Medical errors are common and can affect overall patient care. Radiology is integral in many aspects of overall patient care, and radiologists play a critical role. As such, radiologists can affect patient morbidity and mortality as a consequence of diagnostic error. Radiologists must recognize common forms of bias and become familiar with methods (both internal and external) to minimize them.
Diagnostic errors account for a significant cause of patient morbidity and mortality and are an understandable source of anxiety for patients, clinicians, and radiologists alike. The contribution of cognitive bias to diagnostic errors within radiology is well de- scribed, with Garland [1] first discussing differences in interpretations of chest radiographs. Since then, research has delved into the potential causes of diagnostic error and provided insight and a framework for understanding the basis of these errors and potential avenues for mitigation [2].
Cognitive Processes
Kanehman’s [3] Nobel prize-winning work first described critical concepts to understand cognition. In this framework, decision making can be divided into type 1 thinking (heuristics) and type 2 thinking (logic). Type 1 thinking is quick and involves mental shortcuts [4]; it is the muscle memory or gut reaction thinking necessary to accommodate the flood of millions of bits of sensory information processed by the brain at any given moment. Type 1 thinking allows one to make split-second decisions using limited available information, often based on experience, but it is also highly susceptible to cognitive bias. Type 2 thinking is slower and more deliberate. It is often used in completely novel situations. In radiology, an analogy would be the amount of time spent re- viewing a head CT study for the first time by a 1st-year radiology resident. The student would spend a significantly longer time reviewing the study, looking slowly and intentionally for each structure (type 2 thinking), potentially with an inefficient search pattern. Compare this to the amount of type spent by an experienced attending radiologist reviewing the same head CT study. Search patterns in this practitioner have become automatic (type 1 thinking) with attention to high-yield areas for pathologic entities and common blind spots that is based on experience. This muscle memory interpretation is what allows speed and efficiency, but it may also open the door to cognitive errors in diagnosis. A further challenge is that type 1 thinking becomes more common as an individual gets older, as more and more processes become compartmentalized [4]. Although this shift allows greater efficiency, it also creates greater opportunity for cognitive error.
Errors can occur at any time in the process, from initial perception to final image interpretation. In addition to internal fac- tors, systemic sources can also contribute to diagnostic errors in medicine [4, 5]. In this post, common errors along the path from initial perception to final interpretation will be reviewed and potential means for mitigating diagnostic errors will be discussed.
Perceptual Error
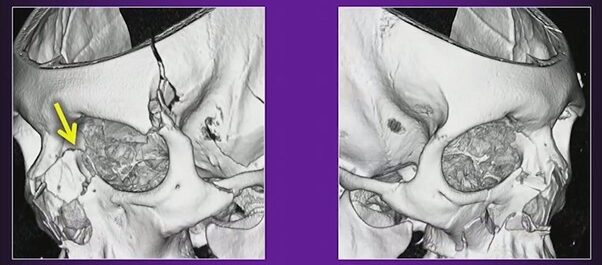
Errors in perception account for a large majority of interpretive errors in radiology. A number of factors contribute to errors in perception such as overall lesion conspicuity, including degree of contrast and border demarcation from adjacent soft tissue [5, 6].
Interpretive Error
More than 30 types of cognitive bias have been described [7]. The most commonly encountered forms of bias in diagnostic im- aging include anchoring bias, confirmation bias, framing bias, availability bias, premature closure, inattentional blindness, and hindsight bias.
Anchoring Bias
Also known as focalism, anchoring bias refers to the common human tendency to place undue influence or anchor on an initial diagnostic impression, despite later information to the contrary [5, 8, 9]. A radiologist’s initial gut reaction to a case, possibly made with limited initial information, can be difficult to deviate from and can potentially lead to useful information being disregarded.
Confirmation Bias
Conceptually related to anchoring bias is confirmation bias. In this case, data supporting an initially suspected diagnosis are sought, and contrary information is given less significance [8, 9]. As a result, diagnoses can be delayed, and potentially unnecessary procedures can be performed [10]. Further, this type of bias may also be encountered in the academic setting with attending radiologist review of preliminary reports by radiology trainees [11].
Framing Bias
In framing bias, different final diagnostic impressions can be made with the same information depending on the presentation of initial clinical information. In clinical context, different conclusions can be drawn from the same imaging study depending on the provided clinical history [10, 12]. Preliminary clinical history can be limited and potentially misleading [13, 14]. Further, the specialty of the referring physician may also be an influencing fac- tor [10].
Availability Bias
In cases of availability bias, recent in- formation is given undue influence in di- agnostic decision making [15]. Recently missed diagnoses may linger in the mind of a radiologist and allow him or her to attribute a rare diagnosis in a case that they may otherwise have not. For example, a radiologist labels a case as “septic arthritis with osteomyelitis” on elbow MRI, only later to find that the case was acute lymphoblastic leukemia. This error might lead the radiologist to diagnose leukemia on more routine cases of osteomyelitis, even with confirmatory laboratory and clinical findings sup- porting that diagnosis [9]. On the opposite end of the spectrum is the concept of non- availability bias; that is, diagnoses that are rarely encountered are rarely considered [9]. A variation of this bias is alliterative error, or satisfaction of report, commonly encountered in radiology as a repeat of a prior report’s impression, even if this might not have been interpreted in the same way de novo. This error has been reported as the fifth most common cause of diagnostic errors by Kim and Mansfield [16].
Premature Closure
Premature closure, the interpretation of initial conclusions as being final, is the overall most common type of error within clinical medicine [12, 17]. This er- ror includes the concept of satisfaction of search, in which an interpretive process is considered finished once an initial abnormality or finding is identified.
Inattentional Blindness
In the case of inattentional blindness, findings may be missed owing to their un- expected nature or their location at the periphery of the image. Corner shot findings on a radiograph or findings on the final im- ages of a cine clip of an ultrasound are examples of potential causes of inattentional blindness [16, 18–20].
Hindsight Bias
Hindsight bias is described as the tendency to de-emphasize the difficulty in making an initial diagnosis after the fact. This bias can occur in group settings including tumor boards, clinical conferences, and medicolegal settings and can prevent realistic assessment of challenges faced with complex initial diagnoses [9, 21].
External Factors
Interruptions are a common occurrence in a busy practice with visiting clinicians, telephone interruptions, and technologist requests. In the face of these interruptions it is easy for radiologists to lose their trains of thought and potentially deviate unknowingly from their typical search patterns. These interruptions have been shown to lengthen interpretation times and reduce accuracy in abnormal cases [22, 23].
Methods of Mitigation
Metacognition
A potential means of partially addressing cognitive bias is the concept of meta- cognition; that is, an individual can evaluate one’s own thought processes [22]. Metacognition involves introspection of one’s thought processes and seeking out- side perspectives.
Minimizing Interruptions
Although radiologists must balance pro- viding high-level service to referring clinicians with efficient use of their time, methods for minimizing interruptions are critical [5, 16]. Employing reading room assistants to field and triage calls can provide a first line of screening for telephone calls to aid in reducing interruptions [24]. Further use of text messaging services can also allow radiologists to communicate findings efficiently and document exact conversations [25].
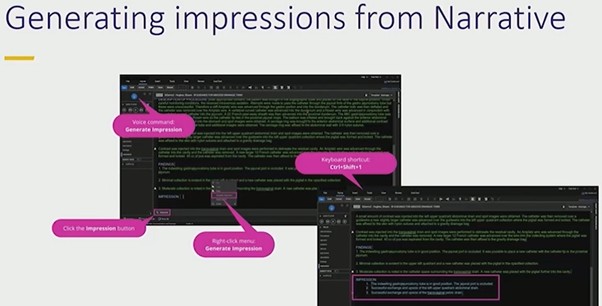
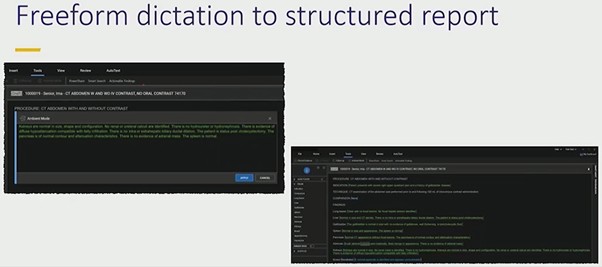
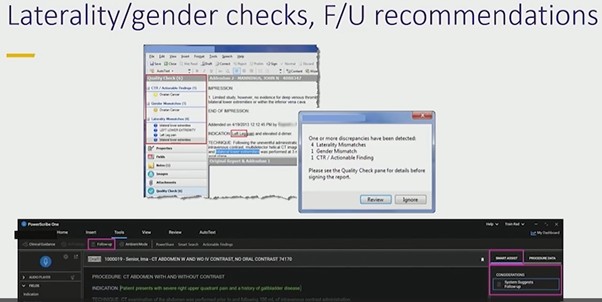
Structured Reporting
Structured reporting provides a check- list-style framework for reporting that al- lows reminders for interpreting radiologists to review all relevant anatomy. For trainees, this process also allows the development of desired interpretive search patterns [26].
Radiologic-Pathologic Review
Follow-up on challenging cases either through quality-control conferences, tumor boards, or personal review of cases is critical for improving and expanding radiologists’ interpretive skills. Supportive and educationally oriented environments can allow meaningful discussion and review of diagnostically challenging cases.
Computer-Aided Diagnostics
Use of increasingly powerful means of computer-aided image interpretation pro- vides another potential tool for radiologists to improve diagnostic accuracy and increase confidence. The current effective- ness of computer-aided detection within areas such as mammography has not been shown to be improved over interpretation without computer-aided detection [27]. However, there is growing potential for ap- plications in multiple other areas with use of neural network–based approaches [28].
The impact of bias in radiologic interpretation can be substantial, with potential implications in patient outcomes. Better understanding the forms of bias, related to both internal and external pressures, can allow radiologists to implement methods for mitigating these biases.
REFERENCES
- Garland LH. Studies on the accuracy of diagnostic procedures. Am J Roentgenol Radium Ther Nucl Med 1959; 82:25–38
- Degnan AJ, Ghobadi EH, Hardy P, et al. Percep- tual and interpretive error in diagnostic radiology: causes and potential solutions. Acad Radiol 2019; 26:833–845
- Tversky A, Kahneman D. Judgment under un- certainty: heuristics and biases. Science 1974; 185:1124–1131
- Durr T. Thinking, fast and slow by Daniel Kahneman. (book review) Am J Educ 2014; 120:287–291
- Waite S, Scott J, Gale B, Fuchs T, Kolla S, Reede D. Interpretive error in radiology. AJR 2017; 208:739–749
- Patel SH, Stanton CL, Miller SG, Patrie JT, Itri JN, Shepherd TM. Risk factors for perceptual-versus- interpretative errors in diagnostic neuroradiology. AJNR 2019; 40:1252–1256
- Rosenkrantz AB, Bansal NK. Diagnostic errors in abdominopelvic CT interpretation: characteriza- tion based on report addenda. Abdom Radiol (NY) 2016; 41:1793–1799
- Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Acad Med 2003; 78:775–780
- Croskerry P. Achieving quality in clinical decision making: cognitive strategies and detection of bias. Acad Emerg Med 2002; 9:1184–1204
- Busby LP, Courtier JL, Glastonbury CM. Bias in radi- ology: the how and why of misses and misinterpre- tations. RadioGraphics 2018; 38:236–247
- Nanapragasam A, Bhatnagar P, Birchall D. Trainee radiologist reports as a source of confirmation bias in radiology. Clin Radiol 2018; 73:1052–1055
- Lee CS, Nagy PG, Weaver SJ, Newman-Toker DE. Cognitive and system factors contributing to diag- nostic errors in radiology. AJR 2013; 201:611–617
- Gunderman RB, Phillips MD, Cohen MD. Improving clinical histories on radiology requisitions. Acad Radiol 2001; 8:299–303
- Loy CT, Irwig L. Accuracy of diagnostic tests read with and without clinical information. JAMA 2004; 292:1602–1609
- Dumitrescu A, Ryan CA. Addressing the taboo of medical error through IGBOs: I got burnt once! Eur J Pediatr 2014; 173:503–508
- Kim YW, Mansfield LT. Fool me twice: delayed diag- noses in radiology with emphasis on perpetuated errors. AJR 2014; 202:465–470
- Graber ML, Franklin N, Gordon R. Diagnostic er- ror in internal medicine. Arch Intern Med 2005; 65:1493–1499
- Drew TH, Võ ML, Wolfe JM. The invisible gorilla strikes again. Psychol Sci 2013; 24:1848–1853
- Beanland V, Pammer K. Gorilla watching: effects of exposure and expectations on inattentional blind- ness. In: 9th Conference of the Australasian Society for Cognitive Science. Sydney, Australia: Macquarie Centre for Cognitive Science, 2010:12–20
- Drew TH, Vo ML, Olwal A, Jacobson F, Seltzer SE, Wolfe JM. Scanners and drillers: characterizing ex- pert visual search through volumetric images. J Vis 2013; 13:3
- Gunderman RB. Biases in radiologic reasoning. AJR 2009; 192:561–564
- Flavell JH. Metacognition and cognitive monitoring: a new area of cognitive-developmental inqui- ry. Am Psychol 1979; 34:906–911
- Wynn RM, Howe JL, Kelahan LC, Fong A, Filice RW, Ratwani RM. The impact of interruptions on chest radiograph interpretation: effects on reading time and accuracy. Acad Radiol 2018; 25:1515–1520
- Ngo JS, Maxfield CM, Schooler GR. The current state of radiology call assistant triage programs among US radiology residency programs. Acad Radiol 2018; 25:250–254
- Torres A, Milov DE, Melendez D, Negron J, Zhao JJ, Lawless ST. A new approach to alarm manage- ment: mitigating failure-prone systems. J Hosp Adm 2014; 3:79–83
- Marcovici PA, Taylor GA. Structured radiology re- ports are more complete and more effective than unstructured reports. AJR 2014; 203:1265–1271
- Lehman CD, Wellman RD, Buist DSM, Kerlikowske K, Tosteson ANA, Miglioretti DL. Diagnostic accuracy of digital screening mammography with and with- out computer-aided detection. JAMA Intern Med 2015; 175:1828
- Taylor AG, Mielke C, Mongan J. Automated detection of moderate and large pneumothorax on frontal chest X-rays using deep convolutional neural networks: a retrospective study. PLoS Med 2018; 15:e1002697
Jesse Courtier, MD
Department of Radiology
UCSF Benioff Children’s Hospital