
At some point of inflection, every new imaging modality will require its own image-guided biopsy capabilities. Why? Because as Haydee Ojeda-Fournier, MD, of UC San Diego Health reminded us in her ARRS Quick Byte video, suspicious findings may be occult on all other systems.
Yes, and … Contrast-enhanced mammography (CEM) is transitioning from diagnostic instrument to a functional intervention platform—addressing Dr. Ojeda-Fournier’s “what next?” query for findings seen only on recombined images.
Percentage Points:
- 62% of CEM-detected lesions can be identified during a second look at digital breast tomosynthesis (DBT).
- 76% of CEM findings have an ultrasound correlate; these correlates are more likely to be malignant.
- ~60% of MRI-guided biopsies could potentially be performed via CEM, providing a faster, lower-cost alternative for impacted MR units.
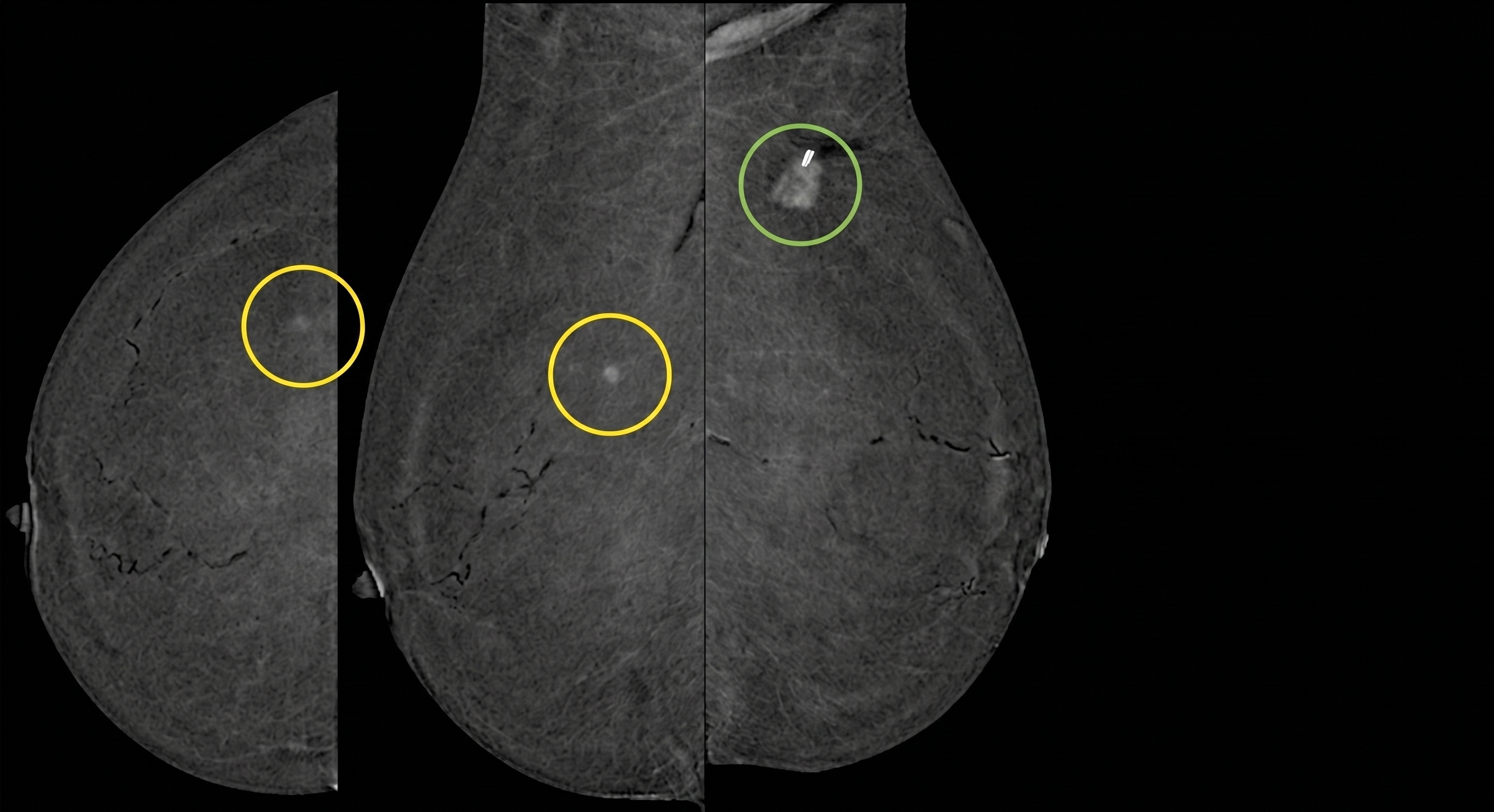
Case in Point: CEM-guided intervention remains a game-changer for patients who cannot tolerate MRI. For example, in the 83YO patient above with invasive lobular carcinoma who was not an MRI candidate, CEM-guided localization successfully targeted a contralateral mass that was mammographically and sonographically occult.
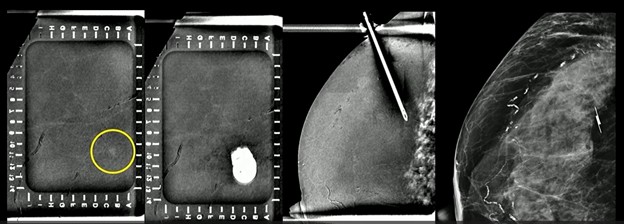
In the projection below, you’ll notice some artifact from the needle. And after Dr. Ojeda-Fournier’s team deployed their wireless localizing device (based on geography), pathology came back benign. She’ll need a follow up, regardless.
Final Points of Order:
- Search in Teams: Using a combined scout (CEM+DBT) provides the most flexibility for choosing the optimal guidance modality.
- Needle Up! While both horizontal and vertical approaches are possible, typically, the vertical needle approach is preferred because it samples a larger tissue volume in the z-axis and is less reliant on precise depth estimation.
- Singular Sensation: A successful biopsy is defined as obtaining tissue within one procedure under a single compression, whether guided by recombined CEM, DBT, or stereotactic techniques.
Leave a Reply