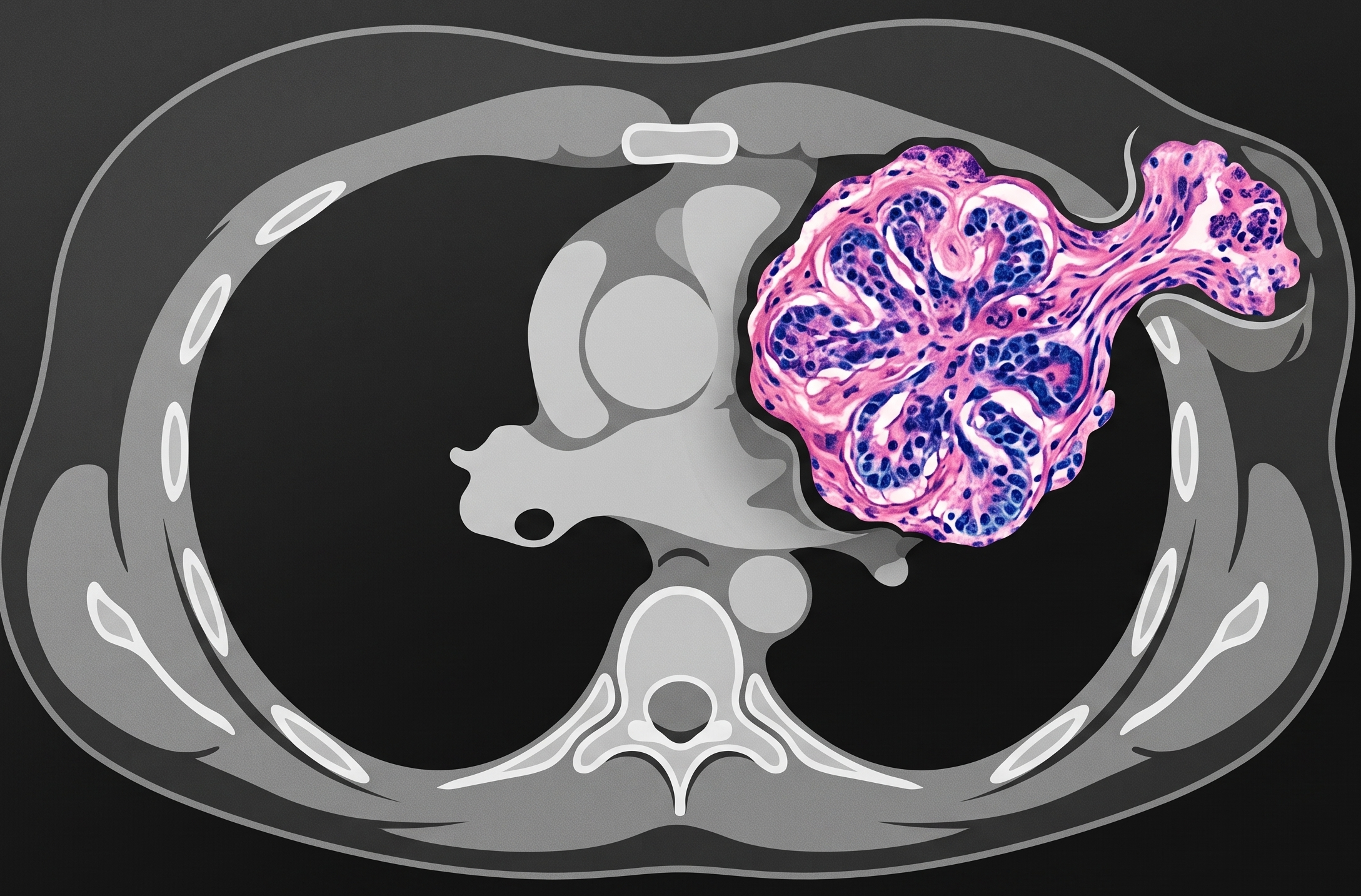
Congratulations to Ayelet Beilin, BA, of Montefiore Medical Center at Albert Einstein College for taking home Best Oral Presentation Abstract in Breast Imaging during ARRS 2026. This research on breast cancer detection with contrast-enhanced CT with histologic correlation from Beilin and her colleagues at St. John’s Riverside Hospital in Yonkers suggests “liver windows” significantly improve the accuracy of spotting incidental breast cancer on scans.
Frame of Mind: Mammography remains the gold standard; incidental findings on CT are common. To wit, optimizing the window setting helps rads differentiate actual masses from background noise, reducing unnecessary anxiety and follow-up.
By the numbers:
8%—False-positive rate when using liver windows.
15%—False-positive rate using standard soft-tissue windows.
98%—Rads who preferred using liver windows or a combination of both settings.
RadFYI: Switching to liver windows during CT interpretation can cut false positives nearly in half—without significantly increasing false negatives.
To quote James Carville, “it’s the economy, stupid.” And when it is done correctly, imaging screening can be a financial powerhouse that balances upfront costs against the massive societal and systemic expenses of late-stage disease.
RadROI: As Lyndon Luk, MD, broke it all down during the ARRS Online Course “Early Detection and Screening with Abdominal Imaging,” health economists use the incremental cost-effectiveness ratio (ICER)—primarily measured in Quality-Adjusted Life Years (QALY), where 1 QALY represents 1 year of perfect health.
$100,000 = the standard threshold per QALY to determine if a treatment is cost-effective.
$16,854 = the remarkably low cost per QALY for abdominal aortic aneurysm screening, making it a “pretty good deal” Dr. Luk said.
Down$tream: Sure, a screening ultrasound may have low reimbursement (or even operate at a loss), but it does serve as a gateway for revenue further down the pike. And identifying a chronic process or cancer triggers a cascade of high-cost diagnostic, procedural, and therapeutic services.
VA Example: Over a decade, screening 20,000 veterans cost $2.8 million (143 per ultrasound). However, the resulting repairs and follow-up for the 1% who met criteria generated nearly $10 million in revenue.
Failure Costs: An emergency repair for a ruptured aneurysm can exceed $124,000, compared to $43,000 for a planned endovascular repair.
We Live in a Society! Managing untreated chronic conditions and advanced cancers carries a staggering economic toll.
In 2015, cancer deaths caused $94 billion in lost earnings in the U.S. alone—a figure estimated to be significantly higher in 2026.
3 of the top 5 cancers responsible for lost productivity are abdominopelvic, directly within rads’ purview.
RadFYI: As radiology inches ever closer toward opportunistic screening, radiologists can position themselves as central figures in creating a healthier society by instituting early treatment strategies that improve survival writ large.
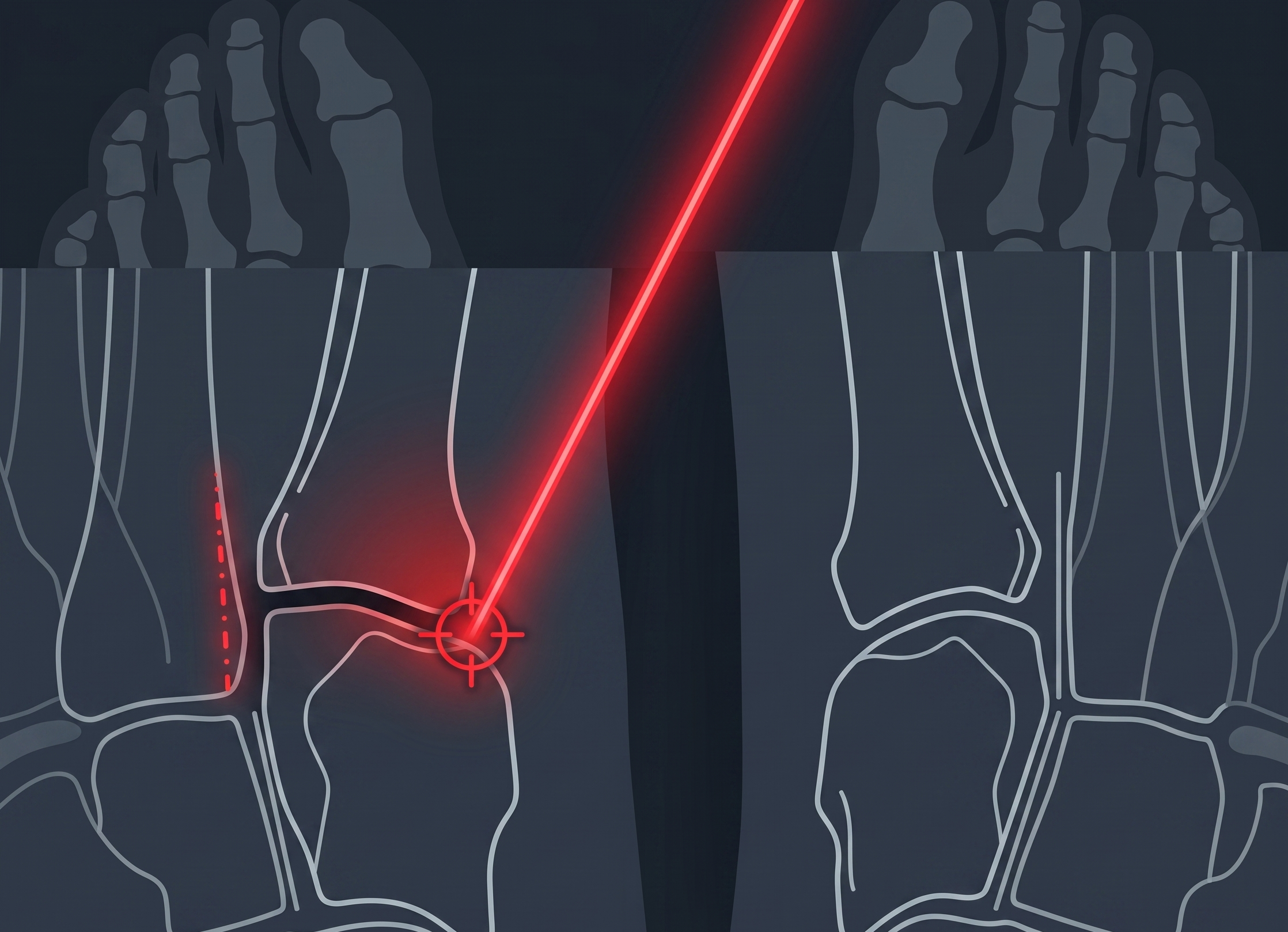
Lisfranc injuries are notoriously easy to miss; 20% of cases are overlooked on initial clinical exams. Failure to diagnose these injuries often leads to high morbidity and long-term post-traumatic osteoarthritis.
Case in Point: In the case of a 22-year-old female soccer player presented by Uma Thakur, MD, as part of the ARRS Online Course “Mastering Radiology: A Comprehensive Board Review Part 2,” a very subtle injury was missed because the alignment offset was extremely slight:
2nd TMT Malalignment—Look for even a minute step-off between the second metatarsal base and the second cuneiform.
Fleck Sign? This is a critical diagnostic pearl representing an osseous avulsion of the distal Lisfranc attachment site at the second metatarsal base.
Widening—Look for increased space between the first and second metatarsal bases.
Weight-Bearing is Mandatory! Non-weight-bearing films are a major pitfall. If you suspect an injury, always recommend weight-bearing views and compare them to the contralateral side to reveal instability.
Get quick, scannable info in your inbox each week.
RadFYI: Escalate to CT to identify occult metatarsal base fractures that are invisible on radiography. Once identified, prompt orthopedic consultation is necessary for management.
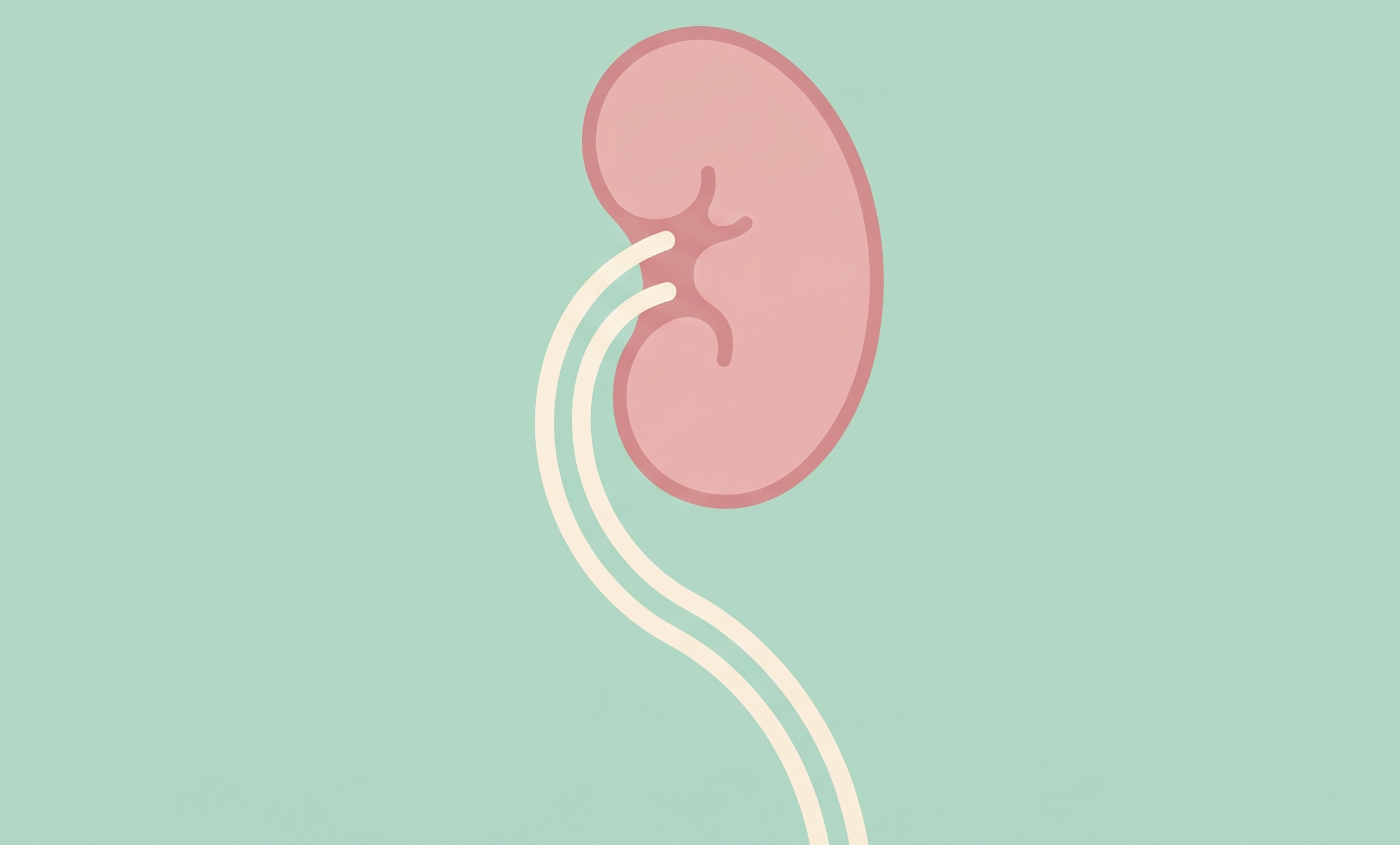
Duplicated collecting systems are the most common congenital urinary tract anomaly. While partial duplications (i.e., bifid ureters) are frequent, typically, complete ureter duplications follow a predictable, um, “vowel-forward” rule.
Case in Context: During his talk on renal and urothelial stones, strictures, mimics, and more for the ARRS Longitudinal Course “Mastering Genitourinary Imaging & Interventions,” Dan Souza, MD, introduced us to a 25YO female with left flank pain. Imaging revealed a dilated upper moiety and ureter inserting ectopically and inferiorly—resulting in significant upstream hydroureteronephrosis.
Weigert-Meyer: This rule defines the relationship between those two moieties in a complete duplication:
Upper Pole: The ureter inserts inferomedial to the lower pole ureter. It is almost always associated with an ectopic insertion and a ureterocele, making it highly prone to obstruction.
Lower Pole: Inserting superolateral to the upper pole ureter, this moiety is classically more prone to vesicoureteral reflux.
RadFYI: Use what Dr. Souza dubbed the “Vowels-Meyer Rule” to help recall the specific insertion patterns and their associated pathologies: upper, inferior, ectopic, obstruction, ureterocele.
Congratulations to Numaan Dogar, MS, and colleagues for taking home Best Oral Presentation Abstract in Emergency Imaging during ARRS 2026! Assessing frailty is crucial for trauma triage; however, the gold standard psoas muscle isn’t visible if abdominal imaging isn’t performed.
Cervicofacial Correlation: Dogar et al. showed that cervicofacial muscles—masseter and sternocleidomastoid (SCM)—are reliable surrogates for sarcopenia.
Male & Masseter: In men, the masseter index was highly predictive of sarcopenia (AUC 0.79).
Better Together: Combining masseter and SCM indices increased diagnostic accuracy (r = 0.56).
Riskier, Earlier: These markers allow for earlier risk stratification using only head or C-spine CT.
RadFYI: While the correlation was strongest in men, the SCM in women still showed a modest AUC of 0.69—suggesting potential for broader use.
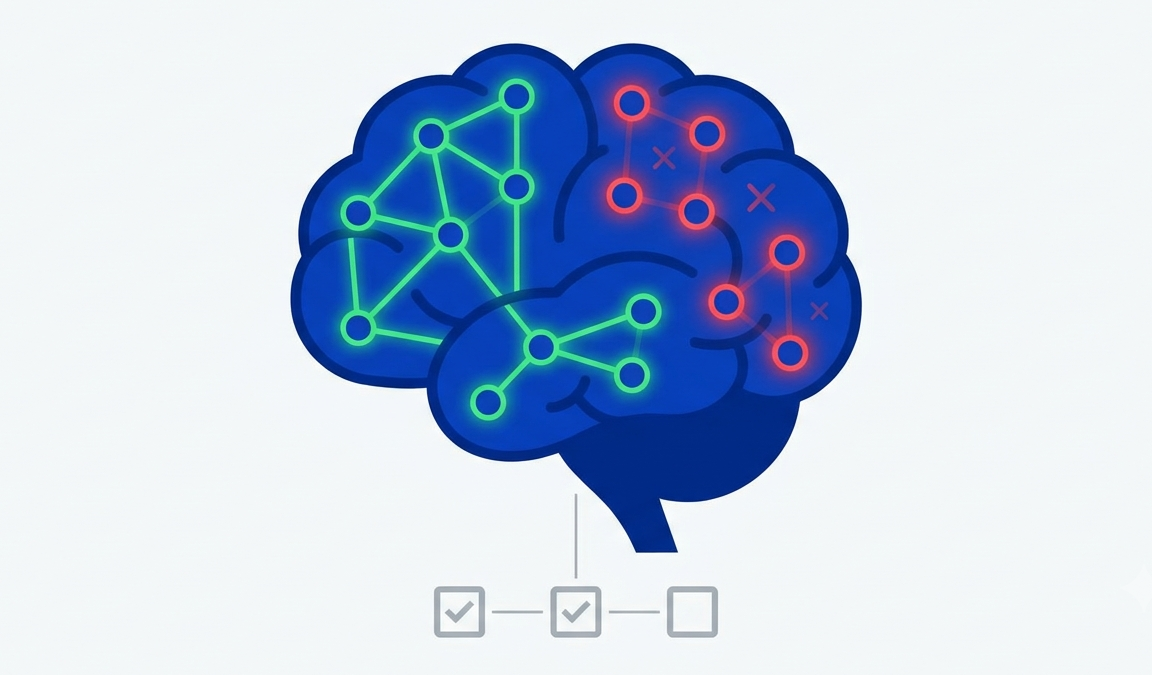
Designing a successful clinical fMRI program requires a balance between technical precision, patient-centered flexibility, and operational efficiency. Clinical fMRI can provide critical maps for surgical planning, but as 2025 ARRS Scholar Luca Pasquini, MD, clarified during ARRS 2026, its success depends on real-time quality assurance and the ability to adapt to patient limitations.
Real-Time Monitoring—Don’t wait for post-processing to check data quality.
No Shoes! Ensure patients are barefoot if performing foot-wiggling motor tasks.
Covert Language: For these tasks, monitor the pre-supplementary motor area, as it correlates highly with language planning and task compliance.
Signal Validation: Use real-time depictions to determine if the patient is actually performing the task before the scan ends.
Performance Management—Patient distress, claustrophobia, or cognitive impairment (e.g., chemo brain) can compromise data.
Fail Once: At Yale, Dr. Pasquini’s team allows for one failure; upon the second, they switch to low-compliance tasks or slower versions of the standard paradigm.
Modify on the Fly: Slow down word generation tasks or switch to passive story listening if a patient cannot keep up.
Sedation? Sure, bland anxiolytics can be used for task fMRI without significantly impacting the signal.
Pitfall ID—Be aware of neurovascular uncoupling, where the BOLD signal disappears—common in glioblastomas.
Breath Fix: Use breath-holding tasks to test cerebrovascular reactivity. This creates a map that can confirm if a lack of activation is a false negative caused by non-reactive vasculature.
Artifact, Check: Use susceptibility mapping to differentiate between real activation and drop-out artifacts from prior surgeries or hemorrhages.
Tech Woes—As Dr. Pasquini duly noted, your choice of software impacts both utility and billing alike.
Compatibility: Ensure output is compatible with surgical navigation systems à la BrainLab.
Flexibility: Opt for thin client software over hardwired licenses to avoid being tethered to a single workstation.
Clear to Code: Software must be FDA cleared and capable of processing task fMRI to be billable.
RadFYI: If a patient is incapable of performing, you must know when to stop the acquisition to maintain your admin’s “vision of value,” as well as to avoid wasting scanner slots.
Congratulations to Samuel Brody, MS, and his colleagues at Penn State College of Medicine in Hershey for taking home Best Oral Presentation Abstract in Thoracic Imaging during ARRS 2026.
Brody et al.’s research reveals that for patients with empyema, the timing of a CT scan can actually be a matter of life and death. Getting a scan on the same day as ER admission significantly improves outcomes, compared to waiting just 1–3 days.
By the Numbers: A study of 4,500 patients showed that early (i.e., same-day) CT led to:
51% lower mortality hazard;
34% reduced risk of invasive surgery;
25% lower ventilator requirement.
The Catch? Although early imaging improved survival, it was associated with a 37.5% rise in all-cause ER readmissions, albeit subsequent readmission frequency remained similar to the late group.
RadFYI: Diagnostic delays allow for fibrous septations to form, making treatment that much harder. Implementing same-day CT protocols in the ER could be a game-changer for reducing mortality and invasive procedures.
New insight from ARRS 2026 would suggest that weight loss from glucagon-like peptide-1 (GLP-1) receptor agonists may well be “healthy”—mirroring the body composition changes seen in exercise, rather than pathological wasting.
Laying Waste: As semaglutide use explodes, indeed, rads are observing significant shifts in CT-based body composition. Understanding whether muscle loss is a clinical concern or a byproduct of healthy weight reduction remains critical for accurate reporting.
Concerns continue to circulate vis-à-vis muscle loss in patients on GLP-1 therapy; however, as Perry J. Pickhardt, MD, previewed during “Opportunistic Screening with Imaging,” the impending publication of a large, multicenter trial analyzing intrapatient CT changes indicates such concerns could be overstated.
Liver Detox: Patients show significantly smaller and less fatty livers, indicating a direct hit to metabolic syndrome.
Quality > Quantity: While muscle volume may decrease slightly, quality often improves via reduced myosteatosis.
Exercise Parallel: The fat loss (both visceral and subcutaneous) categories look nearly identical to weight loss achieved through healthy exercise.
Cachexia: No, GLP-1 weight loss doesn’t mirror the scary signatures of disease-driven muscle attenuation.
RadFYI:Retrospective studies show that even when patients lose weight, their metabolic profile—that ratio of fat to lean tissue quality—moves in a positive direction. And this reassuring data seems to suggest that GLP-1-induced weight loss may simply be a metabolic shift, rather than a muscular crisis.
The 2024 update to the McDonald criteria formally integrated the central vein sign (CVS) and paramagnetic rim lesions (PRL) as optional diagnostic markers for multiple sclerosis (MS). These markers offer high specificity, helping to differentiate MS from mimics, à la small-vessel ischemic disease.
Pro Tip: While many protocols suggest adding a T2-FLAIR or specialized SWI sequence, as Joshua P. Nickerson, MD, tipped us off during ARRS 2026, you can often visualize the CVS using existing 3D data and your PACS vendor’s MPR tool.
Process—Load a 3D SWI image in the MPR tool, then right-click and drag a 3D FLAIR image on top of it to create a composite map.
Benefit—Using a slider bar to blend the two images allows you to confirm if a vessel is centrally located within a T2 hyperintensity…without adding length to your clinical protocol.
More From McDonald ‘24:
Optic Nerve: Now recognized as a fifth topographic site for assessing dissemination in space (DIS).
Rule of 6: Identifying 6 or more CVS-positive lesions can substitute for dissemination in time (DIT) criteria.
CSF Markers:Kappa free light chains are an approved substitute for DIT, providing a quantitative alternative to traditional oligoclonal bands.
Stricter Thresholds: For patients over 50 (or those with vascular risk factors), a diagnosis now strongly recommends the presence of a spinal cord lesion, CSF positivity, or at least 6 CVS-positive lesions.
RadFYI: Imagers should transition to structured reporting that includes the count of CVS-positive lesions, as well as PRLs. Whereas 3T is preferred for detecting these subtle markers, creative use of PACS post-processing may help you satisfy the latest standards.
Recognizing the radiographic progression of congestive heart failure (CHF) is essential for identifying the severity of pulmonary edema and guiding clinical intervention. As Matthew D. Cham, MD, pointed out during the ARRS Online Course “Comprehensive Insights into Heart and Lung Transplant Imaging,” imaging findings correlate directly with increasing hydrostatic pressure—evolving from simple cardiac enlargement to life-threatening alveolar edema:
Early Stage: Often, the only visible finding is cardiomegaly, while the lung fields remain clear and free of effusions.
Interstitial Edema: As pressure rises, signs of interstitial fluid appear. Look for lung markings, as well as peribronchial cuffing and Kerley B lines.
Alveolar Edema: This advanced stage presents as perihilar airspace disease and pleural effusions. On CT, this may manifest as diffuse ground-glass opacification.
RadFYI: In cases of severe alveolar edema, the fluid often settles in a typical perihilar distribution known as the batwing pattern. Moreover, chronic CHF can lead to additional systemic findings, including pericardial effusions, mediastinal lymphadenopathy, as well as ascites.
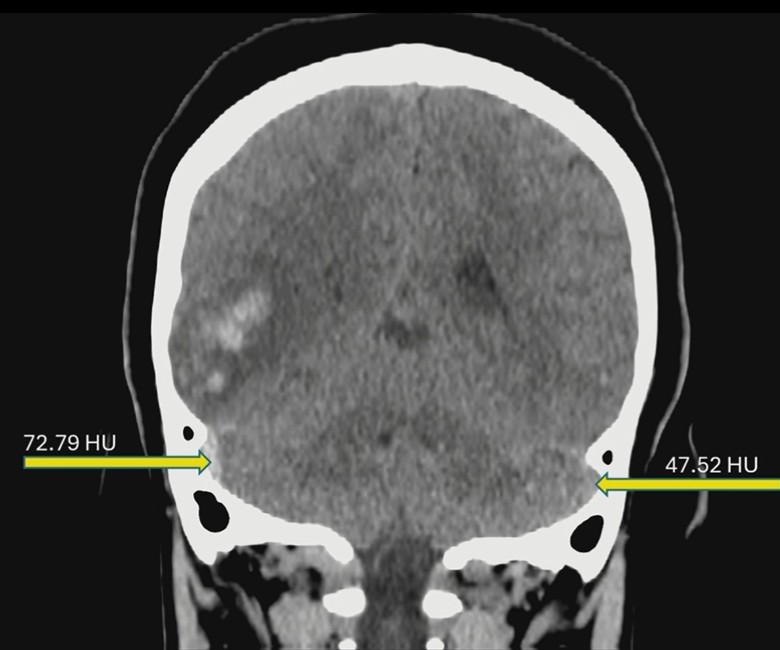
Sure, you’ll read a non-contrast head CT for headaches every day. But as Harprit S. Bedi, MD, reminded us during ARRS 2026, the rad’s real art lies in identifying dural venous sinus thrombosis (DVST)…before that CTA is even ordered.
DVST Dx: Symptoms of DVST can be insidious or acute, often presenting in high-risk patients (e.g., on oral contraceptives or experiencing pain worsened by valsalva). Since missing those subtleties can delay treatment for intracranial bleeds and venous congestion, look for these on that non-contrast CT:
Hyperdensity: Typically, a thrombosed sinus measures >66 Hounsfield units (HU).
73 HU—The thrombosed sigmoid sinus in Bedi’s case above, compared to 47 HU in normal vessels.
Three Signs:
Triangle—Check for increased density in the dural sinuses.
Cord—Look for hyperdense cortical veins.
Empty Delta—Classic, if patient proceeds to a CTA.
HU/Hematocrit Ratio: This tool can help differentiate true thrombosis from hemoconcentration, particularly in anemic patients.
RadFYI: Don’t just look for the bleed; look for the cause. If you see parenchymal changes or a hyperdense sinus on a non-con CT, use the HU tool to increase your confidence.
Heartiest of congratulations to Dr. David DiSantis of Mayo Clinic Jacksonville on garnering Best Overall Scientific Program Oral Presentation Abstract at ARRS 2026. “GI Fluoroscopy: What Are We Still Doing?” provides a data-driven roadmap for modernizing trainee education.
Venue Change: Despite the rise of cross-sectional imaging, GI fluoroscopy remains a pillar of clinical practice—with >2.2 million procedures performed nationwide annually. However, where these procedures happen is changing. Using 2023 Medicare data, DiSantis revealed a massive disparity in procedure volumes as you move down the alimentary canal:
Swallowing studies—1,085,826
Esophagrams—551,897
Upper GI—409,174
Small bowel—152,967
Contrast enemas—74,445 (double contrast study considered “moribund” with only 15,302 performed)
Dr. DiSantis speaks during the opening ceremony of ARRS 2026 in Pittsburgh, PA.
Above the Diaphragm: >1.6 million fluoroscopic procedures are concentrated in swallowing studies and esophagrams. To ensure rads-in-training provide useful interpretations in real-world practice, residency programs must shift their emphasis to areas “above the diaphragm.”
RadFYI: Training must follow the volume. This award-winning research proves that mastering the upper GI tract is the most critical skill set for the modern rad performing fluoroscopy.