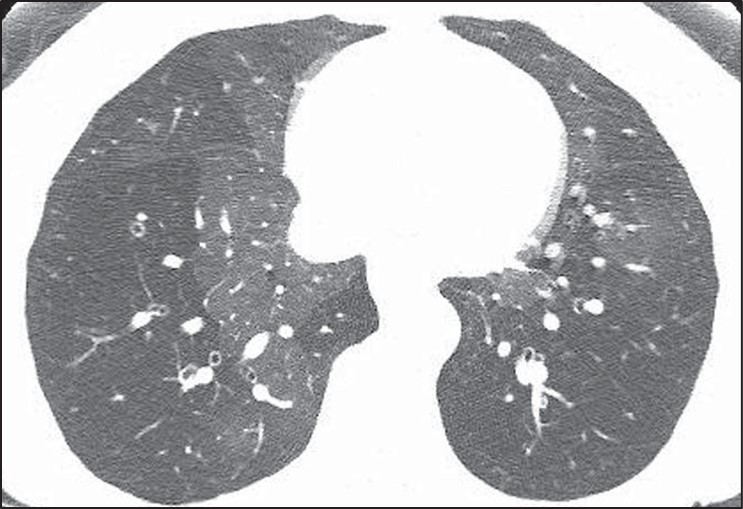
None of these features are perfect in making this distinction, however. For instance, diseases characterized by ground-glass opacity may occasionally be geographic with sharp borders (Fig. 9).
Fig. 9—Axial high-resolution CT scan shows ground-glass opacity due to SARS-CoV-2 infection. Sharp borders between areas of opaque and lucent lung usually suggest that lucent lung is abnormal and pattern is mosaic perfusion. However, sharp borders may occasionally be seen in ground-glass opacity, such as in this case. Normal lung and areas of ground-glass opacity show marked difference in attenuation.
In these cases, the absolute difference in attenuation between the two regions of lung may be helpful. Mosaic perfusion typically results in a relatively subtle difference in attenuation between the diseased lucent lung and the normal opaque lung. Ground-glass opacity, on the other hand, typically shows a more marked difference in density between the two areas [21]. That being said, when mosaic perfusion results in significant shunting of blood away from the diseased areas, a greater difference in lung attenuation may be present. These cases are not infrequently misinterpreted as ground-glass opacity. Another challenge in the distinction between mosaic perfusion and ground-glass opacity is that many cases of mosaic perfusion will not show a significant difference in vessel size between the lucent and opaque lung. Last, pulmonary vascular diseases characterized by mosaic perfusion will not show air trapping on expiratory CT. Thus, expiratory CT is not helpful in the diagnosis of diseases such as chronic pulmonary embolism [22].
Pitfalls in the Interpretation of Diffuse Nodular Lung Disease
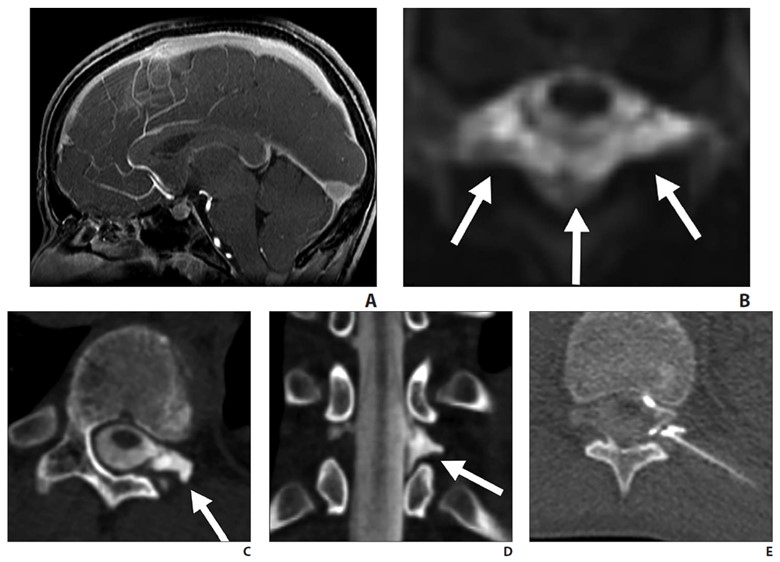
Formulating a differential diagnosis of diffuse nodular lung disease is done by identifying the distribution of nodules in relation to the pulmonary lobular anatomy. Three distributions have been described: perilymphatic, random, and centrilobular [23–25]. The perilymphatic distribution is characterized by patchy, clustered nodules that are concentrated most frequently in the peribronchovascular and subpleural interstitium. Random nodules will also be seen in the subpleural lung; however, they are not clustered but instead show diffuse homogeneous lung involvement. Centrilobular nodules are characterized by a distinct lack of nodules involving the subpleural interstitium.
The determination of the predominant pattern of diffuse nodular lung disease has several pitfalls. The perilymphatic pattern shows significant heterogeneity in the distribution of nodules. Although peribronchovascular and subpleural nodules are most typical, nodules in the interlobular septa, which also contain lymphatics, may predominate [26]. These cases may be confused for lymphangitic spread of tumor or pulmonary edema, although the thickening of the interlobular septa in pulmonary edema should be smooth, not nodular. The centrilobular interstitium is continuous with the peribronchovascular interstitium. Rarely, lymphatic diseases may have a predominance of centrilobular nodules overlapping with the centrilobular distribution (Fig. 10).
Fig. 10—Axial high-resolution CT scan shows centrilobular nodules in perilymphatic disease. Many centrilobular nodules (arrows) are present in this patient with sarcoidosis. Subpleural nodules reflect perilymphatic distribution of disease.
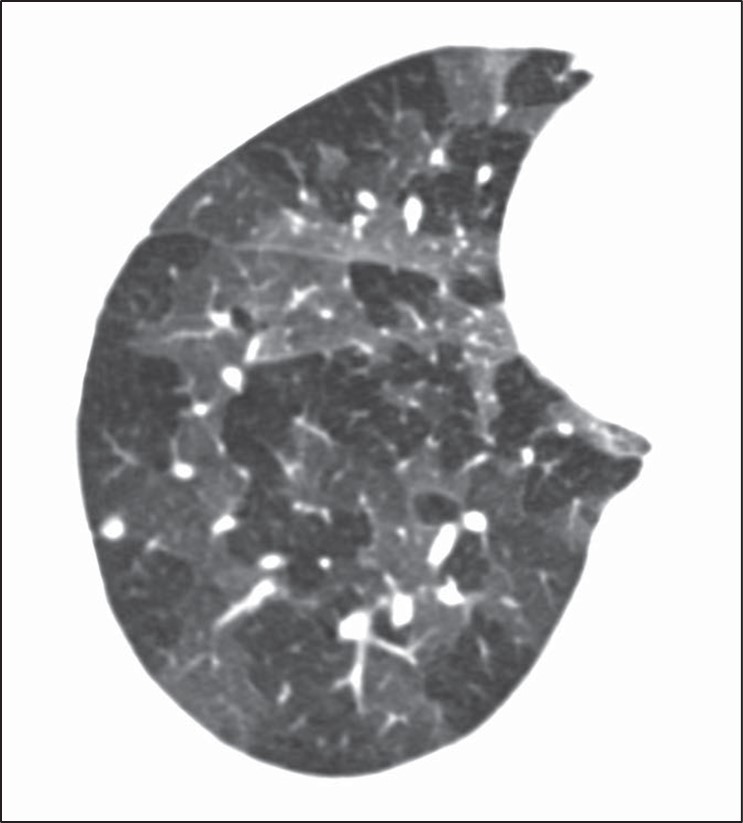
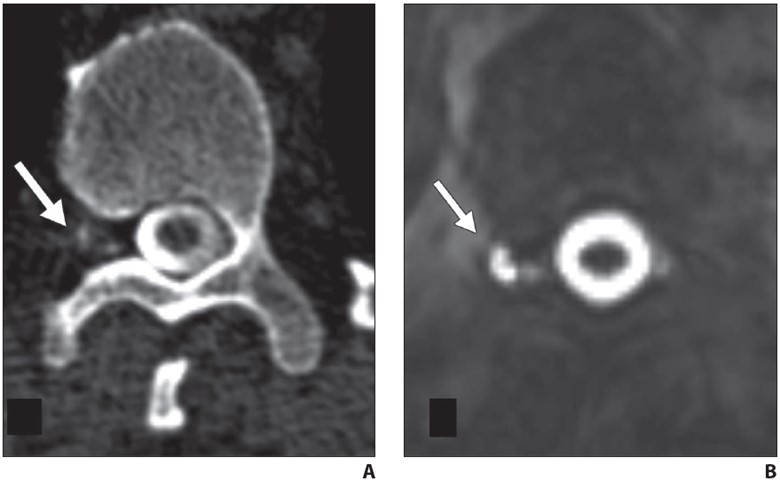
Although many centrilobular nodules may be present in lymphatic diseases, nodules should also be seen in the peribronchovascular or sub- pleural interstitium. This is in distinction to the centrilobular pattern in which only centrilobular nodules are present and no subpleural nodules should be seen. Lastly, diseases typically associated with a perilymphatic distribution of nodules (such as sarcoidosis) may occasionally show a fairly homogeneous involvement of the lung, mimicking a random distribution [27] (Fig. 11).
Fig. 11—Axial high-resolution CT scan shows perilymphatic distribution mimicking random nodules. Innumerable tiny nodules are present. Although pattern resembles random distribution, heterogeneous distribution in lung shows proportionally more nodules along fissures (arrows) than would be expected for random distribution.
A greater number of nodules in the subpleural or peribronchovascular interstitium may be the only clue that the distribution is perilymphatic.
Diseases for Which HRCT Has Limited Sensitivity
Certain categories of diseases may present with significant symptoms or pulmonary function test abnormalities but only manifest with mild HRCT abnormalities. Understanding the subtle imaging clues that may be present in these diseases is important in increasing the sensitivity of imaging for diagnosis. The two main categories of disease that show this discrepancy between symptoms and pulmonary function tests and HRCT manifestations of disease include small airways diseases and pulmonary vascular diseases. As discussed above, small airways diseases that manifest as isolated mosaic perfusion (e.g., constrictive bronchiolitis) may be difficult to detect on HRCT. The subtle increase in lung lucency associated with these diseases may be difficult to see, especially when the disease is diffuse in distribution [28]. Pulmonary vascular diseases such as pulmonary hypertension or chronic pulmonary embolism may also present with subtle findings. Centrilobular nodules or ground-glass attenuation or mosaic perfusion are often the only findings present and are typically much less severe than would be predicted by the patient’s advanced clinical symptoms. The lungs may appear completely normal in some patients with pulmonary vascular disease, in which case the only manifestation of pulmonary vascular disease may be extrapulmonary findings such as an enlarged pulmonary artery or right ventricular enlargement [29]. Lastly, pulmonary symptoms and pulmonary function test abnormalities might have one of several nonlung causes including pleural fibrosis, diaphragmatic dysfunction, and musculoskeletal abnormalities. All of these should be evaluated in patients with significant symptoms but no evidence of lung abnormalities on HRCT.
Awareness of common pitfalls in the diagnosis of ILD including the UIP pattern of fibrosis, cystic lung disease, airways disease, diffuse nodular disease, and lung diseases with subtle HRCT findings will better equip the radiologist to contribute to the multidisciplinary diagnosis of patients with ILD.
References
Hovinga M, Sprengers R, Kauczor HU, Schaefer-Prokop C. CT imaging of interstitial lung diseases. In: Schoepf UJ, Meinel FG, eds. Multidetector-row CT of the thorax. Springer, 2016:105–130
Wuyts WA, Cavazza A, Rossi G, Bonella F, Sverzellati N, Spagnolo P. Differential diagnosis of usual interstitial pneumonia: when is it truly idiopathic? Eur Respir Rev 2014; 23:308–319
Raghu G, Remy-Jardin M, Richeldi L, et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/ JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2022; 205:e18–e47
Brownell R, Moua T, Henry TS, et al. The use of pre- test probability increases the value of high-resolution CT in diagnosing usual interstitial pneumonia. Thorax 2017; 72:424–429
Hobbs S, Chung JH, Leb J, Kaproth-Joslin K, Lynch DA. Practical imaging interpretation in patients suspected of having idiopathic pulmonary fibrosis: official recommendations from the Radiology Working Group of the Pulmonary Fibrosis Foundation. Radiol Cardiothorac Imaging 2021; 3:e200279
Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology 2008; 246:697–722
Watadani T, Sakai F, Johkoh T, et al. Interobserver variability in the CT assessment of honeycombing in the lungs. Radiology 2013; 266:936–944
Arakawa H, Honma K. Honeycomb lung: history and current concepts. AJR 2011; 196:773–782
Devaraj A. Imaging: how to recognise idiopathic pulmonary fibrosis. Eur Respir Rev 2014; 23:215–219
Grant LA, Babar J, Griffin N. Cysts, cavities, and honeycombing in multisystem disorders: differential diagnosis and findings on thin-section CT. Clin Ra- diol 2009; 64:439–448
Abehsera M, Valeyre D, Grenier P, Jaillet H, Battesti JP, Braunerl MW. Sarcoidosis with pulmonary fibro- sis: CT patterns and correlation with pulmonary function. AJR 2000; 174:1751–1757
Silva CIS, Churg A, Müller NL. Hypersensitivity pneumonitis: spectrum of high-resolution CT and pathologic findings. AJR 2007; 188:334–344
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. an official ATS/ ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2018; 198:e44–e68
Araki T, Nishino M, Gao W, et al. Pulmonary cysts identified on chest CT: are they part of aging change or of clinical significance? Thorax 2015; 70:1156–1162
Friedman PJ. Imaging studies in emphysema. Proc Am Thorac Soc 2008; 5:494–500
Lee KC, Kang EY, Yong HS, et al. A stepwise diagnostic approach to cystic lung diseases for radiologists. Korean J Radiol 2019; 20:1368–1380
Ferreira Francisco FA, Soares Souza A, Zanetti G, Marchiori E. Multiple cystic lung disease. Eur Respir Rev 2015; 24:552–564
Parambil JG, Yi ES, Ryu JH. Obstructive bronchiolar disease identified by CT in the non-transplant population: analysis of 29 consecutive cases. Respirology 2009; 14:443–448
Loverdos K, Fotiadis A, Kontogianni C, Iliopoulou M, Gaga M. Lung nodules: a comprehensive review on current approach and management. Ann Thorac Med 2019; 14:226–238
Gruden JF, Webb WR, Naidich DP, McGuinness G. Multinodular disease: anatomic localization at thin-section CT—multireader evaluation of a simple algorithm. Radiology 1999; 210:711–720
Shroff G, Konopka K, Chiles C. Perilymphatic pulmonary nodules: definition, differential diagnosis, and demonstration of the “pipe-cleaner” sign. Con- temporary Diagnostic Radiology 2013; 36:1–5
Rajagopala S, Sankari S, Kancherla R, Ramanathan RP, Balalakshmoji D. Miliary sarcoidosis: does it exist? A case series and systematic review of literature. Sarcoidosis Vasc Diffuse Lung Dis 2020; 37:53–65
Hansell DM. Small airways diseases: detection and insights with computed tomography. Eur Respir J 2001; 17:1294–1313
Kacprzak A, Burakowska B, Kurzyna M, et al. Predictive value of chest HRCT for survival in idiopathic pulmonary arterial hypertension. Respir Res 2021; 22:293
Center for Evidence-Based Imaging Brigham and Women’s Hospital
What would you do if your hospital was going to run out of iodinated contrast? Reduce the amount of IV contrast used for each CT scan? Administer multiple doses of IV contrast from a single-use vial? Defer non-urgent contrast-enhanced CT? Utilize alternative modalities, such as ultrasound, MRI, or PET/CT?
In March of last year, supply chain disruptions in China resulted in an unexpected 80% reduction in global supply of iohexol (Omnipaque, GE Healthcare). Hospitals needed to make immediate decisions about ways to conserve contrast. Otherwise, they may run out. The American College of Radiology [1], Radiological Society of North America [2], and American Hospital Association [3] released statements, and AJR continues to publish all of its research regarding the contrast media shortage as free and open access [4].
The situation was rapidly evolving, but getting more inventory wasn’t an option. As part of the response to the contrast shortage, our hospital system created and implemented an electronic health record (EHR) -based solution to help reduce iodinated contrast usage by targeting referring provider CT ordering patterns [5].
First, we added a sidebar to the ordering panel that presented an alert describing the shortage (Fig. 1), including the following strategies for imaging patients (Intervention 1; May 10, 2022):
Fig. 1—Screenshot from electronic health record shows sidebar text displayed to referring clinicians after placing orders for body CT (defined as CT of neck, chest, or abdomen and pelvis) that describes iohexol shortage and provides appropriate strategies for iodinated contrast media conservation.
Oncologic Imaging
Avoid contrast for chest CT done alone to assess metastatic disease, unless primary is thoracic malignancy
For chest/abdomen/pelvis restaging exams, consider combining non-contrast CT chest with abdominal MRI
Consider abdominal MRI for assessment of hepatic metastases
Non-Oncologic Imaging
CT for pulmonary embolism (PE)—utilize risk scoring methodology, such as Wells criteria or pulmonary embolism rule-out criteria (PERC), before pursuing CT
CT chest for lung parenchymal disease does not require IV contrast
In case of suspected musculoskeletal infection, use MRI
Emergency Imaging
Neuro
CTA head/neck—contrast needed to assess large vessel occlusion in patients within stroke treatment window. For subacute stroke outside window, please consider non-contrast head CT, followed by MRI, when appropriate
Reconsider CTA utilization for low-yield indications, including headache and dizziness
Thoracic
CT for PE—utilize risk scoring methodology (i.e., Wells or PERC)
CT chest for lung parenchymal disease doesn’t require IV contrast
Abdomen/pelvis
Pancreatitis and pyelonephritis—CT rarely indicated for these diagnoses
For primary hepatobiliary concerns, right upper quadrant ultrasound remains an excellent choice, unless high likelihood that CT also needed to explain symptoms
GI Bleeding—reserve CTA for patients with bright red blood per rectum or hemodynamic instability in whom acute intervention might be needed
Trauma
CT torso with IV contrast is needed to assess for parenchymal or vascular injury.
Consider non-contrast CT torso imaging (or radiography) in patients with low suspicion for parenchymal or vascular injury, such as elderly patients with ground-level fall and suspicion for rib fracture or thoracic/lumbar spine fracture
Next, we required referrers to enter additional clinical information into a free text field describing why iodinated contrast was needed for the CT (Intervention 2; May 16, 2022).
The number of patients undergoing contrast-enhanced CTs per day decreased from 726 prior to the interventions, to 689 after intervention 1, to 639 after intervention 2 (Fig. 2).
Fig. 2—Box-and-whisker plots show changes during preintervention and postintervention periods in number of patients who underwent contrast-enhanced CT examinations per day. Centerlines represent medians, ends of boxes represent interquartile ranges, ends of whiskers represent interdecile ranges, and dots beyond ends of whiskers represent outliers.
The overall number of patients undergoing CT per day decreased, as did the percentage of CT exams performed with IV contrast. These decreases were seen for all CT, as well as body CT alone (neck/chest/abdomen/pelvis). As expected, there was a decrease in requests for contrast-enhanced CT and a corresponding increase in requests for non-contrast CT.
In summary, an EHR intervention was able to reduce the number of contrast-enhanced CTs per day by 12%, the total number of CTs performed per day decreased 2.7%, and the percentage of CTs performed with IV contrast per day decreased from 53.8% to 48.6%. This simple intervention was implemented within weeks of the onset of the shortage and led to rapid practice change. Along with other conservation strategies, our health system was able to avoid rationing and continue near normal operations.
References
Wang CL, Asch D Cavallo J. Statement from the ACR Committee on Drugs and Contrast Media on the Intravenous Iodinated Contrast Media Shortage. J Am Coll Radiol 2022; 19:834-835
Grist TM, Canon CL, Fishman EK, Kohi MP, Mossa-Basha M. Short-, mid-, and long-term strategies to manage the shortage of iohexol. Radiol 2022; 304:2
Glazer DI, Lucier DJ, Sisodia RC. Electronic health record order entry–based interventions in response to a global iodinated contrast media shortage: impact on contrast-enhanced CT utilization. AJR 2022; 220:1
Over the last few years, we in radiology have faced incredible and unprecedented challenges in our day-to-day work, and this is true regardless of our specific work environments. Why? The pandemic, which has touched everyone, has had a profound impact on the workplace in general. It has changed how we work, approach work, and shaped our opinions of work. And it is not just the pandemic—it’s other phenomena: political polarization, social unrest, changes in home life and education, remote work. The pandemic and its effects led to a great resignation, and as a result, many of our sites are now understaffed. One in five doctors plan to leave their current practice in two years; two in five nurses plan to leave their practice in two years; one in three doctors expect to work less next year.
Health care workers have far greater demands now than in the pre-pandemic times. The delivery of health care has changed dramatically and quickly over the last few years. There is unprecedented “consumerism” in medicine now with a mandate to improve and rethink patient access, to provide more and better mental health services to our populations, and to have transparent pricing.
In radiology, whether you work in a large or small private practice, remotely by yourself, an academic department in a medical center, or part of a mega radiology practice, there has been a palpable shortage of radiologists. This shortage is fueled by a trend toward exclusive subspecialization with declining numbers of radiologists who can handle general work, ever-increasing expectations for service to our patients, referring doctors, hospitals, and health care systems. We have been stretched thinner. There is a desire by radiologists to have more flexible work hours or, simply stated, to work less hours overall compared to years past. There is a concern about what role artificial intelligence and machine learning will play; will we be displaced? Reimbursement has been decreasing relative to inflation and compared with other specialties. As a result of these realities and others, there is clear evidence of burnout among radiologists, similar to health care workers in other specialties. On top of that, sometimes, we find that the leaders in our organizations may be distant, or too corporate, or suffer from “toxic positivity,” which may be worse than “toxic negativity.”
There has been a steady headwind for years, but it now feels like a gale force wind. And a lot of this feels out of our control. So, goodness, how do we manage all of this?
Hold on, let’s take a breath. One strategy that we can embrace and control is to develop a culture of teams within our workplaces. In fact, I have titled this series “The Teamwork Imperative” because we must establish teamwork as a core value within the radiology workforce. I believe that if we foster a culture of teams, we can mitigate and shield ourselves from some of these headwinds.
Obviously, I’m not the first to suggest the importance of teams. It’s all over the blogs and press and our literature. In last year’s presidential address, Dr. Gary Whitman alluded to the importance of a culture of resiliency and teamwork [1]. I will also shout out to the 2021 president of our society, Dr. Jonathan Kruskal. Dr. Kruskal, along with colleagues and ARRS staff, launched RadTeams.org—an open-access website that helps radiologists establish, grow, and sustain high-functioning radiology teams, along with other aspects of imaging wellness and wellbeing [2]. Check it out. And you have to revisit the exciting ARRS Radiology Wellness Summit from the Annual Meeting that addressed, among many things, the importance of teams [3, 4].
Let me be clear. Here, when I say teams, I am specifically not referring to the “macro teams” that many of us find ourselves in. For example, at Duke Health, it is said that the 30,000-plus employees are my “teammates.” That very well may be true. But no, I am referring to your local and focal team. I am referring to the individuals that you rely on daily or weekly to deliver your work product. It’s the folks you huddle with. And the teams develop where you huddle. If you are in training, I am referring to your team of co-residents, your chief residents, maybe your program director or program coordinator who you lean on. If you are in a private practice, I am referring to those that you share physical space with, or perhaps switch call with, or the individuals you show difficult cases to, or the referring docs you have developed close relationships with, and who rely on you to deliver care. In an academic environment like mine, it might be the members of your subspecialty division. If done well, the division pulls together as a team to deliver care, service, teaching, and research.
Those divisions that have a culture of team are far more effective than those who are unable to act as a team. If you are lucky enough to have these local and focal teams (and these often form and evolve organically), many challenges at work open up and become more manageable and attainable. The clouds begin to lift. Specifically, your deliverables, whatever they may be, are far more easily and effectively achieved if you have your team and approach your work from the perspective of that team.
Work becomes more efficient and fulfilling and, frankly, more fun. The work becomes more manageable, with more aspects under your control. You become more engaged. And that then becomes an antidote to burnout. Teams, therefore, contribute to retention.
Coaches discuss this all the time. Just as Dr. Whitman was fond of quoting UCLA basketball coach John Wooden in his InPractice columns [5, 6], I’ll borrow here from Mike Krzyzewski, the legendary Duke basketball coach. “Coach K” famously talked about the five keys to an effective team and likened the keys to the fingers on a hand. Each finger is individual and can stand alone, but when the fingers come together into a fist, the fist proves to be much stronger than the sum of the individual fingers.
Communication, trust, responsibility, caring, productivity—my next installments of “The Teamwork Imperative” will discuss all five of these fingers and more, so please do stay tuned!
ARRS RadTeams website. About page. RadTeams.org/About. Accessed July 26, 2023
Kruskal J, Azour L, Goldin J. Introducing the ARRS Radiology Wellness Summit in Hawaii—Time to Get Serious! ARRS InPractice website. www.radfyi.org/radiology-wellness-summit-arrs-2023-hawaii. Published August 1, 2022. Accessed July 26, 2023
Kruskal J, Azour L, Goldin J. A Lighthouse for Radiology Wellness. ARRS InPractice website. www.radfyi.org/a-lighthouse-for-radiologists. Published November 14, 2022. Accessed July 26, 2023
Whitman GJ. Be a Primary Radiologist. ARRS InPractice website. www.radfyi.org/primary-radiologist. Published August 5, 2022. Accessed July 26, 2023
Whitman GJ. Repairing the World. ARRS InPractice website. www.radfyi.org/repairing-the-world. Published November 4, 2022. Accessed July 26, 2023
Sadia R. Qamar, Ramin Hamidizadeh, Samad Shah, Patrick McLaughlin, Anto Sedlic, Savvas Nicolaou
Department of Radiology University of British Columbia
Memoona Mian
Department of Radiology University of Arkansas for Medical Sciences
Prompt and early diagnosis is vital for timely treatment of traumatic cardiac emergencies. Myocardial rupture is a rare cause of immediate death after blunt cardiac trauma, with only 0.3–1.1% of patients with trauma reaching the emergency department (ED) [1]. Pericardial tears caused by deceleration forces or rib cage fractures are uncommon after blunt chest trauma, with a frequency of 0.3–0.5%. Rarely, valvular dysfunction can be seen due to an abrupt raised intracardiac pressure against a closed valve resulting from sudden rise in intraabdominal pressure translating into the heart causing valve cusp avulsion or tear [2]. Penetrating trauma can result in pericardial injuries further complicated by life-threatening conditions including partial or complete transdefect cardiac herniation or luxation with a mortality rate as high as 67%.
Plain radiographs will show pneumopericardium, hydrothorax or hemothorax, and mediastinal hematoma. Echocardiography will show abnormal valve function; wall motion abnormalities with decreased left ventricular ejection fraction; and pericardial effusion, signs of cardiac tamponade, or both. CT will show pneumopericardium, pericardial effusion, pericardial or myocardial laceration or rupture, cardiac herniation or luxation with associated SVC obstruction or right heart strain, valvular cusp avulsion or tears, coronary artery dissection or rupture, and associated rib cage fractures, retained foreign bodies, bullet fragments, and wound tracks [3] (Fig. 1).
Fig. 1—29-year-old man with gunshot wound. Left, Axial four-chamber cardiac CT image shows bullet fragment (arrow) abutting left ventricular side wall at mid cardiac level without myocardial penetration. Right, Mid ventricle short-axis color-coded functional cardiac CT image depicts reduced perfusion (white arrow) consistent with myocardial contusion. Black arrow indicates bullet fragment.
Imaging Pearls and Pitfalls in Cardiac Trauma
Any pericardial effusion detected in the acute trauma setting is presumed to be hemopericardium until proven otherwise. CT provides valuable information about the possible nature of pericardial effusions on the basis of the attenuation measurements of the collection. Coronary artery injuries are rare (in less than 2% of chest trauma cases), with left anterior descending artery being most commonly injured [4]. Penetrating cardiac trauma can result in pericardial injuries, which can result in partial or complete transdefect cardiac herniation or luxation with mortality up to 70% [5]. Portable supine studies in ED are suboptimal with overlying artifacts, which limits evaluation. TEE is invasive and difficult to perform in patients with acute craniocervical injuries. Cardiac MRI in trauma is primarily useful as a problem-solving tool after patients are admitted, especially to delineate the extent of myocardial contusion, regional infarction, wall motion abnormality, and valvular dysfunction.
Limitations of MDCT
First, CT involves use of ionizing radiation which increase the radiation exposure in the population. Second, the quality of MDCT images suffers with fast heart rate and high calcium burden. Finally, the patients with arrhythmias, ectopy or misregistration ECG artifacts degrade the image quality and limit evaluation. Optimizing techniques should be incorporated to counter these limiting factors.
Reduction of Radiation Dose
Radiation dose can be reduced with a prospective ECG-gated technique with narrow window acquisition, ECG tube current modulation, and limited pulse windows; tube voltage reduction based on body mass index; automated tube voltage reduction based on topogram attenuation profile; adaptive collimation limiting helical over spiral scanning; and iterative reconstructive techniques to reduce noise and ultimately reduce dose.
Optimizing Quality of Cardiac CT
Several steps can be taken to optimize the quality of cardiac CT studies. A heart rate of less than 65 beats/min can be achieved by administering 5–20 mg of β-blocker (metoprolol) IV or 50–100 mg by mouth 1 hour before the CT. Lowering the heart rate widens diastole and decreases beat-to-beat variability. Coronary arterial dilatation for optimal visualization can be achieved by administering 0.4–0.8 mg of nitroglycerin sublingually 5 minutes before contrast injection. Reconstruction algorithms can be used to reduce beam-hardening artifacts from iodine that mimic ischemia (Fig. 2).
Fig. 2—CT images show beam-hardening correction (left) and utility of B23 kernel (right) as it reduces beam-hardening artifact from iodine in left ventricle and thoracic aorta, affecting posterior inferior aspect of left ventricle wall mimicking infarct.
Edge-enhancing reconstruction algorithms can be used to reduce noise caused by extensive coronary calcifications or coronary stents.
Emerging Applications and Outlook
Coronary Atherosclerotic Plaque Characterization
The rationale behind growing efforts to accurately characterize a vulnerable, predominantly lipid-rich, plaque is its grave association with ACS and SCD. Novel attenuation-based application of dual-energy CT (DECT) has shown promising results when correlated with histologic findings. Spectral attenuation curves for material characterization are generated using attenuation values of a specific material for each and every monochromatic energy ranging from 40 to 140 keV [6]. Lipid-rich atherosclerotic plaques share the known attenuation curve of fat, in which attenuation decreases with lower monochromatic energy, thus differentiating lipid-rich plaques from fibrous plaques [7].
CT-Derived Fractional Flow Reserve
Coronary blood-flow volume effectively provides an estimation of lesion-specific ischemia. Recent vigorous advancements in digital analysis of fluid dynamics allow noninvasive assessment of coronary flow on the basis of mathematic models. CT-derived fractional flow reserve (FFR) calculates lesion-specific FFR using static coronary CT data without additional radiation or modification in image acquisition protocols. Studies have found that CT FFR shows 90% sensitivity and nearly 83% specificity for lesions with moderate stenosis causing ischemia [38]. A multicenter prospective trial showed 73% specificity and 90% sensitivity for CT FFR in diagnosing obstructive CAD compared with conventional angiographic FFR [8].
CT Myocardial Perfusion and Viability
Myocardial perfusion is one of the most important prognostic indicators for patient outcome and management of CAD. CT myocardial blood pool analysis using myocardial iodine content is a promising dynamic technology. DECT color-coded iodine maps permit sensitive detection of myocardial perfusion by depicting myocardial blood pooling [9]. The perfused myocardium takes up iodine, but no iodine uptake is seen in the infarcted myocardium (Fig. 3). Assessment of myocardial viability predicts successful revascularization therapy.
Fig. 3—Myocardial ischemia in 51-year-old man. Left and right, Mid ventricle short-axis cardiac CT image (left) and iodine perfusion map (right) show decreased subendocardial iodine uptake (arrows) in inferior basal ventricle, suggesting perfusion defect consistent with myocardial ischemia.
MDCT is a viable, reliable, and potentially effective imaging modality in evaluation of coronary and noncoronary cardiac emergencies. Cardiac CT efficiently rules out CAD in patients with low to intermediate risk who present with acute chest pain in the ED and accurately predicts midterm adverse outcome. With integration of innovative applications like morphologic plaque characterization, coronary FFR and myocardial perfusion, cardiac CT will be able to offer unprecedented benefits, ranging from triage to treatment decisions in the ED.
References
Mirvis SE. Imaging of acute thoracic injury: the advent of MDCT screening. Semin Ultrasound CT MR 2005; 26:305–331
Farhataziz N, Landay MJ. Pericardial rupture after blunt chest trauma. J Thorac Imaging 2005; 20:50–52
Sohn JH, Song JW, Seo JB, et al. Pericardial rupture and cardiac herniation after blunt trauma: a case diagnosed using cardiac MRI. Br J Radiol 2005; 78:447–449
Bruschi G, Agati S, Iorio F, Vitali E. Papillary muscle rupture and pericardial injuries after blunt chest trauma. Eur J Cardiothorac Surg 2001; 20:200–202
Prêtre R, Chilcott M. Blunt trauma to the heart and great vessels. N Engl J Med 1997; 336:626–632
Beckman JA, Ganz J, Creager MA, Ganz P, Kinlay S. Relationship of clinical presentation and calcification of culprit coronary artery stenoses. Arterioscler Thromb Vasc Biol 2001; 21:1618–1622
Min JK, Leipsic J, Pencina MJ, et al. Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA 2012; 308:1237–1245
Yoon YE, Choi JH, Kim JH, et al. Noninvasive diagnosis of ischemia-causing coronary stenosis using CT angiography: diagnostic value of transluminal attenuation gradient and fractional flow reserve computed from coronary CT angiography compared to invasively measured fractional flow reserve. JACC Cardiovasc Imaging 2012; 5:1088–1096
Han R, Sun K, Lu B, Zhao R, Li K, Yang X. Diagnostic accuracy of coronary CT angiography combined with dual-energy myocardial perfusion imaging for detection of myocardial infarction. Exp Ther Med 2017; 14:207–213
I am deeply honored and grateful to serve as the 123rd president of the American Roentgen Ray Society (ARRS). As you know, our society is the oldest radiology society, and we are widely regarded as the education society.
As a medical student, I started perusing the radiology journals; they were on library shelves back then, and there was the gray one and the yellow one. I loved the one with the yellow cover, the American Journal of Roentgenology, and I have ever since. Indeed, the ARRS was the first radiology society that I became aware of. I joined the society as a radiology resident, and I have been a member ever since.
Now, as ARRS president, I encourage all of our learners to join.
Left to right: Erik K. Paulson, Gary J. Whitman, and Deborah A. Baumgarten on stage during the Opening Ceremony of the 2023 ARRS Annual Meeting in Honolulu, HI.
It takes a team to run the society, and we have one. I would like to thank the hardworking and dedicated members of our Executive Council. Also, I would like to thank the Executive Committee of the Council, consisting of president-elect Angelisa M. Paladin, MD; vice president Deborah A. Baumgarten, MD, MPH; and secretary-treasurer Christine M. Glastonbury, MD.
Left to right: Nadja Kadom, Courtney Coursey Moreno, Christine M. Glastonbury, and Angelisa M. Paladin enjoy front-row seating at the Hawaii Convention Center.
A special and large thanks to outgoing ARRS president Gary J. Whitman, MD, who did a fabulous job in many respects.
Dr. Paulson receives the ARRS presidential gavel from Dr. Whitman on Sunday, April 16, 2023.
In addition, Susan B. Cappitelli, MBA, CAE, and her excellent ARRS staff deserve robust recognition. And thanks to all of our almost 20,000 dedicated members, who we serve, of course.
Importantly, I would like to thank my family and my wife, Kathy Merritt, who has been a rock of support throughout my entire career.
Over the last few years, we in radiology have faced incredible and unprecedented challenges in our day-to-day work, and this is true regardless of our specific work environments. Why? The pandemic, which has touched everyone, has had a profound impact on the workplace in general. It has changed how we work, approach work, and shaped our opinions of work. And it is not just the pandemic—it’s other phenomena: political polarization, social unrest, changes in home life and education, remote work. The pandemic and its effects led to a great resignation, and as a result, many of our sites are now understaffed.One in five doctors plan to leave their current practice in two years; two in five nurses plan to leave their practice in two years; one in three doctors expect to work less next year.
Health care workers have far greater demands now than in the pre-pandemic times. The delivery of health care has changed dramatically and quickly over the last few years. There is unprecedented “consumerism” in medicine now with a mandate to improve and rethink patient access, to provide more and better mental health services to our populations, and to have transparent pricing.
In radiology, whether you work in a large or small private practice, remotely by yourself, an academic department in a medical center, or part of a mega radiology practice, there has been a palpable shortage of radiologists. This shortage is fueled by a trend toward exclusive subspecialization with declining numbers of radiologists who can handle general work, ever-increasing expectations for service to our patients, referring doctors, hospitals, and health care systems. We have been stretched thinner. There is a desire by radiologists to have more flexible work hours or, simply stated, to work less hours overall compared to years past. There is a concern about what role artificial intelligence and machine learning will play; will we be displaced? Reimbursement has been decreasing relative to inflation and compared with other specialties. As a result of these realities and others, there is clear evidence of burnout among radiologists, similar to health care workers in other specialties. On top of that, sometimes, we find that the leaders in our organizations may be distant, or too corporate, or suffer from “toxic positivity,” which may be worse than “toxic negativity.”
There has been a steady headwind for years, but it now feels like a gale force wind. And a lot of this feels out of our control.
So, goodness, how do we manage all of this?
Hold on, let’s take a breath. One strategy that we can embrace and control is to develop a culture of teams within our workplaces. In fact, I have titled this InPractice series “The Teamwork Imperative” because we must establish teamwork as a core value within the radiology workforce. I believe that if we foster a culture of teams, we can mitigate and shield ourselves from some of these headwinds. During my term as your ARRS president, future installments of “The Teamwork Imperative” here in InPractice will feature specific thoughts on this subject, borrowing some thoughts from the game of basketball’s great coaches.
To officially kick off the 123rd meeting of the ARRS, Lopaka Kapanui, the island’s foremost practitioner of oli kāhea (entrance chant), welcomed society members from more than 40 countries with the open hand and heart of aloha—duly noting “e mau ana ka ‘ike” (the knowledge must continue).
Erik K. Paulson
Erik K. Paulson, MD, chair of the radiology department at Duke University, was installed as the 123rd president of ARRS. “I am absolutely honored and delighted to serve as the president of our country’s oldest radiology society, a society whose sweet spot is member education,” Dr. Paulson said during his opening remarks at the Hawaii Convention Center. “It takes a team, though,” he acknowledged. And joining Dr. Paulson are the following newly elected ARRS officers for 2023–2024: Angelisa M. Paladin, President-Elect; Deborah A. Baumgarten, Vice President; and Christine M. Glastonbury, Secretary-Treasurer.
Dr. Paulson succeeds Gary J. Whitman, MD. Having presided over our society ably and honorably from 2022 to 2023, Dr. Whitman presented this year’s coveted ARRS awards. The first laurels of the morning went to Bernard F. King, Jr., MD, FACR, FSAR, the 117th President of ARRS, who was awarded the 2023 ARRS Gold Medal. The highest distinction bestowed by ARRS, our Gold Medal has been honoring distinguished service to radiology for more than four decades.
Bernard F. King, Jr.
Jon A. Jacobson, MD, FACR, was then recognized as the 2023 ARRS Distinguished Educator. The ARRS Distinguished Educator award recognizes outstanding individuals in the field of medical imaging, who have a proven record of improving radiological education and remain committed to creating and implementing new and innovative educational activities.
Jon A. Jacobson and Gary J. Whitman
Next, ARRS was proud to recognize two recipients of 2023 ARRS Scholarships: Andrew Wentland, assistant professor at the University of Wisconsin School of Medicine & Public Health, and Steven Rothenberg, assistant professor at the University of Alabama at Birmingham. Provided by ARRS’ own The Roentgen Fund®, the ARRS Scholarship supports early-career faculty members pursuing radiological research that promises to change how medical imaging is practiced. A two-year grant totaling $180,000, the ARRS Scholarship aims to advance emerging scholars, as well as prepare them for positions of leadership.
During the American Journal of Roentgenology (AJR) Luncheon, Sarah Kamel of Thomas Jefferson University Hospital in Philadelphia, PA was honored as the 2023 Melvin M. Figley Fellow in Radiology Journalism, while Ankur Goyal of the All India Institute of Medical Sciences in New Delhi was recognized as the 2023 Lee F. Rogers International Fellow in Radiology Journalism.
Left to right: Ankur Goyal, Andrew B. Rosenkrantz, Sarah Kamel
Also provided by The Roentgen Fund and named for two distinguished Editors Emeriti of the American Journal of Roentgenology (AJR), the Melvin Figley and Lee Rogers Fellowships offer practicing radiologists an unparalleled opportunity to learn the tenets of medical publishing via “the yellow journal”—the world’s longest continuously published radiology journal. Through hands-on experience with ARRS staff and AJR personnel—as well as personal apprenticeship with AJR’s 13th Editor of Chief, Andrew B. Rosenkrantz—Drs. Kamel and Goyal will receive expert instruction in scientific writing and communication, manuscript preparation and editing, peer review processes, journalism ethics, and both print production and digital publication.
2023 ARRS Honorary Member: Jeong Min Lee
Jeong Min Lee
Jeong Min Lee, President of the Korean Society of Radiology, was recognized with honorary membership as part of ARRS’ Global Partner Society (GPS) program. The GPS program was established to build long-standing relationships with key leaders and societies in the global imaging community to enhance understanding, raise awareness, and increase participation in programs and services. The Annual Meeting Global Exchange incorporates one partner society annually into the educational and social fabric of the meeting, with ARRS reciprocating at the partner society’s meeting that year. The GPS partner to be featured at the 2024 ARRS Annual Meeting in Boston, MA, will be the British Institute of Radiology.
@AndrewCallenMD Department of Radiology, Neuroradiology Section, University of Colorado Anschutz Medical Campus
Spontaneous intracranial hypotension (SIH) is a disabling headache disorder caused by abnormal leakage of CSF through a dural defect, ruptured meningeal diverticulum, or CSF venous fistula (CVF) [1]. The clinical hallmark of this syndrome is a headache that improves when supine and worsens when upright. Although iatrogenic post–dural puncture headaches have been recognized for over a century, the understanding of spontaneous leakage of CSF and its associated syndrome has evolved rapidly over the past decade [2]. CVF in particular was first recognized in 2014, so our understanding of how to localize and treat this specific pathology is in its relative infancy [3].
As radiologists, we find ourselves uniquely positioned to both diagnose and treat patients with spontaneous intracranial hypotension (SIH). Understanding the spectrum of SIH imaging abnormalities in the brain and spine, how to implement specialized MRI and myelographic protocols to localize CSF leaks and CVF, and the treatment options available allows optimal care of these patients [4].
First-Line Evaluation With Noninvasive Imaging
MRI of the Brain
Routine MRI brain protocols consisting of contrast-enhanced 3D T1-weighted, susceptibility-weighted, and T2-weighted FLAIR sequences are sufficient to evaluate evidence of underlying SIH. Changes during SIH can be framed in terms of the Monro-Kellie doctrine: in normal states, the volumes of blood, CSF, and brain parenchyma are in equilibrium [5]. In response to abnormal CSF deliquoration, compensatory enlargement or deformation of brain parenchyma and vascular structures occurs, resulting in sagging of the brainstem, diffuse circumferential pachymeningeal thickening, epidural venous engorgement, and pituitary hyperemia [6]. Subdural hygromas or hematomas may occur secondary to distention of intracranial venous structures, which must not be mistaken for posttraumatic hemorrhage, as surgical evacuation of the collections will not improve the patient’s underlying pathology [6]. Hemosiderosis, particularly of the infratentorial brain, can be seen and may be due to repeated microtrauma to the epidural venous plexus at the dural defect, resulting in circulation of subarachnoid blood products [7] (Fig. 1).
Fig. 1—MRI findings of spontaneous intracranial hypotension. A, Sagittal contrast-enhanced T1-weighted image shows sagging of brainstem with effacement of mamillopontine, prepontine, and suprasellar intervals as well as engorgement of dural venous sinuses. B, Coronal contrast-enhanced T1-weighted image shows bilateral subdural hygromas (solid arrows) and diffuse smooth pachymeningeal thickening and enhancement (dashed arrows). C, Axial susceptibility-weighted image shows diffuse infratentorial hemosiderosis (arrows).
Emerging evidence suggests that although findings of SIH are specific for an underlying CSF leak, brain MRI may have limited sensitivity for these findings, particularly in chronic leaks [8]. A recent meta-analysis suggests that at least 19% of patients with proven CSF leaks may have normal findings on brain MRI [9]. Additional studies have reported that as a CSF leak persists, imaging findings either resolve or become more subtle, particularly diffuse pachymeningeal enhancement [10].
The following Bern criteria [11] have been developed as a scoring system using both qualitative and quantitative information on brain MRI to assign high, intermediate, or low probability of SIH:
Bern Criteria for Assessment of Spinal CSF Leak Based on Brain MRI Findings
MRI Finding
No. of Points
Pachymeningeal enhancement
2
Venous engorgement
2
Suprasellar effacement (≤ 4 mm)
2
Subdural collection
1
Prepontine effacement (≤ 5 mm)
1
Mamillopontine effacement (≤ 6.5 mm)
1
Note—Based on information in Dobrocky et al. [11]. When points for individual findings are totaled, 0–2 points indicates low probability of spontaneous intracranial hypotension, 3–4 points indicates moderate probability, and 5 or more points indicates high probability.
Standardized reporting for brain MRI with clinical indications suggestive of underlying SIH can appropriately frame the risks and benefits of further invasive diagnostic testing and avoid wrongly characterizing a patient as not having SIH because of a negative brain MRI examination. The radiologist’s understanding of limited sensitivity of brain MRI is critical for patients with SIH; it is strongly encouraged to adopt language that conveys probabilities of underlying SIH and incorporation of Bern scoring to not prevent further diagnostic workup in cases of high clinical suspicion.
MRI of the Spine
If SIH is suspected on the basis of clinical or imaging findings, imaging evaluation of the spine must be performed, as most CSF leaks resulting in SIH occur in the spine, not from the skull base [12]. In the upright position, intracranial pressure is slightly negative relative to atmospheric pressure, and pressure in the spinal compartment is slightly positive, which can result in spontaneous leakage of CSF in sufficient quantities to result in SIH [13]. This phenomenon is critical for the radiologist to understand, as it is not rare for patients to be inappropriately referred for CT cisternography in the context of orthostatic headaches, positive brain MRI, and rhinorrhea for suspicion of an underlying skull base leak.
Although routine spine imaging protocols can adequately delineate a dorsal or ventral spinal epidural CSF collection, leaks originating from the lateral dura (ruptured nerve root axilla or meningeal diverticulum) will not be evident on routine axial non–fat-saturated T2-weighted MRI. Similarly, laterally directed meningeal diverticula will not be completely characterized on routine protocols (Fig. 2).
Fig. 2—Axial lumbar spine MRI findings of 39-year-old woman with orthostatic headache. (B and C adapted from [4]) A and B, Axial T2-weighted (A) and heavily T2-weighted fat-saturated (B) images do not delineate any clear extradural fluid. T2-weighted hyperintensity lateral to dura (arrow, A) blends with fat and epidural veins (A). Three-dimensional CSF leak protocol shows minimal T2-weighted asymmetry (arrow, B) in right L4–5 neural foramen at same level (B). C, Delayed T1-weighted fat-saturated image with intrathecal gadolinium confirms extradural CSF (arrow) at this level. Patient was treated with transforaminal epidural fibrin patch that relieved symptoms.
Therefore, specialized 3D heavily T2-weighted fat-saturated spine MRI protocols should be used routinely in the workup of potential underlying SIH. At my institution, we use a Siemens Healthcare protocol with coronal fat-saturated HASTE images with 256 echo train length, 0.9-mm3 isotropic resolution, and TR/TE of 8000/271. These images are reformatted in sagittal and axial planes, reformatted into a coronal volumetric maximum intensity projection, and supplemented with sagittal STIR sequences at each spinal level. The entire protocol encompassing the cervical, thoracic, and lumbar spine is performed in approximately 40 minutes.
If a fluid collection is identified, dynamic myelography using digital subtraction or CT techniques can precisely locate the leak, allowing percutaneous or surgical treatment. If no extradural fluid collection is present, dynamic myelography can be used to localize CVF. Supplementary MR myelography with intrathecal gadolinium can also be used to localize slowly leaking dural defects and meningeal diverticula.
A large epidural fluid collection with a substantial ventral component almost always suggests an underlying ventral dural defect, often caused by a bony osteophyte. In contrast, epidural fluid collections that have a minimal ventral component but a greater posterolateral component are often caused by ruptured nerve root sleeves or meningeal diverticula [14] (Fig. 3).
Fig. 3—14-year-old boy with sudden-onset orthostatic headache after playing golf. A, Sagittal contrast-enhanced T1-weighted MR image shows sagging of brainstem, dural venous sinus, and pituitary engorgement. B, Axial reconstruction of 3D T2-weighted fat-saturated MR image of spine shows epidural fluid collection confined to dorsal and lateral epidural spaces at T10 level (arrows) without ventral component. C and D, Axial (C) and coronal (D) slices through left lateral decubitus dynamic CT myelography show pooling of contrast material along lateral epidural space at T10–11 (arrows), arising from ruptured T10 nerve root sleeve. E, Intraprocedural CT image obtained during CT-guided epidural fibrin glue patching shows percutaneous epidural injection of fibrin and autologous blood. Treatment provided only temporary relief, so patient underwent primary surgical repair.
This distinction is important, because it will dictate patient positioning during dynamic myelography. Thus, the presence and location of epidural fluid collection should be described in the radiology report.
In the absence of epidural fluid collection, the radiologist should report the presence, overall burden, location, and laterality of meningeal diverticula in the spine, because meningeal diverticula are often the nidus of CVF. An asymmetric burden of meningeal diverticula may inform initial patient positioning in dynamic myelography. Additional supplementary findings include any large osteophytes (even in the absence of epidural fluid collection) or enlargement of the thecal sac, which may reflect underlying dural ectasia.
Dynamic Myelography
What distinguishes dynamic from conventional myelography is the timing of imaging and the use of provocative maneuvers such as patient elevation, pressure augmentation, and inspiration to increase conspicuity of CVF [15, 16]. Conventional myelography is often performed in two parts, with the injection of intrathecal iodinated contrast material (often performed under fluoroscopy) followed by whole spine CT after a delay to allow diffusion of contrast material throughout the thecal sac and delineation of the entire subarachnoid compartment. In contrast, dynamic myelography is performed to identify fast, transient egress of CSF into a paraspinal vein laterally. Immediate imaging is obtained after injection of contrast material with the patient in the lateral decubitus position so that contrast material layers along the meningeal diverticula where most CVF tend to arise. Dynamic myelography can be performed with either CT (CTM) or digital subtraction (DSM) techniques. DSM has high temporal resolution but suffers from lack of simultaneous whole spine imaging and is susceptible to motion, superimposition, and breathing artifacts, often requiring general endotracheal anesthesia for technical success. In contrast, dynamic CTM does not require general anesthesia, acquires simultaneous whole spine imaging, and has high spatial localization, allowing optimal treatment planning. DSM may not be available at many institutions; therefore, this chapter discusses dynamic CTM technique in detail. Procedural details of DSM have been published [17].
When an extradural collection is present, the patient will be either prone in case of a suspected dural defect or decubitus when a fast leak from a ruptured meningeal diverticulum or ruptured nerve root axilla is suspected. When CVF is suspected, the patient is placed in the decubitus position.
After intrathecal access is achieved with a spinal needle and iodinated contrast material is injected into the subarachnoid space (5–10 mL of 300 osmolar iodinated contrast material), the patient’s hips are elevated with a foam wedge or inflatable air transfer mattress. When a foam wedge is used, the patient is positioned on the device from the outset, and whole spine CT is performed immediately after injection of contrast material, but because the patient is not in a horizontal position, opening pressure cannot be measured, and thus pressure cannot be reliably manipulated with intrathecal saline infusion. When an inflatable mattress is used, after accessing the subarachnoid space, opening pressure can be measured with a digital manometer and, as long as pressure is normal or low, subsequently augmented with 5-mL aliquots of sterile saline, with repeat measurements after saline infusion to a maximum of approximately 30 cm of water. Subsequently, contrast material is injected, the needle is removed, the device is inflated for approximately 10 seconds, deflated, and then whole spine CT is initiated. In addition, studies have shown that patient inspiration during imaging can increase conspicuity of CVF, presumably lowering central venous pressure and facilitating CSF moving across the fistula [15]. Rehearsing timing of inspiration with the patient before the procedure can be useful to avoid technical failure.
Once whole spine CT is initiated, at least two whole spine acquisitions phases should be performed in succession to maximize temporal resolution. Multiphase acquisition allows scrutinization of paraspinal densities over time, as CVF often fills transiently on a single phase of acquisition (Fig. 4).
Fig. 4—62-year-old woman with orthostatic headache. A, Axial early phase image of right lateral decubitus pressure-augmented dynamic CT myelogram shows filling of small paraspinal vein (arrow) lateral to perineural cyst at T11–12 level. B, Delayed-phase MR image shows contrast material dissipated from vein (arrow), consistent with CSF venous fistula.
Side-by-side comparison of dynamic CT images with preprocedural 3D heavily T2-weighted fat-saturated spine MRI helps distinguish partial filling of perineural cysts from CVF (Fig. 5).
Fig. 5—42-year-old man with orthostatic headaches. A, Axial decubitus dynamic CT myelogram shows irregular contrast enhancement in right T12-L1 neural foramen (arrow). B, Axial heavily T2-weighted fat-saturated 3D MR image with CSF leak protocol at same level delineates irregular perineural cyst (arrow), confirming contrast pattern seen in A reflects partial filling of distal portion of perineural cyst rather than CSF venous fistula.
After multiphase whole spine CT is performed in the lateral decubitus position, the patient may be placed in the contralateral decubitus position for one final image, which may reveal a contralateral fistula. Because sensitivity for detecting CVF is highest on the first injection and early phase of imaging, dynamic myelography is traditionally performed in two sessions, one for each laterality. However, some centers have had success leaving the needle in place during patient repositioning, allowing a second injection to complete the contralateral image [18]. Potential concerns with this procedure are excessive needle motion and exacerbation of an iatrogenic dural puncture–related leak. When we perform same-day bilateral decubitus myelography, the needle is either retracted into the ligamentum flavum before repositioning or the needle is removed and a second puncture is performed after repositioning. In patients with underlying connective tissue disease or who may be susceptible to post–dural puncture headache, prophylactic same-day epidural blood or fibrin glue patching at the site of puncture can be performed.
In contrast to CVF localization, pressure augmentation and inspiration maneuvers are not necessary when locating fast leaks from a violation of the ventral or lateral dura. After injection of contrast material into the subarachnoid space, the patient’s hips are elevated and rapid whole spine imaging is performed. Images should be scrutinized for where contrast material first moves from the subarachnoid to the epidural space, filling the epidural fluid collection or lateral epidural space (Fig. 6).
Fig. 6—72-year-old woman with orthostatic headaches. A and B, Axial (A) and sagittal (B) T2-weighted MR images through thoracic spine show ventral epidural fluid collection extends from T1 to T6 (arrows). C, Sagittal prone early-phase dynamic myelogram shows filling of ventral epidural fluid collection at C7-T1 level with dense contrast material (solid arrow), while more inferior component of collection (dashed arrow) has not yet filled, suggesting that dural defect is at C7-T1 level.
Regardless of technique, all spinal access should be attempted with a noncutting, pencil point sidehole spinal needle, rather than a traditional cutting spinal needle, which has been shown to minimize the risk of post–dural puncture headache [19].
In cases of high pretest probability (i.e., positive brain MRI and/or highly suspicious clinical symptoms), dynamic myelography may be repeated several times to discover the underlying CVF. Repeated procedures must be weighed against the risk of radiation and multiple dural punctures for a given patient. In patients undergoing repeat dynamic myelography, we may consider concurrent infusion of 0.2 mL intrathecal gadolinium (gadobenate dimeglumine 0.5 M; MultiHance, Bracco) to perform delayed, pressure-augmented MR myelography to potentially reveal a slowly leaking dural defect or meningeal diverticulum. We perform MR myelography using a multiplanar T1-weighted fat-saturated sequence and modified 3-point Dixon fat-suppression technique with 3-mm section thickness with 0.5-mm skip (TR/TE, 475/10; echo train length, 3–4; bandwidth, 50 Hz; matrix size, 320 in frequency-encoding direction and 224 in phase direction). After sagittal full spine acquisition, real-time monitoring is performed to prescribe additional axial and coronal planes of interest to minimize scan time while optimizing image quality.
Treatment Options
CSF Venous Fistula
Percutaneous fibrin glue embolization of CVF is a reasonable first treatment option after a CVF is identified, because it is minimally invasive and can be performed on the same day as dynamic myelography [20]. The technical details of the procedure have been described, but briefly, a 20- or 22-gauge spinal needle is advanced to the origin of the CVF under intermittent CT guidance. When the needle is in the desired position, a test injection of air or dilute contrast material is performed to confirm epidural positioning of the needle. In addition, injection of fibrin glue into the adjacent meningeal diverticulum has been reported to result in technical success without reported chemical meningitis or arachnoiditis [21]; 2–4 mL of fibrin injectate is instilled through the needle, then an image is obtained to observe the injectate spread pattern.
We routinely perform anticipatory fiducial marker placement during fibrin glue injection to facilitate easy relocalization in case of a repeat procedure or subsequent surgery or endovascular treatment. If the first fibrin glue embolization is unsuccessful, a second attempt may be made prior to surgical or endovascular referral. Patients receiving a repeat fibrin injection should be premedicated with 50- mg oral diphenhydramine 30 minutes before the procedure to minimize potential for an allergic reaction. Fibrin glue is a biosynthetic material made from reconstituted human blood components and contains aprotinin, which has been associated with allergic reactions.
At my institution, patients who do not respond to percutaneous fibrin glue embolization are referred for either endovascular embolization or surgical ligation, depending on the patient’s preference and risk tolerance. Surgical ligation of CVF is considered definitive and has been performed the longest of the treatment modalities; however, it is the most invasive treatment option and many patients prefer to avoid surgery if possible. When undergoing endovascular embolization, access to the culprit paraspinal vein is achieved via the azygos or hemiazygos via the internal jugular or femoral vein. After the correct paraspinal vein is catheterized, embolization may be performed with either a liquid embolic system (Onyx, Medtronic) or N-butyl-cyanoacrylate.
Dural Defects and Meningeal Diverticula
First-line treatment of dural defects and leaking meningeal diverticula is targeted epidural blood and/or fibrin glue patching. The epidural space can be accessed via dorsal interlaminar or transforaminal approaches depending on the type of leak. In dorsal interlaminar approaches, a loss of resistance technique using air can be performed to ideally position the needle in the epidural compartment, whereas in transforaminal approaches, epidural position can be confirmed with injection of a small amount (approximately 0.5 mL) of dilute iodinated contrast material to observe epidural spread of injectate. As many dural defects are ventral, far lateral transforaminal approaches can be used to attempt to access the ventral epidural space (Fig. 7).
Fig. 7—45-year-old man with orthostatic headaches and confirmed ventral dural defect at T1-2 level. A and B, Sequential axial CT slices obtained during epidural blood patching show far lateral transmuscular approach using 15-cm spinal needle (arrow) to reach ventral epidural space at T1-2 level.
After treatment, patients should be monitored for resolution of symptoms and repeat imaging performed to ensure resolution of brain findings and epidural fluid collection. Persistent evidence of an epidural fluid collection even in the context of symptom resolution may require surgical treatment, because a chronic dural defect increases the risk of hemosiderosis, which causes its own clinical syndrome and is largely irreversible.
Patients Without a Localized Leak or Fistula
Patients with suspected SIH in whom no leak or fistula is identified on dynamic myelography present a management challenge, particularly if their first-line brain and spine MRI did not show findings of SIH. In these patients, empirical multilevel epidural blood patching is offered for both potential therapeutic and diagnostic purposes. Patients with a strong but temporary clinical response to patching may warrant repeat dynamic myelography. In patients without a clinical response to empirical patching, alternative diagnoses may be considered. My institution has established a multidisciplinary conference consisting of neuroradiologists, neurologists, and neurosurgeons to discuss management of these and other patients to coordinate and optimize care.
SIH is an increasingly recognized, debilitating clinical syndrome for which radiologists have an opportunity to play a key role in diagnosis and treatment. By implementing specialized first-line MRI protocols and dynamic myelography techniques, radiologists can optimize clinical outcomes in this patient population.
References
Kranz PG, Luetmer PH, Diehn FE, Amrhein TJ, Tanpitukpongse TP, Gray L. Myelographic techniques for the detection of spinal CSF leaks in spontaneous intracranial hypotension. AJR 2016; 206:8–19
Schievink WI, Moser FG, Maya MM. CSF-venous fistula in spontaneous intracranial hypotension. Neurology 2014; 83:472–473
Callen AL, Timpone VM, Schwertner A, et al. Algorithmic multimodality approach to diagnosis and treatment of spinal CSF leak and venous fistula in patients with spontaneous intracranial hypotension. AJR 2022; 219:292–301
Mokri B. The Monro-Kellie hypothesis: applications in CSF volume depletion. Neurology 2001; 56:1746–1748
Schievink WI, Maya MM, Louy C, Moser FG, Tourje J. Diagnostic criteria for spontaneous spinal CSF leaks and intracranial hypotension. AJNR 2008; 29:853–856
Payer M, Sottas C, Bonvin C. Superficial siderosis of the central nervous system: secondary progression despite successful surgical treatment, mimicking amyotrophic lateral sclerosis—case report and review. Acta Neurochir (Wien) 2010; 152:1411–1416
Kranz PG, Gray L, Amrhein TJ. Spontaneous intracranial hypotension: 10 myths and misperceptions. Headache 2018; 58:948–959
D’Antona L, Jaime Merchan MA, Vassiliou A, et al. Clinical presentation, investigation findings, and treatment outcomes of spontaneous intracranial hypotension syndrome: a systematic review and meta-analysis. JAMA Neurol 2021; 78:329–337
Kranz PG, Amrhein TJ, Choudhury KR, Tanpitukpongse TP, Gray L. Time-dependent changes in dural enhancement associated with spontaneous intracranial hypotension. AJR 2016; 207:1283–1287
Dobrocky T, Grunder L, Breiding PS, et al. Assessing spinal cerebrospinal fluid leaks in spontaneous intracranial hypotension with a scoring system based on brain magnetic resonance imaging findings. JAMA Neurol 2019; 75:580–587
Schievink WI, Schwartz MS, Maya MM, Moser FG, Rozen TD. Lack of causal association between spontaneous intracranial hypotension and cranial cerebrospinal fluid leaks. J Neurosurg 2012; 116:749–754
Magnaes B. Body position and cerebrospinal fluid pressure. Part 2. Clinical studies on orthostatic pressure and the hydrostatic indifferent point. J Neurosurg 1976; 44:698–705
Madhavan AA, Verdoorn JT, Shlapak DP, et al. Lateral decubitus dynamic CT myelography for fast cerebrospinal fluid leak localization. Neuroradiology 2022; 64:1897–1903
Amrhein TJ, Gray L, Malinzak MD, Kranz PG. Respiratory phase affects the conspicuity of CSF–venous fistulas in spontaneous intracranial hypotension. AJNR 2020; 41:1754–1756
Caton MT, Laguna B, Soderlund KA, Dillon WP, Shah VN. Spinal compliance curves: preliminary experience with a new tool for evaluating suspected CSF venous fistulas on CT myelography in patients with spontaneous intracranial hypotension. AJNR 2021; 42:986–996
Schievink WI, Moser FG, Maya MM, Prasad RS. Digital subtraction myelography for the identification of spontaneous spinal CSF-venous fistulas. J Neurosurg Spine 2016; 24:960–964
Carlton Jones L, Goadsby PJ. Same-day bilateral decubitus CT myelography for detecting CSF-venous fistulas in spontaneous intracranial hypotension. AJNR 2022; 43:645–648
Philip JT, Flores MA, Beegle RD, Dodson SC, Messina SA, Murray JV. Rates of epidural blood patch following lumbar puncture comparing atraumatic versus bevel-tip needles stratified for body mass index. AJNR 2022; 43:315–318