Updated October 25, 2021

Victoria Chernyak
Associate Professor of Radiology, Harvard Medical School
Beth Israel Deaconess Medical Center
@VChernyakMD
2021 ARRS Symposium Course Director
Abdominal MRI: Practical Applications and Advanced Imaging Techniques

Kathryn J. Fowler
Professor of Radiology, University of California San Diego
University of California San Diego Health
@chemshift1
2021 ARRS Symposium Course Director
Abdominal MRI: Practical Applications and Advanced Imaging Techniques
As MRI technology continues to improve, radiologists must maintain a mastery of complex sequences, evolving protocols, and advanced techniques. Likewise, disease-specific guidelines, protocols, and reporting continue to evolve. Radiologists in all practice types are often tasked with managing a busy practice at this intersection of advanced technology and state-of-the-art clinical care.
From September 9–10, the ARRS Virtual Symposium, Abdominal MRI: Practical Applications and Advanced Imaging Techniques, delivered trusted perspectives on the most pressing issues in body MRI—ranging from protocol and acquisition optimization, incorporation of advanced techniques in routine clinical practice, and interpretation/reporting for the most important trends in liver, prostate, emergency, and gynecological MR imaging. What follows is our primer for those unable to attend the live sessions.

Abdominal MRI: Practical Applications and Advanced Imaging Techniques
This Online Course covers strategies for protocol optimization, standardized interpretive schemas and assessment systems, as well as advanced topics in emergency settings and liver MRI.
Emergency MR Imaging
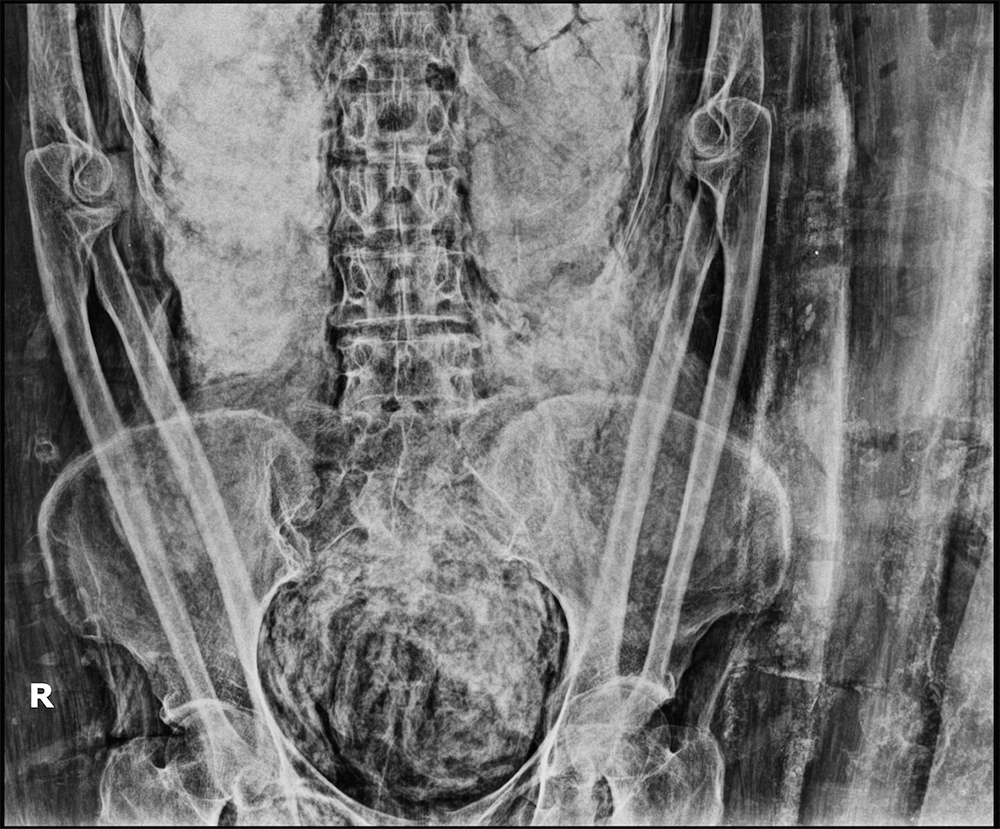
Although CT is the workhorse imaging modality in the emergency department (ED), there are many concerns related to ionizing radiation exposure in populations that are vulnerable due to young age, pregnancy, or exposure to repeated imaging examinations. In patients with nontraumatic acute abdominal symptoms, non-contrast MRI offers similar diagnostic performance to CT. For instance, in a prospectively enrolled cohort of 48 patients with head-to-head comparison of MRI to CT, there was no significant difference in performance for diagnosing acute appendicitis in young adults and adolescents (Fig. 1).
A key to harnessing the efficacy of MRI in the ED setting is through protocol optimization, focusing on efficiency and speed. Abbreviated protocols, comprising fewer and faster sequences, allow for improved adoption, decreased cost, and maintained sensitivity for answering directed clinical questions. For example, in the ED setting, compared to conventional MR cholangiopancreatography (MRCP) protocols, abbreviated MRCP provides significant time savings, while maintaining similar diagnostic accuracy for the detection of choledocholithiasis. ARRS Symposia course director Victoria Chernyak, ARRS Instructional Courses Committee chair Courtney Coursey Moreno, and Elena Korngold highlighted ED MR protocols and imaging findings for common genitourinary and gastrointestinal emergencies.
Advanced MR Techniques
Beyond the ED setting, advanced MR imaging techniques have opened the door for quantitative imaging, and multiparametric assessment has become standard practice for many disease processes. Sequences for assessment of liver steatosis, iron deposition, and fibrosis are now available on all major MR vendor platforms, allowing accurate diagnosis and monitoring of patients with chronic liver diseases. A working knowledge of how to extract and report the quantitative data derived from MRI proton density fat fraction, R2* maps, and elastography is required to build a state-of-the-art radiology liver practice. Diffusion weighted imaging (DWI) is no longer an ancillary or optional sequence but is required for accurate multiparametric assessment of prostate cancer. DWI can be used as a biomarker of tumor response; for instance, DWI adds value in assessing response to neoadjuvant therapy in patients with rectal cancer. While important and useful, DWI can be challenging to optimize and interpret in practice. 2002 ARRS Scholar Claude B. Sirlin imparted his applied wisdom regarding DWI acquisition optimization and interpretation, Mustafa Rifaat Bashir offered insights into some of the new sequences and future directions, and Antonio Carlos A. Westphalen emphasized the utility of DWI in the current prostate imaging reporting and data system (PI-RADS) v2.1.
Protocol Optimization
In practice, MRI provides both great potential and great challenges. Optimizing sequences across multiple scanners, technologists, and protocols can be laborious and frustrating for radiologists. Optimized MRI protocols achieve a delicate balance between acquisition times, image quality, and sequence comprehensiveness, and they are—to paraphrase Albert Einstein—made as simple as possible, but no simpler. Richard Kinh Gian Do, Steven S. Raman, Elizabeth A. Sadowski, and Korngold shared their expert insights into optimal protocols for hepatobiliary, prostate, female pelvis, and bowel imaging. Bashir presented real-world methods for recognizing and, most importantly, mitigating artifacts commonly encountered in abdominal MR imaging.
State-of-the-Art Reporting
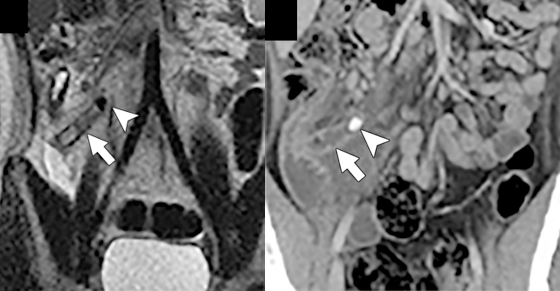
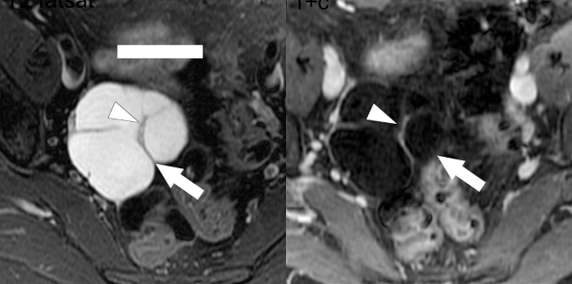
Optimizing images is just one hurdle for delivering the best imaging care to patients. Over the last decade, there has been a major movement toward standardized reporting for many disease processes in the abdomen and pelvis. Standardized reporting allows for more precise communication of results and improves compliance with diagnostic criteria. Notably, the liver imaging reporting and data system (LI-RADS), PI-RADS, ovarian reporting and data system (O-RADS), and updated Bosniak criteria are increasingly recognized as the standard of care for interpretation and reporting. ARRS Symposia course codirector Kathryn J. Fowler, Westphalen, Raman, and Sadowski provided an overview of these important systems, a framework for applying them, as well as insights into creating templates to improve reporting efficiency (Fig. 2).
Delivering state-of-the-art care with MRI requires comfort with the technical aspects of image acquisition, reporting standards and approaches to common disease processes, and advanced sequences as integrated into practice. Taught by world-renowned MR imaging experts, Abdominal MRI: Practical Applications and Advanced Imaging Techniques provided practicable tools to harness the power of these expanded procedures for improving patient care.