Matthew Lee and Luca Pasquini Receive 2025 ARRS Scholarships
The American Roentgen Ray Society (ARRS) is pleased to announce two 2025 ARRS Scholarships have been granted to Matthew Lee, MD, at the University of Wisconsin School of Medicine and Public Health and Yale School of Medicine’s Luca Pasquini, MD, PhD.
Provided by ARRS’ own The Roentgen Fund®, the ARRS Scholarship supports early-career faculty members pursuing radiological research that promises to change how medical imaging is practiced. A two-year grant totaling $180,000, the ARRS Scholarship aims to advance emerging scholars, as well as prepare them for positions of leadership.
Drs. Lee and Pasquini were formally recognized as recipients of the ARRS Scholarship during the opening ceremony of the 2025 ARRS Annual Meeting at Southern California’s Marriott Marquis San Diego Marina.
Matthew Lee, MD, is an assistant professor of radiology in the abdominal imaging and intervention section at the University of Wisconsin School of Medicine and Public Health. He completed his medical degree, surgical internship, and diagnostic radiology residency at the University of Wisconsin School of Medicine and Public Health. Following residency, Dr. Lee served as an active-duty diagnostic radiologist in the United States Navy. Returning to the University of Wisconsin for an abdominal imaging and intervention fellowship, in 2022, he joined the faculty. Dr. Lee’s research focuses on artificial intelligence (AI) applications in abdominal imaging, “opportunistic” imaging, body composition analysis, workflow optimization, and advancing radiology’s role in population health. Having published and presented extensively on these topics, Dr. Lee is particularly interested in applying novel AI tools to radiology datasets to gain insights into disease diagnosis, risk prediction, outcomes, and health disparities—while optimizing radiology resource utilization. Committed to expanding radiology’s impact on public and population health, he is passionate about leveraging large-scale imaging data to add value through enhanced prevention, improved patient outcomes, and reduced health care costs, particularly for preventable diseases.
Luca Pasquini, MD, PhD, earned his medical degree from the University of Florence in 2014, followed by a radiology residency and a PhD in neuroplasticity at La Sapienza University in Rome—completed in 2019 and 2023, respectively. During his early career in Italy, he held neuroradiology positions at La Sapienza University and Bambino Gesù Children’s Hospital in Rome. In the United States, Dr. Pasquini advanced his career at Memorial Sloan Kettering Cancer Center (MSKCC), where he served as a research associate in the fMRI laboratory. Subsequently, he completed a Fellowship in neuro-oncology imaging and a nuclear medicine residency at MSKCC from 2020-2024. Having published more than 50 papers in peer-reviewed journals, he is internationally recognized for his contributions to the understanding of brain plasticity, earning multiple prestigious awards from leading radiological societies. Currently, he serves as assistant professor in radiology and biomedical imaging at Yale School of Medicine and as a neuroradiologist at Yale New Haven Hospital in Connecticut.
Medical schools, affiliated hospitals, and clinical research institutions with training interests in diagnostic radiology, nuclear medicine, allied sciences, or other professions fundamental to imaging techniques are invited to submit one nomination for the 2026 ARRS Scholarships. For full details, please visit ARRS.org/Scholars.
ARRS Scholar Update: Steven Rothenberg
Steven Rothenberg, MD, is in the second year of his ARRS Scholarship program, investigating methods for mitigating the nocebo effect in diagnostic reporting of lumbar spine MRI. Currently, he is recruiting for his first prospective randomized controlled clinical trial: NCT06103474. Since receiving his ARRS Scholarship during the 2023 ARRS Annual Meeting in Honolulu, HI, Dr. Rothenberg has been awarded Most Prolific Inventor by the Herbert Institute for Innovation and Entrepreneurship and the Light Bulb Award from the University of Alabama at Birmingham’s radiology department. His submission of eight invention disclosures have led to three distinct patent applications and one notice of allowance (US20240257947A1) from the United States Patent and Trademark Office. Meanwhile, Dr. Rothenberg’s research findings have yielded five co-authored published articles, two related editorials, and two AJR Original Research manuscripts presently in press. As an ARRS Scholar, thus far, he has presented 19 scientific abstracts, earning a Certificate of Merit during the 2024 ARRS Annual Meeting in Boston, MA. Dr. Rothenberg continues to donate to The Roentgen Fund to give back in support of other early-stage faculty applying for future ARRS Scholarships.
30 Radiologists Receive Grants for Clinician Educator Development Program
ARRS proudly announces the latest recipients of our longrunning Clinician Educator Development Program (CEDP) for radiologists. The CEDP Class of 2025 includes the following 30 clinical educators of medical imaging, selected from a competitive field of applicants, who have collectively received more than $40,000 in grant funding from The Roentgen Fund:
Ellen Sun Kathleen Eddy Danielle Kruse Ryan Adams Rory Cochran Maria El Homsi Sarah Beier Christopher Newman Maham Jehangir Meng (Cathy) Hao Daniel O’Neal Pat Whitworth Preethi Raghu Hyung Won Choi Iris Chen
Christine Boatright Aurela Clark Samer Soussahn Alyson Stacks Carraway Lei Yu Natalie Cain-Wisdom Rekha Krishnasarma Nicholas Voutsinas Janardhana Ponnatapura Mark Hoegger Babina Gosangi Livia Maria Kruger Nai-Wen Chang Kye Jin Park Jose Felices Farias
Each year, our CEDP recipients are selected to receive a travel grant to attend a specialized workshop during the ARRS Annual Meeting. With a curriculum offering increased proficiency in teaching skills, as well as educational activity design, the ARRS Clinician Educator Development Program remains a highly interactive day of learning. Focusing on new and emerging pedagogical tools, while improving already acquired clinical acumen, over half of this expertly curated syllabus consists of hands-on learning.
This year’s CEDP intensive was held on Saturday, April 26–the day before the 2025 Annual Meeting.
Chairpersons and directors at medical schools, affiliated hospitals, and clinical research institutions are invited to nominate two candidates per institution for the ARRS Clinician Educator Development Program. For full details, please visit ARRS.org/CEDP.
Introducing SPARC—Sparking and Promoting Academic Radiology Careers
Sparking and Promoting Academic Radiology Careers, or SPARC, is a new three-day program from ARRS designed to introduce PGY2 and PGY3 radiology residents to the many opportunities in academic radiology. The inaugural SPARC program took place Monday, April 28 through Wednesday, April 30 during ARRS 2025 in San Diego. Participants received a $1,000 stipend payable to their institution to support their involvement.
Led by course directors Ania Kielar, MD, and John-Paul “JP” Yu, MD, PhD, SPARC attendees received invaluable insights from academic radiologists on how to chart a viable career path, seek institutional employment, and even explore hybrid public-academic roles. The “freshman class” participants will also received mentorship from experienced faculty, participated in career focus groups, and learned about critical topics in the field, including the economics of academic imaging and work-life transitions and harmonization. Additionally, SPARC covered how to build a strong CV, time management tips, promotion considerations, committee involvement, and more pertinent topics. Panel discussions and professional networking will addressed the true diversity of career arcs from teaching to research to leadership.
The mission of ARRS’ SPARC program is to help ensure the future of academic radiology by exposing junior trainees to a variety of practice and career perspectives—guiding them on their journey of discovery to decide if academic imaging is indeed right for them. SPARC’s goal is to provide insight, mentorship, and career direction, which might otherwise be absent in their training curricula. All SPARC participants receive access to the ARRS Annual Meeting, including recorded content available for up to a year, extending their education beyond this program.
The American Roentgen Ray Society (ARRS) joins the radiology community in mourning the loss of Dr. Lee F. Rogers, a transformative leader, beloved educator, and devoted advocate for medical publishing. Named president of ARRS in 1988 and recipient of the 1993 Gold Medal, Dr. Rogers passed away on November 28, 2024, at the age of 90. He leaves an indelible mark on radiology and on ARRS, where his visionary leadership advanced the society’s mission of fostering excellence in radiologic education and research.
As just the 10th Editor in Chief of the American Journal of Roentgenology (AJR) from 1996 to 2004, Dr. Rogers ushered in a new era for “the yellow journal.” His editorial innovations, such as the medicolegal column by Dr. Leonard Berlin and his acclaimed Editor’s Notebook, enriched AJR as it transitioned into the digital age with advancements like AJR Online.
A look back at AJR Online in 2000—a pioneering step into the digital age, championed by Dr. Rogers during his tenure as Editor in Chief.
Reflecting on his impact, AJR’s current Editor in Chief, Andrew Rosenkrantz, MD, shared the following words:
“Lee Rogers had a tremendous influence on radiology. During his tenure with AJR, he greatly propelled the journal forward, introducing many changes that helped shape the journal into what it is today. He was an amazing educator, mentor, colleague, and friend to many throughout the field. He will be missed by those who had the chance to know him, with his legacy greatly remembered.”
Dr. Rogers’ influence extends beyond the pages of AJR through the Lee F. Rogers International Fellowship in Radiology Journalism. This Roentgen Fund fellowship invites radiologists from around the world to work closely with AJR’s Editor in Chief and publications staff, cultivating the next generation of medical journalists and enhancing the quality of radiology literature worldwide. Through this program, Dr. Rogers’ passion for academic excellence and mentorship continues to inspire radiologists to shape the future of the field. Writing Dr. Rogers’ memorial in the January issue of AJR, Ronald J. Zagoria, MD, duly noted: “Working under Lee’s guidance in the journal office, a generation of editors, authors, and reviewers now reflect his virtues” [1].
In his own Editor’s Notebook for AJR in November 2003 [2], Dr. Rogers shared his heartfelt belief in the value of participation:
“Meaningful participation is a broadening experience. You become informed, gain insights into the world about you, make new and often lasting friendships, and may have the opportunity to make significant contributions to things that are of interest and importance to you.”
ARRS honors Dr. Lee F. Rogers’ profound participation in radiology, his mentorship, and his enduring vision. His leadership and intellect will be deeply missed but remain a guiding light for all who follow in his footsteps.
ARRS is also saddened to note the passing of former president and Gold Medalist John P. Tampas of Colchester, VT. Having ably served on the ARRS Executive Council for many years, Dr. Tampas was gaveled in as president of this society during the opening ceremony of the 1982 ARRS Annual Meeting in New Orleans, LA.
ARRS is also saddened to note the passing of former president and Gold Medalist John P. Tampas of Colchester, VT. Having ably served on the ARRS Executive Council for many years, Dr. Tampas was gaveled in as president of this society during the opening ceremony of the 1982 ARRS Annual Meeting in New Orleans, LA.
Earning both undergraduate and medical degrees from his beloved University of Vermont (UVM), Dr. Tampas chaired the radiology department at his alma mater for a remarkable 26 years. In 2006, UVM endowed the Soule-Tampas Green & Gold Professorship in Radiology—a faculty-funded position named after him and predecessor, Dr. Bradley Soule.
Dr. Tampas’ medical career was marked by continuous service to his profession. In 1956-1957, he volunteered to serve as a U.S. Air Force flight surgeon in Korea and was awarded the rank of captain. A frequent contributor to AJR, he was bestowed lifetime membership in ARRS. And for his distinguished service to this society, in 1992 in Orlando, FL, Dr. Tampas received the ARRS Gold Medal.
Ruth Carlos Honored With American Roentgen Ray Society’s Gold Medal
The American Roentgen Ray Society (ARRS) proudly announces that former ARRS president Ruth C. Carlos, MD, MS, FACR, has been awarded the 2025 ARRS Gold Medal.
The highest accolade bestowed by North America’s first radiological society, the ARRS Gold Medal has been honoring illustrious service to radiology for more than four decades. The ARRS Gold Medal is awarded to physicians with a substantial record of service and who continue to render distinguished service to both the practice and science of medical imaging and its allied sciences.
Ruth Carlos was installed as the 119th president of ARRS during the 2019 Annual Meeting in Honolulu, Hawaii, succeeding Philip Costello, MD. She was honored as this year’s ARRS Gold Medalist on Sunday, April 27 during the opening ceremony of the 2025 ARRS Annual Meeting at California’s Marriott Marquis San Diego Marina.
Ruth Carlos, MD, MS, FACR, is a professor of radiology at Columbia University Irving Medical Center and associate chair of research faculty development for the department of radiology. She is a board-certified radiologist specializing in abdominal imaging.
Dr. Carlos also serves as the director of research in outcomes and care delivery for the Center for Imaging Biomarkers and Innovation in Integrated Diagnostics (CIMBID) at Columbia University Irving Medical Center.
A distinguished leader and pioneer in the field of radiology, Dr. Carlos has held several prestigious leadership positions that have shaped the direction of radiology research and practice. She is the first woman editor-in-chief of a major radiology journal, the Journal of the American College of Radiology (JACR), which guides the management and practice of radiology. She has served as president of ARRS, the Association of University Radiologists (AUR), and the Radiology Alliance for Health Services Research in Radiology. Currently, she chairs the GE AUR Research Radiology Academic Fellowship (GERRAF), a national program supporting early-stage investigators in health services research and care delivery.
Dr. Carlos’ influence extends to national policy, evidenced by her role as co-chair of the National Cancer Institute (NCI) Cancer Care Delivery Research (CCDR) Development Committee, and she lends her expertise as a thought leader to the National Academy of Medicine, the National Quality Forum, and the Joint Commission. Her wealth of expertise spans health services research and policy, health equity, and structural racism. Most recently, her work has focused on social genomics, the negative biological effects of social and economic marginalization and imaging biomarkers.
Dr. Carlos has received numerous awards and honors. She is an elected fellow of the American College of Radiology (ACR), as well as the Society of Computed Tomography and Magnetic Resonance (SCBT-MR). She has received the AUR Gold Medal, the Distinguished Educator Award from the Radiological Society of North America (RSNA), and the Stanford Medicine X Research Challenge Grand Prize. A funded investigator of the National Institutes of Health (NIH), she has been recognized for her research by induction into the Academy of Radiology Research Council of Distinguished Investigators, reflecting top 10% of all academic radiology faculty and awarding of the Paul C. Hodges Excellence Award.
Dr. Carlos received her medical degree from the University of Chicago, where she also completed her diagnostic radiology residency. She then completed an abdominal imaging fellowship at the University of Michigan in Ann Arbor. She also holds a master’s degree from the School of Public Health at the University of Michigan.
Tanya Moseley Receives American Roentgen Ray Society Distinguished Educator Award
ARRS is also proud to announce Tanya W. Moseley, MD, as the 2025 ARRS Distinguished Educator. The ARRS Distinguished Educator award recognizes outstanding individuals in the field of medical imaging who have a proven record of improving radiological education and remain committed to creating and implementing new and innovative educational activities.
ARRS’ Distinguished Educator award celebrates truly inspirational teachers—like Dr. Moseley— dedicated to education that results in improved participant performance, ultimately leading to enhanced patient outcomes. She was recognized as our 2025 Distinguished Educator during the opening ceremony of the ARRS Annual Meeting in San Diego, CA.
Newly installed ARRS president Deb Baumgarten with 2025 Distinguished Educator Tanya Moseley, and immediate past president Angelisa Paladin at the ARRS Annual Meeting at Marriott Marquis Marina in San Diego, CA.
Tanya Moseley exemplifies transformative leadership in radiology education, making her an exceptional choice for our Distinguished Educator. Following her distinguished tenure at MD Anderson Cancer Center as professor of breast imaging and breast surgical oncology, she now brings her visionary leadership to the University of Mississippi Medical Center, where she serves as vice chair of faculty development, division chief of breast imaging, and breast imaging fellowship director.
Her impact on radiology education has been both innovative and profound. As director of MD Anderson’s breast imaging fellowship program, she developed comprehensive curricula that have influenced generations of specialists. Her leadership of the Breast Imaging Technologist Continuing Education Committee demonstrated her commitment to technologist advancement, while her work as clinical image reviewer for multiple American College of Radiology accreditation programs underscores her dedication to maintaining the highest educational standards.
For more than two decades, Dr. Moseley’s contributions to the ARRS have transformed radiological education. Through her service on key educational committees and roles as case-based breast imaging chair and AJR SA-CME Consultant Editor, she has fundamentally shaped the organization’s educational direction. Her pioneering vision led to the creation of the first multi-vendor tomosynthesis certification course, demonstrating her exceptional ability to build collaborative educational programs. As architect and director of the ARRS Longitudinal Course Series, she continues to advance innovative approaches to radiology education.
Dr. Moseley’s leadership influence extends from institutional to national levels. In her role as chair of the FDA’s National Mammography Quality Assurance Advisory Committee, she helps establish national quality standards. Her leadership of both MD Anderson’s Diagnostic Imaging Council on Gender Inclusion Committee and the Society of Breast Imaging’s Inclusion, Diversity, and Equity Alliance reflects her commitment to creating a more inclusive field that elevates both trainees and faculty.
What truly sets Dr. Moseley apart is her comprehensive approach to education and leadership. Through strategic academic appointments across multiple institutions, she has created vital connections between breast imaging, surgical oncology, and clinical sciences. Her extensive committee service encompasses scientific programming, faculty achievement, quality improvement, and executive leadership, demonstrating her profound impact on medical education and practice.
Her teaching excellence has garnered prestigious recognition, including the University of Texas System Regents’ Outstanding Teaching Award and induction into the University of Texas Shine Academy of Health Science Education. Her influence reaches globally through international breast imaging observership programs and visiting professorships.
Dr. Moseley’s educational philosophy rests on seven core principles: clinical excellence in teaching, innovative program development, rigorous quality standards, interdisciplinary collaboration, dedicated mentorship, technological advancement, and an unwavering commitment to diversity and inclusion in medical education.
Her selection as ARRS Distinguished Educator recognizes a career dedicated to transforming radiology education and leadership. Dr. Moseley’s exceptional ability to combine clinical expertise with innovative teaching methods, while championing mentorship, quality, and inclusivity, makes her the ideal recipient of this honor. Her career exemplifies the highest standards of an educator-leader who shapes the future of radiology through both educational excellence and visionary leadership.
ARRS Names 2025 Honorary Member: Salvador Amézquita Pérez
Drs. Paladin, Pérez, and Baumgarten at the 2025 ARRS Annual Meeting in San Diego, CA.
And, finally, ARRS is happy to report that Dr. Salvador Amézquita Pérez, president of Sociedad Mexicana de Radiología e Imagen (Mexican Society of Radiology and Imaging), will receive honorary ARRS membership on day one of the society’s 2025 Annual Meeting in San Diego.
A distinguished army veteran and vascular and interventional radiologist with more than two decades experience in clinical practice and medical education, Dr. Pérez has chaired the radiology and imaging department at Hospital Central Militar (Central Military Hospital) in Mexico City since 2019, following his seven- year tenure as deputy department chair. He has been a prominent figure in the Mexican Society of Radiology and Imaging (SMRI), receiving the Award for Academic Excellence in 2018. Previously, Dr. Pérez served SMRI as treasurer (2018-2020) and general secretary (2020-2022). He will remain SMRI President until 2026.
ARRS looks forward to welcoming Dr. Pérez and his colleagues to the 2025 ARRS Annual Meeting in San Diego as part of the Global Exchange Featuring Mexico. The global exchange includes the ARRS-SMRI Sunday Featured Course, “Advances in Cardiac Imaging,” focused on techniques and considerations for evaluating structural heart conditions and coronary artery anomalies. This session will address non-atherosclerotic coronary artery narrowing, CT’s role in transcatheter mitral valve replacement and adult congenital heart disease, CT perfusion and FFR-CT for myocardial ischemia, as well as CT in TAVR before and after surgery.
Since its founding in 1946, SMRI has focused its mission on maintaining high levels of academic and scientific partners, while working with radiology groups across the country on annual courses and weekly, on-site ultrasound and general radiology meetings. In recent years, SMRI has organized international events with the International Society of Magnetic Resonance in Medicine and the European School of Radiology. SMRI also maintains a technical school for radiologists—the oldest and most prestigious in Mexico. Anales de Radiología México, founded in 2002, is the country’s only publication of its kind specializing in radiology.
The mission of the ARRS Global Partner Society Program is to build long-standing relationships with key leaders and organizations in the worldwide imaging community—increasing awareness of our society’s services in specific nations, while raising the stature of Global Partner Societies among ARRS members. Every year, the ARRS Annual Meeting Global Exchange incorporates one partner society into the educational and social fabric of our meeting. ARRS members then reciprocate at the partner society’s meeting that same year.
A member of the Radiology Health Equity Coalition (RHEC), ARRS continues to collaborate with RHEC on curating and disseminating trusted resources and best practices for improving access to and utilization of preventive and diagnostic imaging.
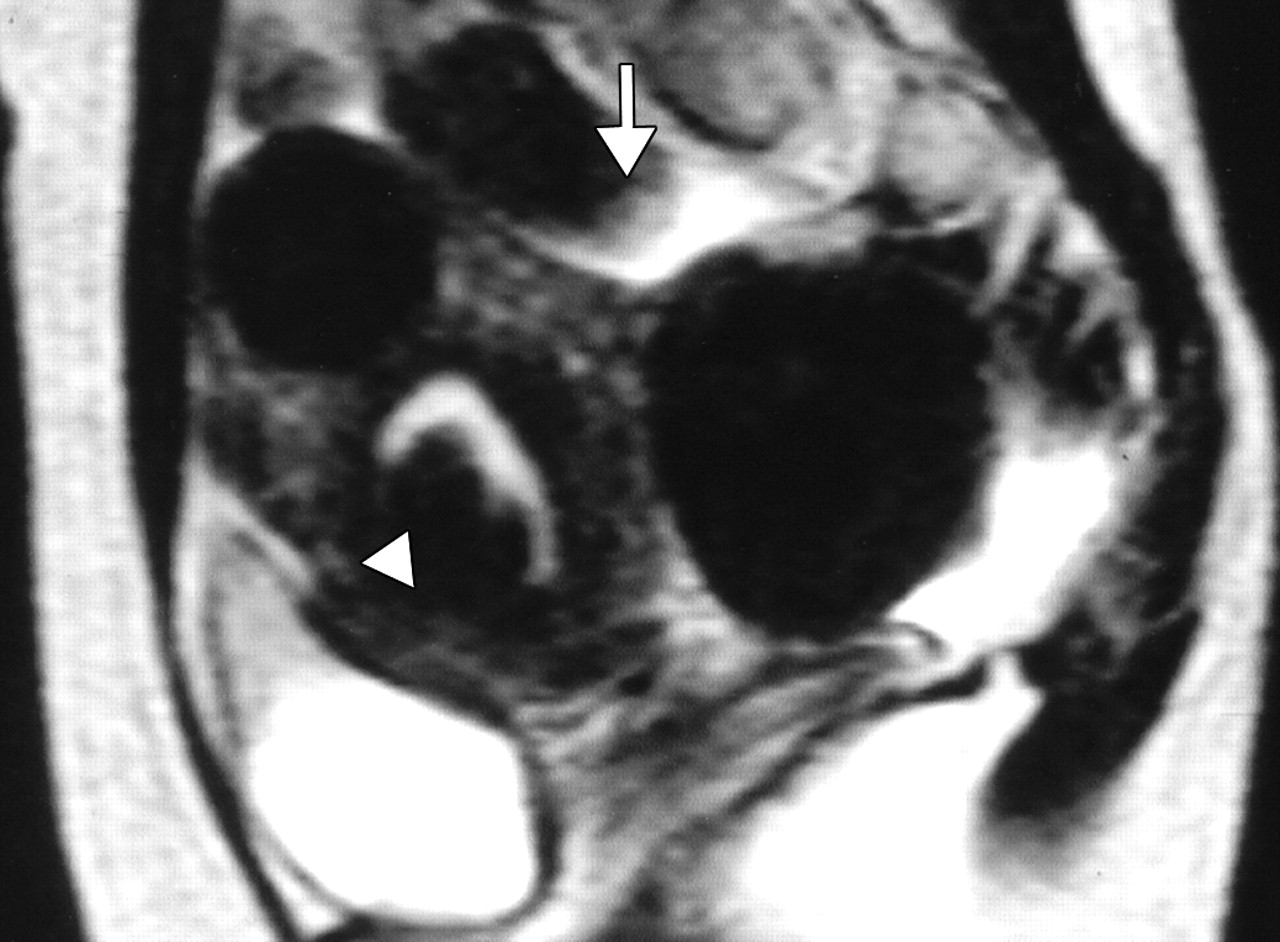
Uterine fibroids are benign tumors that develop in the uterus. While common among all women, fibroids disproportionately affect women of color. Fibroids are the leading cause of hysterectomy, with the average age of women undergoing this major surgery being just 39 years old (Fig. 1).
Fig. 1—44-year- old woman with menorrhagia and bulk-related symptoms caused by multiple uterine fibroids. T2-weighted MR image obtained before embolization reveals submucosal fibroid (arrowhead) and pedunculated subserosal fibroid 6 cm in maximal diameter. Diameter of stalk (arrow) is 2 cm.
Why Patients Should Consider Uterine Fibroid Embolization
UFE offers numerous benefits compared to hysterectomy or other surgical options:
Minimally Invasive
Performed by an interventional radiologist, UFE involves no surgical incisions
Outpatient Procedure
Patients typically go home the same day
Shorter Recovery Time
Recovery from UFE takes only 5–7 days compared to the 6–8 weeks often required after a hysterectomy
Uterus Preservation
Unlike a hysterectomy, UFE allows women to keep their uterus, maintaining their fertility and hormonal balance
Safe and Effective
UFE has a success rate of 90%, providing relief from fibroid symptoms like heavy menstrual bleeding, pelvic pain, and increased urinary frequency (Fig. 2)
Fig. 2—44-year- old woman with menorrhagia and bulk-related symptoms caused by multiple uterine fibroids. Contrast-enhanced T1-weighted MR image obtained 1 year after embolization reveals pedunculated subserosal fibroid, now 4.5 cm in maximal diameter, is not enhancing. Diameter of stalk (arrow) is now 1.1 cm. Rate of volume reduction in pedunculated subserosal fibroid is 61%. Menorrhagia and bulk-related symptoms markedly improved.
Why Keeping Your Patient’s Uterus Matters
Even for women not planning to have children, the uterus plays a vital role in overall health. Removing the uterus through hysterectomy can lead to serious complications, such as:
Psychological distress (often compared to the emotional impact of castration in men)
Sexual dysfunction, including reduced libido and loss of orgasm
Urinary incontinence
Significant bone loss
Increased risks of high blood pressure, heart attack, and stroke
Nearly all patients who qualify for surgery are also candidates for UFE, and UFE is covered by all major insurance providers, including Medicare and Medicaid.
Artificial intelligence (AI) now impacts radiologists at all stages of training and in all practice settings. Every day, radiologists hear of new opportunities and new challenges that AI will bring to their work and lives. Most practicing radiologists, and many radiologists in training, have not received the education necessary to navigate this new world, discern truth from hype, and recognize the dangers and responsibilities facing them as they integrate these systems into hospitals and clinics.
In order to safely, responsibly, and successfully develop, implement, and use AI systems to improve patient care and our work lives, radiologists must learn the basics in key areas. On Sunday, April 27 during the 2025 ARRS Annual Meeting at Marriott Marquis San Diego Marina, “Critical Education for Safe, Ethical, and Successful AI in Radiology” will provide expert guidance in:
Reliable AI: From Research to Production;
Practical AI: Implementation, Workflow and Monitoring;
Successful AI: Product Development, Validation, and Regulation;
Ethical AI: Bias, Diversity, Accessibility, and Privacy.
Most practicing radiologists have not received basic, trustworthy education that will allow them to understand, assess, implement, and successfully utilize AI products in their practices. Training programs now offer basic education about AI, but this often lacks teaching from those with broad experience and the ability to provide a comprehensive overview, including research, ethics, clinical implementation, and the business and economics of AI. Radiologists in practice and in training must be prepared to evaluate products, understand the important role of standards for AI integration into workflow, and be aware of pitfalls and dangers that could harm patients and the practice if not recognized. Led by course director Wende Gibbs, MD, attendees of “Critical Education for Safe, Ethical, and Successful AI in Radiology” will benefit from the unique group of speakers who are trailblazers in the areas of AI research, education, and business, and current and future leaders who are breaking down silos and facilitating multidisciplinary, multispecialty cooperation in the creation of safe, successful, and ethical AI for all.
Later in the afternoon on Sunday, April 27 in San Diego, CA, “Clinical Implementation of AI” will provide a timely review of best practices for selecting and a primer for deploying AI products to maximize return on investment. Course director Manisha Bahl, MD, has assembled four leading researchers in AI who also practice in different subspecialties. Their goal? Enhancing the overall value of any AI system by streamlining clinical workflows, while instilling effective methodology for monitoring said system’s practical impacts. Combining expert-led lectures with an interactive Q&A session, this ARRS Annual Meeting Sunday Session is open to all registrants.
Stacy J. Kim, MD Mallinckrodt Institute of Radiology Washington University in St. Louis
The first human lung transplant was performed in 1963. Since then, the number of lung transplant cases in the United States has steadily increased due to continued advancements in surgical technique and immunosuppressive medication. There were over 3000 lung transplants performed in the United States in 2023, and the number of lung transplants is likely to continue to increase [1]. The patients who undergo lung transplant are those with end-stage lung disease, which can result from a variety of pathologies including emphysema, fibrosing interstitial lung disease, cystic fibrosis, and pulmonary arterial hypertension. Postoperatively, these lung transplant recipients are vulnerable to complications for the remainder of their lives. The complications can be categorized by time course; that is, the time period after transplant during which the complications occur or most often occur.
The postoperative time periods can be organized as follows: immediate, within 24 hours of transplant; early, from 24 hours to 1 week after transplant; intermediate, from 1 week to 3 months after transplant; and late, more than 3 months after transplant [2]. Some complications can occur during more than one time period or span multiple time periods. This chapter will discuss the complications that occur or most often occur during the 1st month or so after lung transplant, which includes immediate, early, and some of the intermediate complications. Late complications of lung transplant will be discussed during the 2025 ARRS Annual Meeting Categorical Course, “Comprehensive Insights Into Transplant Imaging,” in San Diego, CA, and online April 27-May 1.
Imaging Techniques
Chest radiography is the most commonly used imaging study in the immediate and early postoperative setting. Chest radiographs are easy to acquire at the bedside and are useful in evaluating the positions of tubes and lines, which are ubiquitous immediately after transplant, such as endotracheal tubes, central venous catheters, and chest tubes. The lung parenchyma and the pleura can also be evaluated with chest radiographs for complications such as pneumonia and pleural effusion. Given the lower radiation dose of chest radiography when compared with CT, chest radiographs are useful for serial imaging; that is, image acquisition over multiple days to assess for change over time.
CT of the chest is performed if a more detailed assessment of the chest is required. Example scenarios in which a detailed assessment may be necessary include if there is concern for bronchopleural fistula in the setting of a persistent pneumothorax, if a pulmonary embolism (PE) is suspected due to new-onset tachycardia, and if a patient with decreasing hemoglobin values must be evaluated for hemorrhage. A noncontrast chest CT examination is sufficient for evaluation of the lung parenchyma, airways, and bones. A contrast-enhanced chest CT examination should be acquired (if the patient’s renal function permits and if the patient does not have a contrast media allergy) for evaluation of the vasculature and the pleura and assessment for active hemorrhage. The protocol or phase of contrast should be tailored to the diagnosis being evaluated; for example, a PE protocol should be used when evaluating for PE.
A noncontrast high-resolution chest CT examination is rarely necessary for the evaluation of early lung transplant complications. However, it is useful for the evaluation of late lung transplant complications as it can be used to detect air trapping and fibrosis (discussed in the next chapter). MRI, sonography, and nuclear medicine imaging are not typically used in the evaluation of early lung transplant complications.
Hyperacute and Acute Rejection
Hyperacute rejection occurs during the lung transplant surgery or within 24 hours of transplant when preformed recipient antibodies react to donor antigens in the allograft [3]. It is exceedingly rare because ABO blood group antigens and human leukocyte antigens are taken into account when lung donation is arranged, to ensure donor-recipient compatibility. Hyperacute rejection manifests as fulminant multiorgan system failure, and most patients with hyperacute rejection die within a few days to 2 weeks after lung transplant. The imaging findings of hyperacute rejection are nonspecific and resemble severe pulmonary edema, including consolidation, ground-glass opacities, and septal-line thickening. Acute rejection can occur anytime after lung transplant. It consists of two types, acute cellular rejection (ACR) and antibody-mediated rejection (AMR), which can coexist. ACR is the more common of the two types and occurs when recipient T lymphocytes attack donor antigens within the lung allograft. Approximately 35% of lung transplant recipients experience at least one episode of ACR during the 1st year after transplant [2]. During these episodes, patients may be asymptomatic or may present with nonspecific symptoms such as dyspnea and cough. The imaging findings of ACR are nonspecific and include consolidation, ground-glass opacities, and septal-line thickening; as with hyperacute rejection, ACR resembles pulmonary edema. Given its nonspecific clinical and imaging manifestations, ACR requires transbronchial biopsy and tissue analysis for diagnosis. Timely treatment, typically by increased immunosuppression with steroids, is important because ACR is the greatest risk factor for chronic lung allograft dysfunction [4]. Figure 1 shows a patient with biopsy-proven ACR.
Fig. 1—Patient with history of bilateral lung transplant who developed acute cellular rejection (ACR). Left: Chest CT at time of biopsy-proven ACR shows bronchial wall thickening and nodular ground-glass opacities in both lungs, as well as small pleural effusions. Right: Chest CT several months after treatment of ACR shows resolution of bronchial wall thickening, ground-glass opacities, and pleural effusions.
AMR, the less common of the two types of acute rejection, occurs when recipient B lymphocytes create donor-specific antibodies (DSA), donor-specific antigens and DSA form complexes, and the complexes trigger the immune system’s complement pathway. Like patients with ACR, patients with AMR can be asymptomatic; can have nonspecific symptoms such as dyspnea and cough; and can have normal chest imaging or nonspecific imaging findings resembling pulmonary edema such as consolidation, ground-glass opacities, and septal-line thickening. Transplant physicians diagnose patients with clinical versus subclinical AMR and definite versus probable versus possible AMR on the basis of the presence or absence of allograft dysfunction, histology results suggestive of AMR (such as neutrophil arteritis and capillaritis), immunostaining results (positive C4d staining of the capillary endothelium), and the presence or absence of DSA in peripheral blood [4]. Treatments include plasmapheresis and IV immunoglobulin to remove harmful antibodies and to suppress antibody production, respectively. Steroids are not typically used to treat AMR, unlike ACR. Figure 2 shows a patient with AMR.
Fig. 2—Patient with history of bilateral lung transplant who developed antibody-mediated rejection (AMR), which was diagnosed by transbronchial biopsy and donor-specific antibody blood testing. Chest CT at time of AMR diagnosis shows ground-glass opacities and reticulation in both lungs and small pleural effusions.
Primary Graft Dysfunction
Primary graft dysfunction (PGD) is a transient complication that occurs within 24–72 hours after lung transplant and tends to resolve by postoperative day 5–10. PGD is thought to be secondary to ischemic injury of the allograft before and during transplant and secondary to reperfusion injury after transplant. PGD occurs in approximately 10–30% of lung transplant recipients [5]. On imaging, it manifests as perihilar and lower lung–predominant airspace and interstitial opacities and is similar in appearance to pulmonary edema. Clinically, PGD is graded from 0 to 3 on the basis of the presence or absence of imaging abnormalities and the severity of hypoxemia [6]. In patients who have undergone a unilateral lung transplant, PGD and pulmonary edema can be differentiated by observing the distribution; PGD affects only the lung allograft, whereas pulmonary edema affects both the lung allograft and the native lung. Like acute rejection, PGD is considered a risk factor for chronic lung allograft dysfunction. It is treated with supportive care, such as mechanical ventilation and extracorporeal membrane oxygenation. Figure 3 shows a patient with PGD.
Fig. 3—Patient with right lung transplant who developed primary graft dysfunction (PGD). Left:Chest radiograph on postoperative day 0 shows clear right lung allograft and fibrosis of native left lung. Center: Chest radiograph on postoperative day 3 shows interval development of hazy airspace opacities throughout right lung allograft. Right:Chest radiograph on postoperative day 4 shows near resolution of right lung allograft airspace opacities, consistent with PGD.
Infection
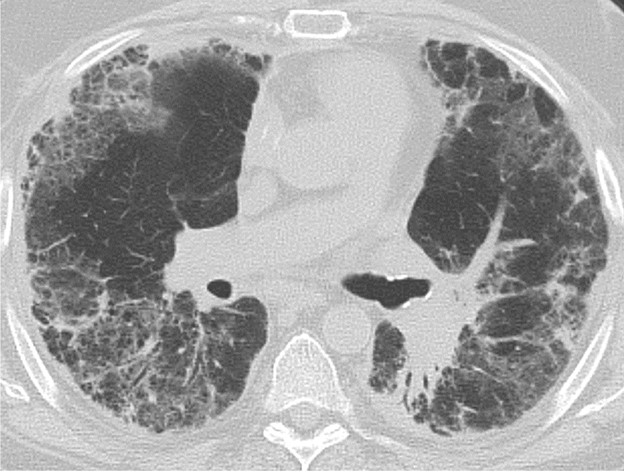
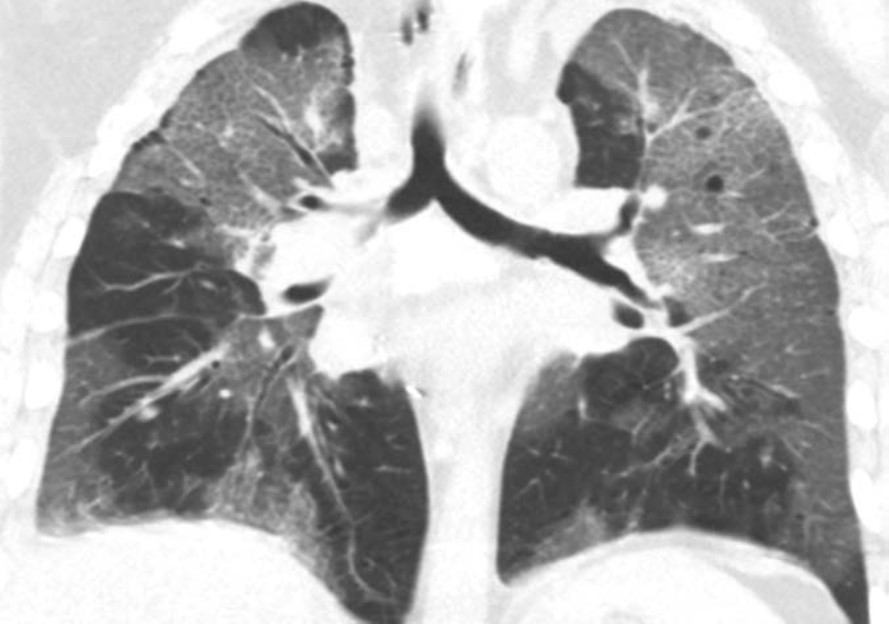
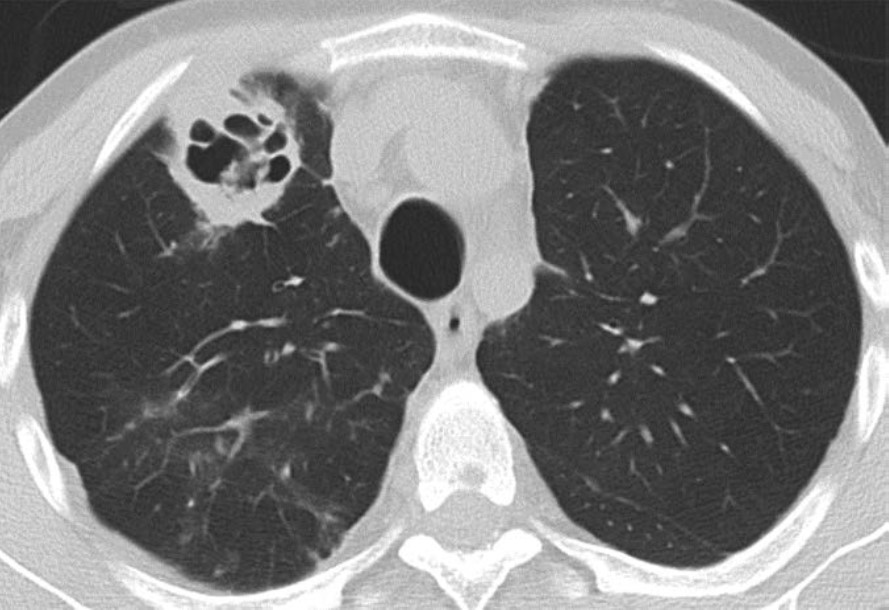
Infection of the lung parenchyma and airways is exceedingly common after lung transplant due to immunosuppression and decreased mucociliary clearance in the airways after transplant. Infection can occur anytime after transplant, including the early postoperative period. Patients are vulnerable to bacterial pneumonia as well as viral and fungal pneumonias not commonly encountered in immunocompetent patients. Common pathogens include Pseudomonas organisms, Staphylococcus aureus, cytomegalovirus, Epstein-Barr virus, herpes simplex virus, Aspergillus organisms, and Candida organisms [2]. The clinical and imaging manifestations of pneumonia in transplant recipients are similar to those of nontransplant patients. Lung transplant recipients who present with dyspnea, cough, or fever are evaluated for pneumonia. Imaging findings of pneumonia include consolidation, ground-glass opacities, septal-line thickening, and pulmonary nodules. Pulmonary nodules can be single or multiple; they may be solid or ground-glass in attenuation. Cavitary nodules and nodules with ground-glass halos can occur, especially in patients with fungal pneumonia. Imaging studies should be scrutinized for complications of infection such as pulmonary abscess and bronchopleural fistula. Patients may also have reactive pleural effusions or reactive mediastinal or hilar lymphadenopathy. Treatment is the same as in nontransplant patients and consists of antibiotics, antivirals, or antifungals depending on the causative pathogen. Figure 4 shows three different lung transplant recipients with pneumonia.
Fig. 4—Three different patients with history of bilateral lung transplant who presented with pneumonia. Left:Chest CT image shows consolidation and numerous small nodules in lungs due to bacterial pneumonia, in addition to left lower lobe cavitation and left empyema with gas in pleural space. Center: Chest CT image shows ground-glass opacities and septal-line thickening throughout both lungs caused by viral pneumonia (SARS-CoV-2). Right:Chest CT image shows cavitary lesion and multiple small nodules in right lung in patient with fungal (Aspergillus) pneumonia.
Pleural Complications
Simple pleural effusions and small pneumothoraces are frequently encountered in the immediate and early posttransplant setting and typically resolve within a few days to 1 week or so after lung transplant. Pleural fluid collections and pneumothoraces that are large, increasing in volume over time, or persist over 1 week may indicate a potentially serious complication such as hemothorax, empyema, bronchial anastomotic dehiscence, or bronchopleural fistula.
Hemothorax, the presence of blood products in the pleural space, should be suspected if there is rapid increase in the volume of pleural fluid over serial imaging or if pleural fluid is hyperattenuating relative to simple fluid on CT. Hemothorax can be heterogeneous in attenuation on CT due to mixing or layering of new blood products with old blood products; a fluid-fluid level may be present. Figure 5 (left) shows a patient with hemothorax.
Fig. 5—Two different patients with history of bilateral lung transplant who presented with hemothorax and empyema. Left: Chest CT image shows large heterogeneous-attenuation collection throughout right pleural space, consistent with hemothorax. Right: Chest CT image shows small- to moderate-volume collection in left pleural space with associated visceral and parietal pleural thickening and enhancement extending into prior left chest tube track, consistent with empyema. Patient also has small right pleural effusion with mild pleural thickening.
Empyema, the presence of infected material (i.e., pus) in the pleural space, should be suspected if there is persistence of pleural fluid over serial imaging for more than 1 week or so after transplant and if visceral and parietal pleural thickening or loculated pleural fluid is present on chest CT. On contrast-enhanced CT of the chest, patients with empyema may have abnormal thickening and enhancement of the visceral pleura and parietal pleura with fluid between the two pleural layers, which is known as the split pleura sign. Figure 5 (right) shows a patient with empyema.
Pneumothorax, the presence of gas in the pleural space, may be indicative of a bronchial anastomotic dehiscence or a bronchopleural fistula if it persists more than 1 week after transplant or increases in volume over time. A tension pneumothorax with cardiomediastinal shift away from the affected hemithorax should be immediately communicated to the transplant medicine team, as an untreated tension pneumothorax can cause cardiovascular and respiratory collapse. Small pneumothoraces on immediate postoperative chest imaging that resolve over the next few days, at which point any chest tubes present would be removed, are considered to be expected postoperative findings.
Treatment of pleural collections typically involves drainage of the pleural space material via pleural catheters or thoracostomy tubes. Surgical intervention may be required if drainage via catheters and tubes is unsuccessful or if the pleural collections are caused by complications such as bronchial anastomotic dehiscence or a bronchopleural fistula.
Vascular Complications
PE can occur after lung transplant. Hemorrhage most commonly occurs during the immediate and early postoperative periods and can manifest as hemothorax, other forms of thoracic hemorrhage such as mediastinal hematoma and chest-wall hematoma, and nonthoracic hemorrhage such as retroperitoneal hematoma. Approximately 4.5% of lung transplant recipients experience posttransplant hemorrhage severe enough to require surgical intervention [7]. The causes of hemorrhage include inadequate coagulation, vascular anastomotic dehiscence (which is rare but can be catastrophic when it occurs), and injury of other vessels. CT of the body part of concern (for example, CT of the chest if there is concern for mediastinal hemorrhage) should be performed, ideally with IV contrast material. If active hemorrhage is suspected, CT can be performed before and after the administration of IV contrast material in the arterial and venous phases to detect contrast material extravasation.
PE also most commonly occurs during the immediate and early postoperative periods. Patients are typically bedbound for at least the first few days after lung transplant, and some patients require mechanical ventilation during that time. Some patients may have been bedbound and/or may have been receiving mechanical ventilation while awaiting the transplant surgery. Immobility increases these patients’ risk for developing deep venous thrombosis (DVT) and subsequently developing PE. It is important to understand that lung transplant recipients are at increased risk of pulmonary infarction secondary to PE because the bronchial circulation is not reestablished during the transplant, and until collateral vessels form in a few weeks, these patients are relying on blood supply from the pulmonary circulation. If PE is suspected, CT of the chest with IV contrast material should be performed per the PE protocol.
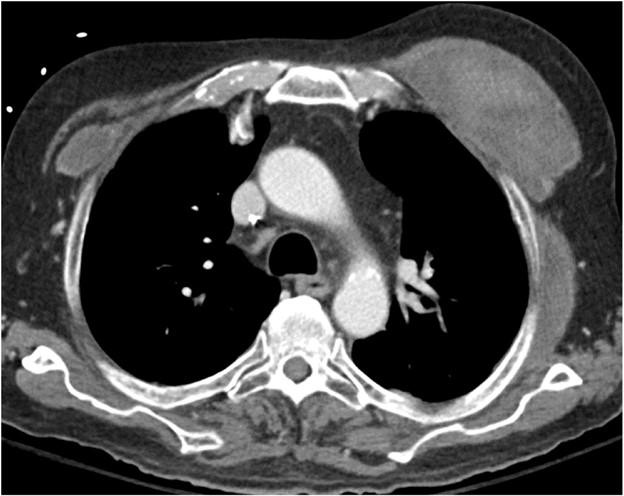
The imaging findings of hemorrhage and PE are the same in lung transplant recipients as in nontransplant patients. Hemorrhage manifests as hyperattenuating fluid (higher attenuation than that of simple fluid) or a hyperattenuating mass (if it is a hematoma) that often has a heterogeneous appearance. PE manifests as hypoattenuating and well-defined filling defects in the contrast material–opacified pulmonary artery branches. These filling defects can be occlusive or nonocclusive; nonocclusive acute PE is centrally located in the vessel lumen, rather than eccentric. Patients with coagulopathy and patients who are receiving anticoagulation therapy for DVT or PE may have both hemorrhage and PE on imaging. Figure 6 shows a patient with bilateral chest-wall hematomas.
Fig. 6—Patient with history of bilateral lung transplant who developed deep venous thrombosis in early postoperative setting was prescribed anticoagulation therapy and then spontaneously developed chest-wall hematomas, left greater than right. CT image shows heterogeneous-attenuation collections in right and left chest walls deep to pectoralis major muscles, which represent hematomas.
Pulmonary vein thrombosis and pulmonary venous anastomotic stenosis occur during the immediate and early postoperative periods, usually within 48 hours of lung transplant [8]. In pulmonary vein thrombosis, CT of the chest with IV contrast material shows a filling defect within a pulmonary vein, which may or may not be accompanied by consolidation, ground-glass opacities, and septal-line thickening in the lung parenchyma drained by the thrombosed pulmonary vein; the airspace opacities and septal-line thickening represent edema and hemorrhage due to venous ischemia and infarction. Endovascular intervention can be attempted, but cases of severe pulmonary vein thrombosis require surgery. Figure 7 (left) shows a patient with pulmonary vein thrombosis.
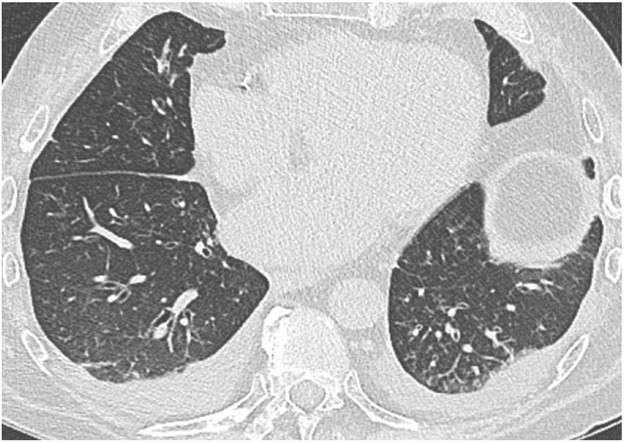
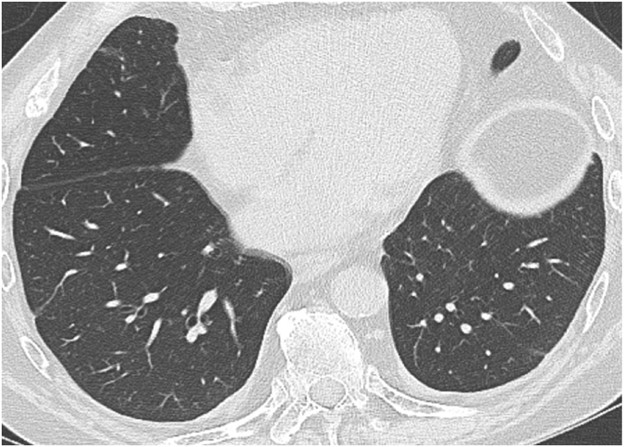
Fig. 7—Patient with history of bilateral lung transplant who presented with thrombosis of left inferior pulmonary vein. Left: Chest CT image acquired day after lung transplant shows occlusion of left inferior pulmonary vein (arrow). Right: Chest CT image shows consolidation and ground-glass opacities in left lower lobe indicative of edema and hemorrhage due to venous ischemia.
The pulmonary venous anastomosis is created adjacent to the left atrium. Stenosis of the pulmonary venous anastomosis is rare compared with stenosis of the pulmonary arterial anastomosis. On imaging, stenosis manifests as a focal narrowing of the pulmonary vein anastomosis that may or may not be accompanied by findings of venous ischemia and infarction in the lung parenchyma drained by the affected pulmonary vein, such as consolidation, ground-glass opacities, and septal-line thickening. As with pulmonary vein thrombosis, treatment options include endovascular intervention and, in severe cases, surgical repair. Figure 7 (right) shows a patient with pulmonary venous anastomotic stenosis.
Mechanical Complications
Mechanical complications include pulmonary torsion and lung herniation. Pulmonary torsion is a very rare complication of lung transplant and occurs during the immediate and early postoperative periods. A risk factor for lung torsion is when the donor lung is small relative to the recipient thoracic cavity, which means that the allograft is more mobile and likely to twist around its vascular pedicle after the transplant [9]. Careful size matching between the donor lung and the recipient chest cavity before the transplant surgery has greatly reduced the risk of lung torsion; however, given the potentially catastrophic consequences of torsion and the need for emergent surgical intervention, it remains an important diagnosis to be aware of. As previously stated, lung transplant recipients are particularly vulnerable to allograft ischemia and infarction because the bronchial circulation is not reestablished during transplant and the lung allograft must rely on pulmonary circulation until collaterals can form. Vascular compromise of the allograft due to torsion can result in severe allograft damage, allograft failure, or even death.
Imaging findings of pulmonary torsion can involve a lobe (in lobar torsion) or the entire lung (if the entire lung has twisted around its vascular pedicle). Pulmonary torsion can manifest as volume loss or collapse of the affected lobe or lung; it can also manifest as rapid expansion or opacification of the affected lobe or lung. Because of the twisting that occurs in torsion, patients with torsion have abnormal orientations and positions of anatomic structures such as lobes, hila, fissures, vessels, and airways. There may be abrupt cutoff of vessels and bronchi at the site of twisting. If pulmonary torsion is confirmed or suspected, the transplant physicians should be notified immediately to salvage as much of the allograft as possible. Pulmonary torsion requires emergent surgery to prevent allograft infarction and patient death.
Lung herniation can occur anytime after lung transplant. A major risk factor for lung herniation is increased intrathoracic pressure, as can be seen in patients with persistent cough due to pneumonia or aspiration after transplant. On imaging, herniated lung has an abnormal contour with a portion of lung bulging into the chest wall; this can occur at surgical sites (such as thoracotomy incisions) or at intercostal spaces. Mild herniation involving a small portion of the lung allograft with normal-appearing parenchyma is not worrisome. However, herniation involving a large portion of the allograft or deep herniation into the chest wall places the patient at risk for atelectasis, ischemia, infarction, and gangrene of the herniated lung, all of which can manifest as opacities within the herniated portion of lung. Surgical repair of the chest wall may be necessary in cases of pulmonary infarction or gangrene. Figure 8 shows a patient with lung herniation.
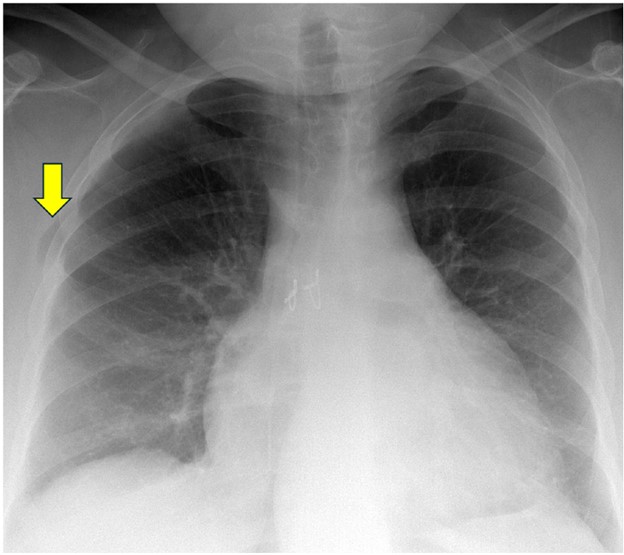
Fig. 8—Patient with history of bilateral lung transplant who presented with lung herniation. Frontal chest radiograph shows mild herniation of small portion of right upper lung into chest wall at thoracotomy incision site (arrow).
Conclusion
Lung transplant is increasingly becoming a cure for many patients with end-stage lung disease. In addition to academic chest radiologists, private practice radiologists and general radiologists are likely to encounter lung transplant recipients at some point in their careers. It is therefore essential for all radiologists to have a basic understanding of lung transplant complications—both common complications such as pneumonia and rare but life-threatening complications such as torsion. Although great progress has been made since the 1960s, the mean life expectancy of lung transplant recipients lags behind that of other organ recipients at only 6–7 years after transplant [10]. Early complications account for much of the morbidity and mortality in lung transplant recipients. These complications must be accurately detected and described when interpreting imaging studies, and they should be taken into account when protocoling imaging studies for lung transplant recipients. By doing so, radiologists can contribute to the postoperative care of lung transplant patients and can help optimize the quality and the duration of their posttransplant lives.
ERRATA:The winter issue featured this article with production errors, including inadvertent unauthorized changes to the title, introduction, and figures 3 and 4. We regret these errors and have republished the complete, corrected article for clarity.
References
Organ Procurement and Transplantation Network, U.S. Department of Health & Human Services. National Data: Transplants in the U.S. by Region. optn.transplant.hrsa.gov/data/view-data-reports/national-data. Published 2024. Accessed August 25, 2024
Kim SJ, Azour L, Hutchinson BD, et al. Imaging course of lung transplantation: from patient selection to postoperative complications. Radiographics 2021;41:1043-63
Masson E, Stern M, Chabod J, et al. Hyperacute rejection after lung transplantation caused by undetected low-titer anti-HLA antibodies. J Heart Lung Transplant 2007;26:642-45
Shah RJ, Diamond JM. Primary graft dysfunction (PGD) following lung transplantation. Semin Respir Crit Care Med2018;39:148-54
Snell GI, Yusen RD, Weill D, et al. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction, part I: definition and grading – a 2016 consensus group statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant 2017;36:1097-1103
Adelmann D, Koch S, Menger J, et al. Risk factors for early bleeding complications after lung transplantation – a retrospective cohort study. Transpl Int 2019;32:1313-21
Kim SJ, Short RG, Beal MA, et al. Imaging of lung transplantation. Clin Chest Med 2024;45:445-460
Amadi CC, Galizia MS, Mortani Barbosa EJ Jr. Imaging evaluation of lung transplantation patients: a time and etiology-based approach to high-resolution computed tomography interpretation. J Thorac Imaging 2019;34:299-312
Verleden GM, Glanville AR, Lease ED, et al. Chronic lung allograft dysfunction: definition, diagnostic criteria, and approaches to treatment – a consensus report from the pulmonary council of the ISHLT. J Heart Lung Transplant 2019;38:493-503
Going into 2025—the 125th anniversary of the American Roentgen Ray Society (ARRS)—I will be using my remaining InPractice columns as your president to provide more context regarding working happier as a radiologist. Centered in worker voice and equity, the happy radiologist is connected most to a safe and secure community—where everything from mentorship to scheduling works together to help foster a true sense of belonging. Opportunities for learning and accomplishment afford radiologists a dignity and meaning beyond our workstations, too.But let us start in 2022. I think we can all remember then. In the wake of the COVID pandemic, the United States Surgeon General, Dr. Vivek Murthy, released an updated framework for mental health and wellbeing in the workplace, outlining the foundational roles that workplaces must play in promoting health and wellbeing alike in our communities [1]. The U.S. Department of Health and Human Services was formally recognizing that our health care industries had to start focusing on working well. I want to share an accompanying figure from this federal framework with InPractice readers because it provides a great platform to think about ground-up, actionable initiatives that could work for our own specific radiological workplaces (Fig. 1).
Fig. 1—The five essentials for workplace mental health and wellbeing help organizations develop, institutionalize, and update policies, processes, and practices that best support the mental health and wellbeing of all workers.
Let’s turn our attention to the right side of this graphic: specifically, making connections and belonging to a community. The first step here is developing a culture. What does your chair or section chief value? What does your CEO treasure? We always talk about mission and vision, and answering these big questions are critically important to those conversations. Personally, I would like to know what my chair and my section value. And what are their goals for my own department? Additionally, what resources are our leaders able to provide to ground us in the institution’s values?
Lately, I’ve been looking at how the social supports of community are connected to a crucial distinction that the Surgeon General’s chart makes here. At the end of the workday, it’s not really a “balance” between that work and our lives at home. It is much more about work-life “harmony,” which Dr. Murthy’s office also notes is based in autonomy and flexibility.
When I was in training, we worked from seven to six o’clock, and then, we’d call from six o’clock to the next morning. Our schedule was rigid. It didn’t allow for a family, much less proper family time. During residency, I didn’t even go to the dentist; I simply didn’t have the time! And as a fellow, I remember tearing up when I got home from a RiteAid, of all places. I was crying because I’d never taken enough care of myself to go and buy products. I was just working so hard.
Given all the types of scheduling we have now, there are such wonderful opportunities with shift work. In January, our group moved to shift-type areas, where some people arrive at noon, some people come in at 4pm. This flexibility has provided a lot of satisfaction for our group, as directors have empowered us to choose the shifts that best fit our lives at that moment.
Moving clockwise, you’ll notice another essential element of working happier. Everyone reading this piece right now is a leader, or a valued member of a group with a leader at the helm. So, how do good leaders accommodate the group’s varied interests, while making individuals feel that they matter? In an academic setting, we can further foster flexibility with research and education, especially subspecialty experience. As you know, data have come out noting that if only 20% of your workday is spent doing something you like, you will be a much happier worker.
For me, my happiness at work is temporal bone. When I see a temporal bone case, I just start smiling because it brings me such great joy. Of course, our colleagues are happier when they’re reading cases that spark joy, so until next time, let’s really think about related worklist opportunities. I’ve seen some creative solutions in which worklists are done not by modality, but by image or imaging interests. Overall, reported happiness is much higher.
Athanasios Pavlou, MD University of Maryland School of Medicine R Adams Cowley Shock Trauma Center
Patient History
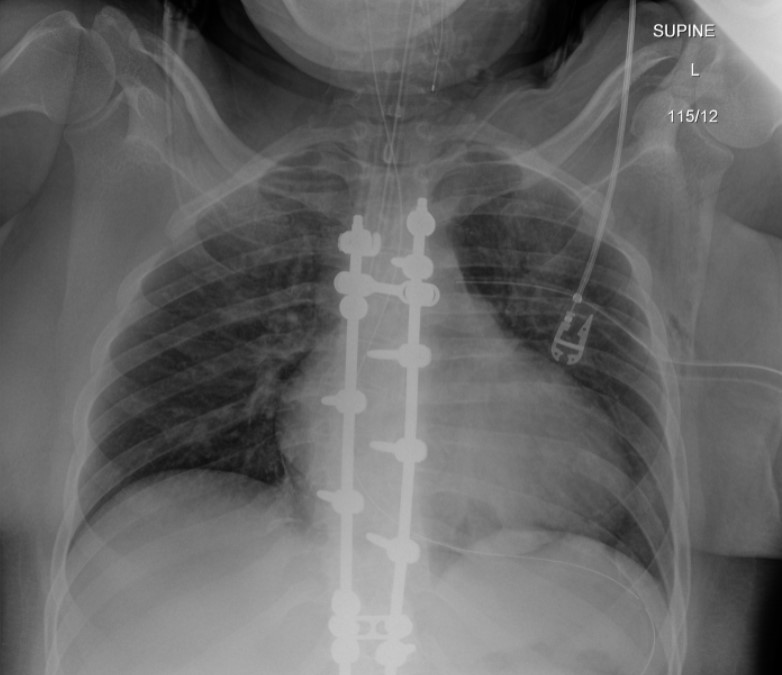
31-year-old female with no significant past medical history presented with multiple injuries after a motor vehicle accident. On arrival, the patient was conscious and moving her upper extremities but progressively developed lethargy.
Imaging Findings—Radiographs and CT Scan
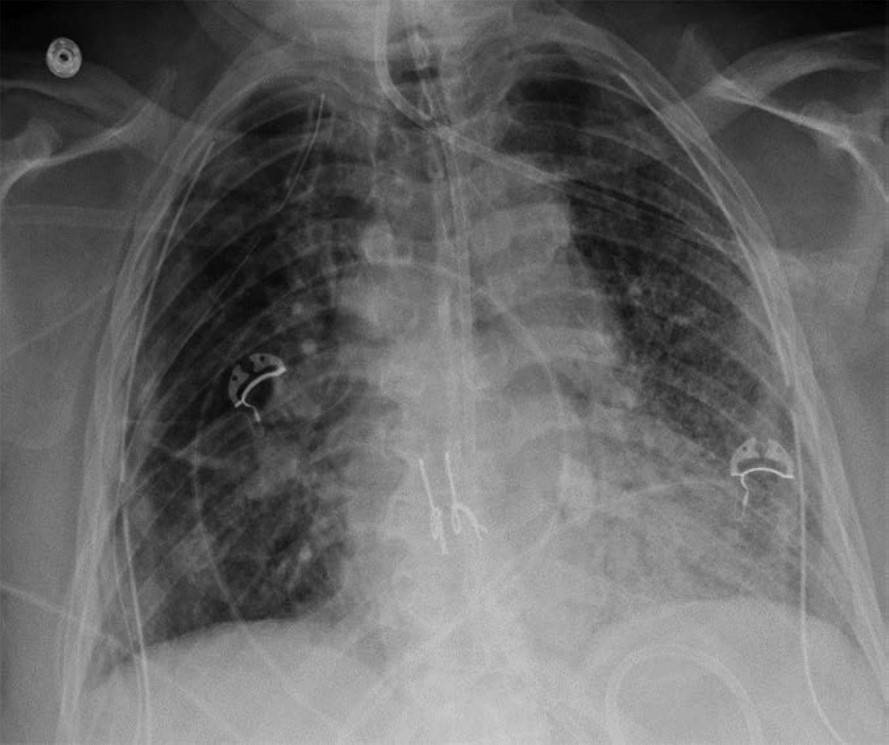
The initial chest radiograph (Figure 1) demonstrated a rounded retrocardiac partially lucent mass interpreted as a hiatal hernia.
Fig. 1—Initial radiograph showing retrocardiac partially lucent mass
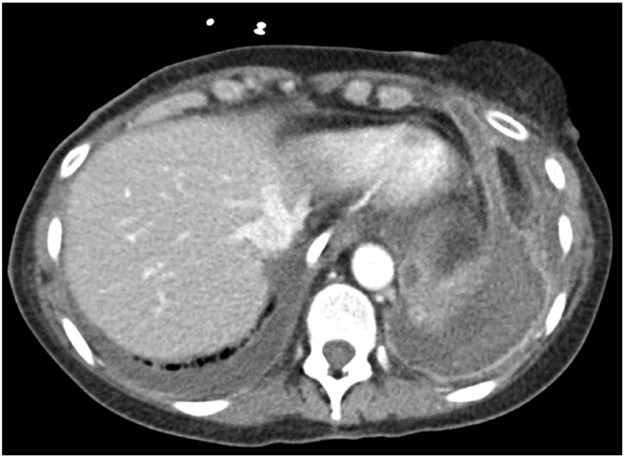
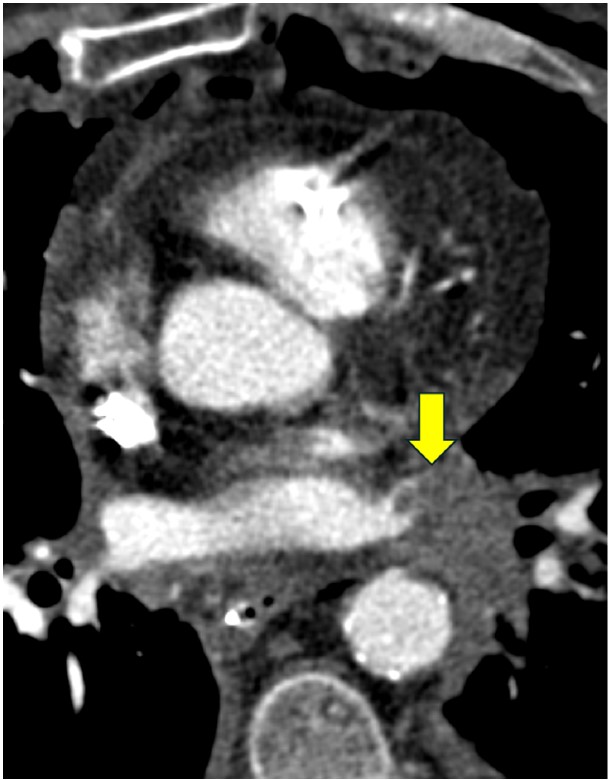
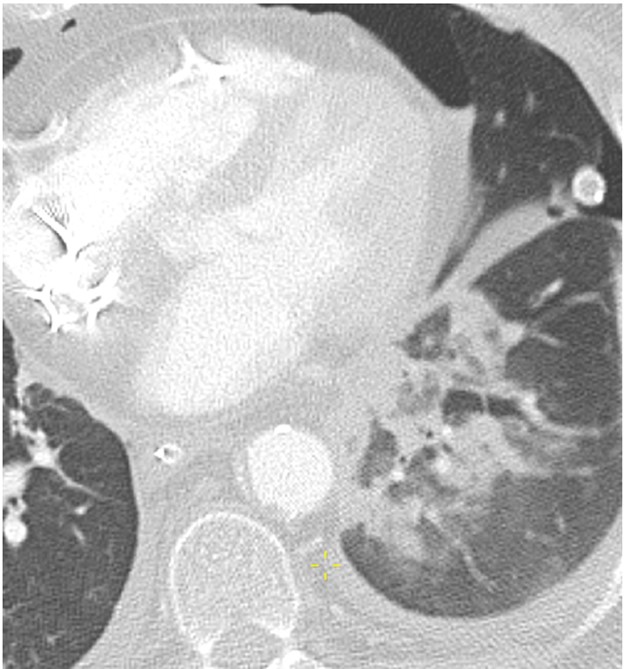
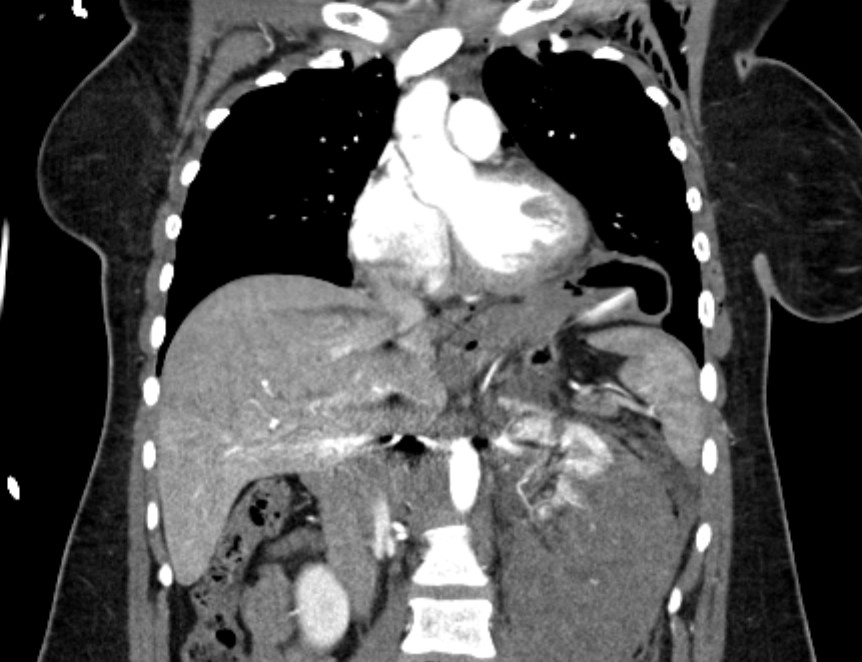
CT scan (Figure 2) revealed multiple clinically significant injuries, including a high-grade left renal injury. The stomach was elevated into the left hemithorax which was interpreted as the consequence of diaphragmatic eventration; medial diaphragm free edge was not appreciated.
Fig. 2—CT scan showing stomach herniating into left hemithorax
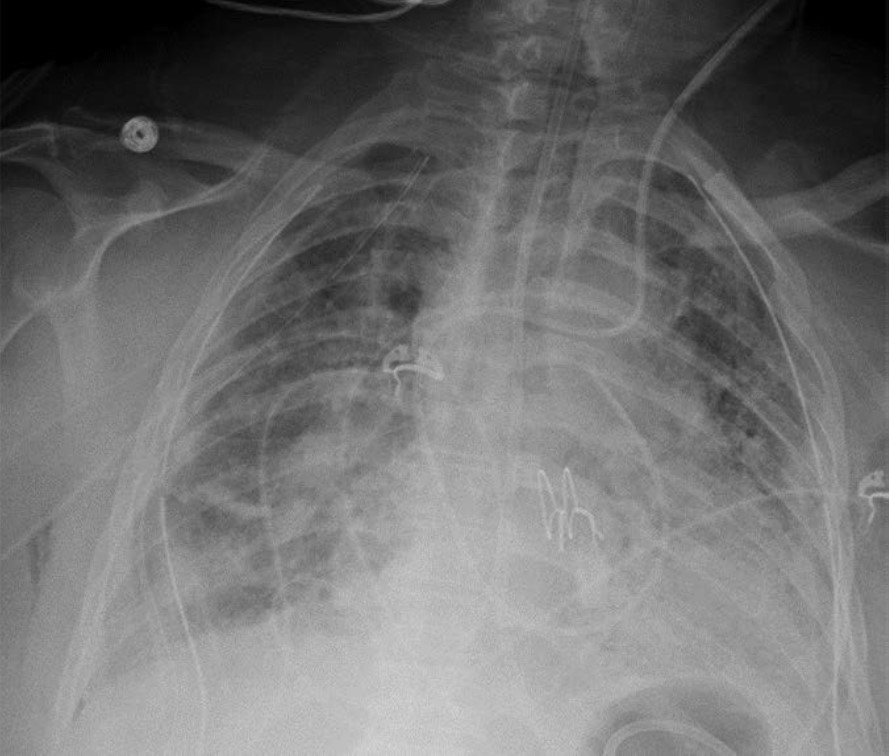
Postintubation radiograph (Figure 3) showed resolution of the retrocardiac mass with normal appearance of the diaphragm contour.
Fig. 3—Radiograph after intubation showing resolution of retrocardiac lucency
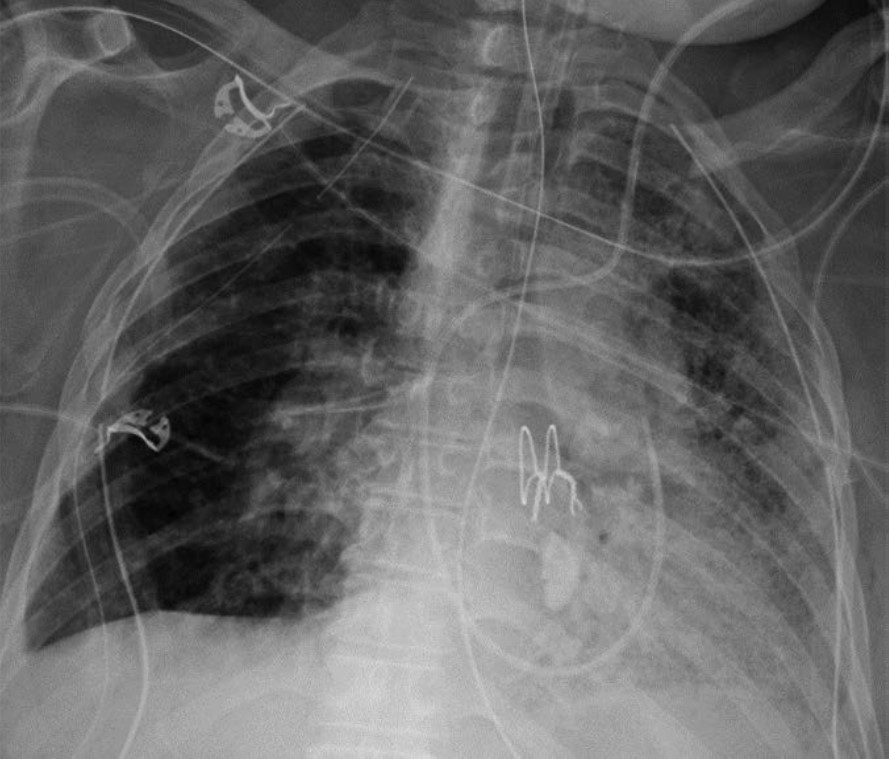
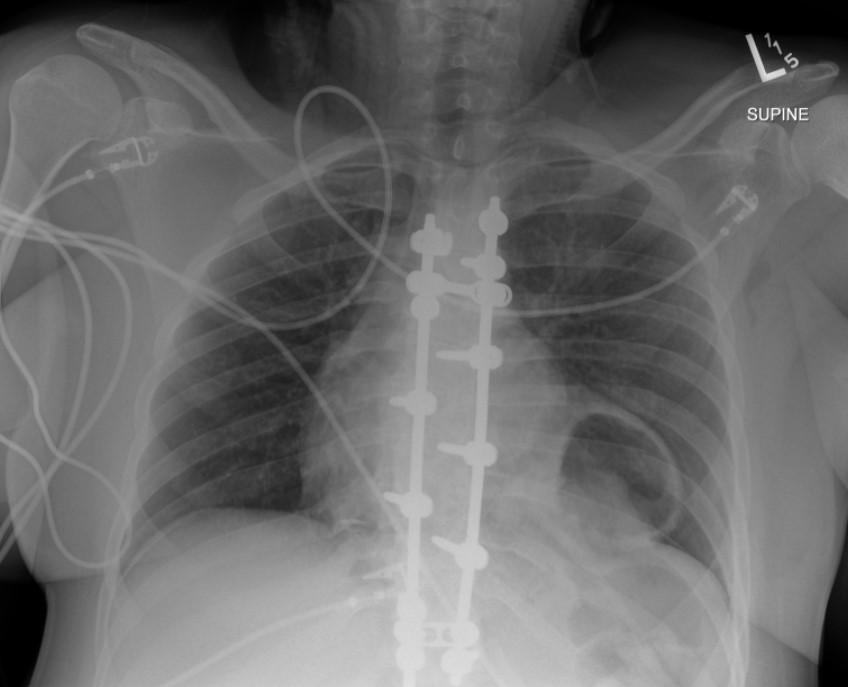
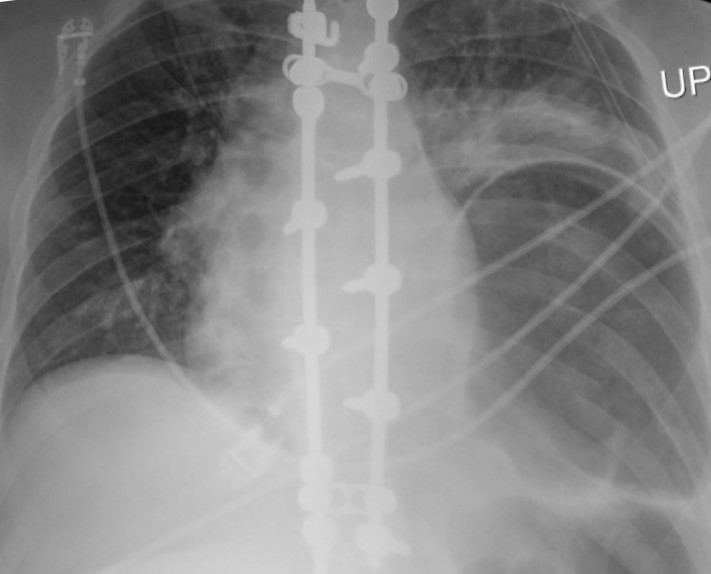
The patient subsequently underwent laparotomy for surgical repair of the renal injury. The follow-up radiograph (Figure 4) after extubation showed a recurrent lower left hemithorax partially lucent mass, increased in size compared to the initial radiograph.
Fig. 4— Radiograph postextubation showing recurrent large lower left hemithorax partially lucent mass
Which Is the Correct Diagnosis? Click on the arrows to reveal the correct answer.
Phrenic Nerve Injury
Incorrect. Please try again.
Congenital diaphragmatic hernia
Incorrect. Please try again.
Traumatic diaphragmatic injury
Correct! Read Further Discussion for more details.
Intraoperative diaphragmatic injury
Incorrect. Please try again.
Further Discussion
Traumatic diaphragmatic ruptures are infrequent with a reported incidence of 0.8-8% in patients who suffer blunt diaphragmatic trauma. They more commonly involve the posterolateral aspect of the left hemidiaphragm. Reported symptoms include chest or abdominal pain, dyspnea, cough, and even a presentation of hemodynamic instability.
The main radiographic finding suggesting diaphragmatic injury is the elevation of the “diaphragmatic contour” either with or without visualization of a herniating hollow viscus. This may be difficult to differentiate from preexisting hiatal hernia, basilar atelectasis, diaphragmatic eventration, congenital hernias, and phrenic nerve injury which may have a similar appearance. Furthermore, as with our case, positive pressure ventilation may lead to delayed diagnosis due to temporary reduction of the intraabdominal contents. The reported rate of missed diaphragmatic injury on chest radiographs is variable and ranges from 12 to 66%. CT has higher sensitivity and specificity for the diagnosis of diaphragmatic injuries. CT findings include visualization of the discontinuity of the diaphragm (73% sensitivity, 90% specificity), intrathoracic herniation of viscera (55% sensitivity,100% specificity), the collar sign (63% sensitivity, 100% specificity), which refers to a waist like constriction of the herniated viscera where it extends through the diaphragmatic defect, and the dependent viscera sign (90% sensitivity, 100% specificity) which describes the positioning of the abdominal viscera directly anterior to the posterior ribs due to loss of the diaphragmatic structural support.
Management of blunt diaphragmatic injury is surgical repair. Laparotomy or thoracotomy with direct suturing or surgical mesh is the mainstay of treatment.
The prognosis is favorable if diagnosed early and repaired. Missed injuries can lead to delayed herniation of abdominal viscera with resulting morbidity and mortality due to the risk of strangulation.
Points InPractice
Radiographic diagnosis of blunt left diaphragmatic injury may be suggested by elevation of the “diaphragmatic contour,” which can be misinterpreted as the result of other abnormalities.
Positive pressure ventilation can reduce the herniated viscera into the abdominal cavity and conceal the radiographic findings of a diaphragmatic injury.
In the setting of acute trauma, CT finding of intrathoracic herniation of abdominal contents has very high specificity for diaphragmatic injury and should be managed as such until proven otherwise.
References
Hammer MM, Raptis DA, Mellnick VM, et al. Traumatic injuries of the diaphragm: overview of imaging findings and diagnosis. Abdom Radiol 2017; 42:1020–1027
Iochum S, Ludig T, Walter F, et al. Imaging of diaphragmatic injury: a diagnostic challenge? RadioGraphics 2002; 22:S103–S116
Sliker CW. Imaging of diaphragm injuries. Radiol Clin N America 2006; 44:199–211
Zarour AM, El-Menyar A, Al-Thani H, et al. Presentations and outcomes in patients with traumatic diaphragmatic injury: a 15-year experience. Journ Trauma Acute Care Surg 2013; 74:1392–1398
McDonald AA, Robinson BRH, Alarcon L, et al. Evaluation and management of traumatic diaphragmatic injuries: a practice management guideline from the Eastern Association for the Surgery of Trauma. Journ Trauma Acute Care Surg 2018; 85:198–207
Min Lang, MD, MSc Department of Radiology, Massachusetts General Hospital Harvard Medical School
John Conklin, MD, MS Department of Radiology, Massachusetts General Hospital Harvard Medical School
Claire White-Dzuro, MD Vanderbilt School of Medicine
Neuroimaging plays a truly critical role in the initial evaluation of acute stroke. Although noncontrast head CT, followed by CT angiography (CTA), has historically been the standard imaging algorithm, it is well established in the literature and clinically that MRI is more sensitive for diagnosing acute ischemic stroke. Specific MRI sequences can provide vital information to help guide patient treatment decisions, especially for those with delayed presentation. For example, diffusion-weighted imaging (DWI) and fluid-attenuated inversion recovery (FLAIR) sequences often offer a better estimate for the onset of ischemia in patients with wake-up stroke.
As noted in our original AJR manuscript, “Triage of Patients With Acute Stroke for Endovascular Therapy: Point—Moving Toward MRI-Based Acute Stroke Triage With Ultrafast Protocols [1],” identification of DWI and FLAIR mismatch on MRI is suggestive of ischemic stroke with a duration of less than 4.5 hours, which is an important patient selection criterion for IV tissue-plasminogen activator (tPA). Additionally, MRI remains superior to CT perfusion imaging (CTP) for assessment of parenchymal integrity, tissue viability, and ischemic core—all of which can help determine thrombectomy and late-window thrombolysis candidacy.
Despite MRI’s superiority, CT remains the most commonly performed exam for code-stroke evaluation for two reasons. First, CT scanners continue to be much more accessible than MRI machines in emergency department (ED) and inpatient settings. Secondly, the imaging time for a head CT is on the order of seconds, whereas a brain MRI typically takes 10-15 minutes, depending upon which sequences are included in the protocol. The longer scan time for MRI results in the patient being more prone to motion, which could degrade the examination’s sensitivity.
Yes, we learned from the THRACE (Mechanical Thrombectomy After Intravenous Alteplase Versus Alteplase Alone After Stroke) Trial that there was a significant difference in acquisition time of a few minutes between patients who underwent CT versus MRI as their first imaging examination [2]. However, this slight delay in acquisition did not impact workflow or outcomes. And while CT remains the faster modality, when it is paired with additional imaging (e.g., CTA and CTP), overall imaging time ends up similar to MRI.
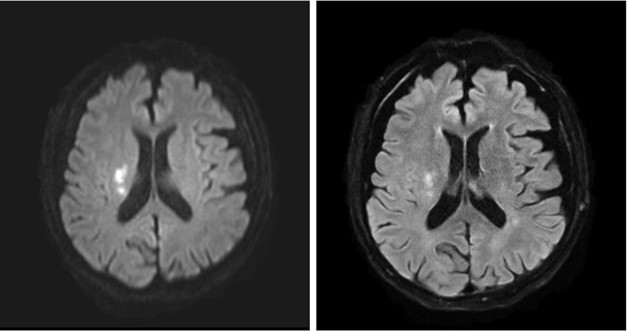
MRI’s intrinsic advantages over CT for evaluating acute infarction, as well as ongoing technological advances, have led to increases in MRI utilization within the ED: 38% from 1999 to 2008, though a more modest 18% from 2012 to 2019 [3-4]. (An increasing number of hospitals are moving toward 24/7 on-site MRI availability to obtain certification from The Joint Commission for Comprehensive Stroke Center, too.) In addition, newer ultrafast brain MRI protocols—comprised of T2/T2*-weighted, FLAIR, and DWI sequences—have been developed to further reduce acquisition times and increase the modality’s accessibility for acute stroke evaluation (Fig. 1).
Fig. 1—Images from axial ultrafast DWI sequence (left) of 21 seconds and axial ultrafast FLAIR sequence (right) of 51 seconds show clear diffusion restriction and T2-FLAIR hyperintensity, respectively, in right corona radiata, consistent with late-acute to early-subacute infarct.
The total acquisition time of the ultrafast brain MRI protocol is approximately 2-3 minutes. This ultrafast protocol uses the multi-shot echoplanar imaging (EPI) technique, a highly efficient interleaved EPI technique using multiple excitations, to decrease geometric distortion and increase SNR. Recent clinical validation of the ultrafast brain MRI protocol published in the American Journal of Neuroradiology showed similar sensitivity for detecting acute intracranial findings and acute ischemic infarct as compared to standard brain MRI protocol [5]. Motion artifacts were also significantly reduced on the ultrafast protocol images. Application of deep learning-assisted reconstruction techniques will only continue to improve image quality and SNR, increasing the confidence of radiologists’ interpretations.
CT will remain the first imaging modality for any unstable patient, as well as for patients where MRI is contraindicated or where a facility faces limited scanner availability. But look at all the benefits of choosing MRI over CT for initial acute infarct screening, including:
Differentiating stroke from mimickers
Migraine
Seizure
Demyelinating process
Infection
Neoplastic process
No radiation
Lower risk for hypersensitivity reaction to gadolinium-based contrast agents
To conclude, with newer MR acceleration techniques, ultrafast MRI-based acute stroke evaluation has been shown to be fast, safe, and accurate. Therefore, MRI should be considered a suitable initial triage imaging modality for the appropriate patient and facility.
References
Lang M, Conklin J. Triage of patients with acute stroke for endovascular therapy: point—moving toward MRI-based acute stroke triage with ultrafast protocols. AJR May 2024. doi: 10.2214/AJR.24.31303
Provost C, Soudant M, Legrand L, et al. Magnetic resonance imaging or computed tomography before treatment in acute ischemic stroke. Stroke 2019; 50:659-664
Burke JF, Kerber KA, Iwashyna TJ, Morgenstern LB. Wide variation and rising utilization of stroke magnetic resonance imaging: data from 11 states. Ann Neurol 2012; 71:179-85
Wang JJ, Pelzl CE, Boltyenkov A, et al. Updated trends, disparities, and clinical impact of neuroimaging utilization in ischemic stroke in the Medicare population: 2012 to 2019. J Am Coll Radiol 2022; 19:854-865
Lang M, Clifford B, Lo WC, et al. Clinical evaluation of a 2-minute ultrafast brain MR protocol for evaluation of acute pathology in the emergency and inpatient settings. Am J Neuroradiol Mar 2024. doi:10.3174/ajnr.A8143
Katerina Dodelzon, MD, FSBI Associate Professor of Clinical Radiology Associate Director Breast Imaging Fellowship Vice Chair of Clinical Operations Weill Cornell Medicine
Physician burnout was its own epidemic, with radiologists consistently ranking among the most burned-out medical specialties, well before the COVID pandemic. The acute and now chronic stressors of COVID further exacerbated radiologists’ wellness with 54% of radiologists reporting symptoms of burnout, according to a recent Medscape report [1]. In addition to radiologists’ wellness, burnout has significant adverse implications on patient care and outcomes [2].
In its most simplistic dissection, burnout is composed of three parts:
Depersonalization
Physical and emotional exhaustion
Low sense of personal accomplishment
As such, the very fundamental aspect of our job as physicians, that of connecting and communicating with patients, may play a central role in physician wellness. A direct association can be observed between physicians’ level of satisfaction with their job and their ability to build rapport and connect with patients [3]. Rapport and relationship building both decrease depersonalization and increase a sense of personal accomplishment. Although anxiety related to challenging physician interactions, which have been shown to last for days beyond the interaction, can lead to fatigue, if cumulative, these interactions may lead to exhaustion [4]. Furthermore, anxiety surrounding challenging patient interactions, like delivering bad news, is more likely to occur if one is faced with such interactions infrequently, and thus feel unprepared or unskilled to navigate them.
Demonstrating the critical impact of patient-physician communication interaction on physician mental health, a recent national study of breast radiologists’ wellness found that less time spent connecting with, educating, and consulting patients was statistically significantly associated with greater odds of reporting psychological distress and anxiety [5]. Interestingly, although increase in frequency of more negative and charged patient interactions were reported by some radiologists in the study, no association between negative interactions and mental health was found. Therefore, it appears that it’s the length of time allotted for physicians to build rapport and make meaningful connections with their patients to educate and inform, rather than the nature of the interactions themselves, which significantly affects radiologists’ wellness.
As institutions, practices, and individual physicians devise strategies for burnout mitigation, time and adequate focus should be allotted to patient-centered communication. Operational leadership should be intentional in incorporating sufficient time for radiologists to discuss results and consult with patients into the daily workflow, not limiting interactions in favor of increased volume. Communication skill training should be increasingly integrated into radiology training curricula. In addition, training and effective communication skill resources should be emphasized and made readily available for all faculty to equip radiologists with the confidence to approach a variety of challenging patient interactions, thus diminishing communication-related anxiety [6]. Radiologists, themselves, should emerge from behind the workstation, seeking out opportunities to consult and educate patients—as our very own wellbeing depends on it.
Panagioti M, Geraghty K, Johnson J, et al. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med 2018; 178:1317–1331
West CP, Dyrbye LN, Shanafelt TD. (Mayo Clinic, Rochester, MN; and Stanford University Medical Center, Stanford, CA, USA). Physician burnout: contributors, consequences and solutions (Review). J Intern Med 2018; 283:516–529
Ptacek J, Fries E, Eberhardt T, et al. Breaking bad news to patients: physicians’ perceptions of the process. Support Care Cancer 1999; 7:113–120
Dodelzon K, Grimm LJ, Plimpton SR, et al. Ongoing impact of COVID-19 on breast radiologists’ wellness. Journ Breast Imag 2023; 3:287–296
Dale West, CAE, has been named incoming Executive Director for the American Roentgen Ray Society (ARRS). West will serve as the administrative and strategic partner to the ARRS Executive Council, overseeing day-to-day operations of the Society, as well as the financial and business operations of the Society’s products and service offerings.
“Dale West has led health care associations to achieve operating excellence and strategic success,” said Angelisa M. Paladin, MD, 2024-2025 ARRS President.
“Dale is skilled in creating growth strategies, ensuring operational efficiencies, driving change, and effectively staffing teams with the talent and drive to achieve our Society’s mission and goals,” Dr. Paladin continued.
Dale West has a strong and established history of successfully developing vibrant association communities, working collaboratively with Boards of Directors, and guiding cross-functional teams to exceed the objectives of the associations he supports.
Currently, West serves as Vice President of the Health Care Clinical and Administrative Unit and Executive Director of the Commission on Accreditation of Athletic Training Education at Smithbucklin, the world’s largest association management company.
“I am truly honored to join the American Roentgen Ray Society as its new Executive Director,” Dale West said.
“ARRS has a rich legacy, and I am excited to work with our dedicated volunteers and staff to build on that success. We will strengthen our community and advance our mission and the field. I am excited about the opportunities ahead and look forward to what we will accomplish in the coming years.”
“Among a field of outstanding candidates, Dale rose to the top,” noted Erik K. Paulson, MD, chair of the search committee and past president of ARRS.
“We are delighted to move forward with him as our new Executive Director,” Dr. Paulson added.
Dale West officially assumes the position on January 2, 2025—following the retirement of longtime ARRS Executive Director, Susan B. Cappitelli, MBA, CAE. The American Roentgen Ray Society thanks Susan for her many years of exceptional service and contributions, always prioritizing member service and the advancement of the specialty.
The American Roentgen Ray Society (ARRS) is pleased to announce Erin Alaia of NYU Langone Health in New York City as the 2025 Melvin M. Figley Fellow in Radiology Journalism. ARRS also recognizes Domen Plut from Slovenia’s University Medical Centre Ljubljana as the 2025 Lee F. Rogers International Fellow in Radiology Journalism.
Supported by The Roentgen Fund® and named for two distinguished Editors Emeriti of ARRS’ own American Journal of Roentgenology (AJR), the Melvin Figley and Lee Rogers Fellowships offer practicing radiologists an unparalleled opportunity to learn the tenets of medical publishing via “the yellow journal”—the world’s longest continuously published radiology journal. Through hands-on experience with ARRS staff and AJR personnel—as well as personal apprenticeship with AJR’s 13th Editor of Chief, Andrew B. Rosenkrantz—Drs. Alaia and Plut will receive expert instruction in scientific writing and communication, manuscript preparation and editing, peer review processes, journalism ethics, and digital publication.
Additionally, Drs. Alaia and Plut will attend the 2025 ARRS Annual Meeting in San Diego, CA, where they will co-present the AJR Year in Review Sunday Session and participate in the Editor’s Forum.
Founded in 1907, AJR is one of the specialty’s leading peer-reviewed journals, publishing clinically oriented content across all imaging subspecialties and modalities relevant to radiologists’ daily practice. Publishing hundreds of articles annually in a diverse range of formats, including original research, reviews, clinical perspectives, editorials, and other short reports, AJR further engages its audience through a spectrum of social media and digital communication activities. In 2023, the journal garnered 32,133 citations and received an impact factor of 4.7, placing AJR at the 89.5th percentile in the radiology, nuclear medicine, and medical imaging category (as reported by Clarivate Analytics).
Since 1990, The Roentgen Fund has granted millions of dollars to hundreds of imaging professionals for both research pursuits and professional development. Today, through six vital scholarship and fellowship programs, the generosity of The Roentgen Fund’s donors is channeled to every corner of the globe—establishing dual foundations in innovation and leadership for a true diversity of radiology’s next generation.
Erin F. Alaia, MD, is an associate professor of radiology and orthopedic surgery at NYU Langone Health in New York, NY. Chair of ARRS’ Radiology Review Track Musculoskeletal Imaging Section, her research, clinical interests, and areas of expertise include sports imaging, postoperative sports imaging, and musculoskeletal infection. As the recipient of a 2022 Research Seed Grant from the Radiological Society of North America, Dr. Alaia focused on the utility and cost-effectiveness of MRI in older patients with hip and knee pain. Prior chair of the Society of Skeletal Radiology Research Committee, presently, she serves on the consulting editorial board of Skeletal Radiology, having received certificates of distinction for her contributions as a reviewer from 2021-2023. Guest editor for an upcoming issue of Seminars in Musculoskeletal Radiology focused on post-operative imaging, Dr. Alaia is also a member of the American College of Radiology’s Committee on Body Imaging, Musculoskeletal Section.
Domen Plut, MD, PhD, completed his medical studies and radiology residency at the University of Ljubljana’s Faculty of Medicine and University Medical Centre Ljubljana in Slovenia. In 2021, he received the European diploma in pediatric radiology, marking him among the first generation in this subspecialty on the continent. In 2022, Dr. Plut was appointed assistant editor at AJR. An assistant professor at the Medical Faculty of Ljubljana, chief of University Medical Centre Ljubljana’s pediatric radiology department, and recipient of the 2023 Lavrič “Best Teacher” Award, teaching is his passion. Dr. Plut is extensively involved in research, having published 45 articles in reputable journals—28 as first or lead author—and serving as a reviewer for many other publications. General Secretary of the Slovenian Association of Radiology and a member of both the European Society of Radiology and European Society of Paediatric Radiology (ESPR), he is a part of ESPR’s Musculoskeletal and Cardiothoracic Taskforce. Dr. Plut’s primary work and research interests include imaging of neonates and contrast-enhanced ultrasound, and he has presented his findings at numerous international radiology conferences, including several annual meetings of the ESPR and Radiological Society of North America.
ARRS Scholar Update: Steven Rothenberg
Steven Rothenberg, MD, is in the second year of his ARRS Scholarship program, investigating methods for mitigating the nocebo effect in diagnostic reporting of lumbar spine MRI. Currently, he is recruiting for his first prospective randomized controlled clinical trial: NCT06103474. Since receiving his ARRS Scholarship during the 2023 ARRS Annual Meeting in Honolulu, HI, Dr. Rothenberg has been awarded Most Prolific Inventor by the Herbert Institute for Innovation and Entrepreneurship and the Light Bulb Award from the University of Alabama at Birmingham’s radiology department. His submission of eight invention disclosures have led to three distinct patent applications and one notice of allowance (US20240257947A1) from the United States Patent and Trademark Office. Meanwhile, Dr. Rothenberg’s research findings have yielded five co-authored published articles, two related editorials, and two AJR Original Research manuscripts presently in press. As an ARRS Scholar, thus far, he has presented 19 scientific abstracts, earning a Certificate of Merit during the 2024 ARRS Annual Meeting in Boston, MA. Dr. Rothenberg continues to donate to The Roentgen Fund to give back in support of other early-stage faculty applying for future ARRS Scholarships.
Steven Rothenberg, MD, is in the second year of his ARRS Scholarship program, investigating methods for mitigating the nocebo effect in diagnostic reporting of lumbar spine MRI. Currently, he is recruiting for his first prospective randomized controlled clinical trial: NCT06103474. Since receiving his ARRS Scholarship during the 2023 ARRS Annual Meeting in Honolulu, HI, Dr. Rothenberg has been awarded Most Prolific Inventor by the Herbert Institute for Innovation and Entrepreneurship and the Light Bulb Award from the University of Alabama at Birmingham’s radiology department. His submission of eight invention disclosures have led to three distinct patent applications and one notice of allowance (US20240257947A1) from the United States Patent and Trademark Office. Meanwhile, Dr. Rothenberg’s research findings have yielded five co-authored published articles, two related editorials, and two AJR Original Research manuscripts presently in press. As an ARRS Scholar, thus far, he has presented 19 scientific abstracts, earning a Certificate of Merit during the 2024 ARRS Annual Meeting in Boston, MA. Dr. Rothenberg continues to donate to The Roentgen Fund to give back in support of other early-stage faculty applying for future ARRS Scholarships.
2023 ARRS Scholars Andrew Wentland, assistant professor at the University of Wisconsin School of Medicine & Public Health, and Steven Rothenberg, assistant professor at the University of Alabama at Birmingham