A member of the Radiology Health Equity Coalition (RHEC), ARRS continues to collaborate with RHEC on curating and disseminating trusted resources and best practices for improving access to and utilization of preventive and diagnostic imaging.
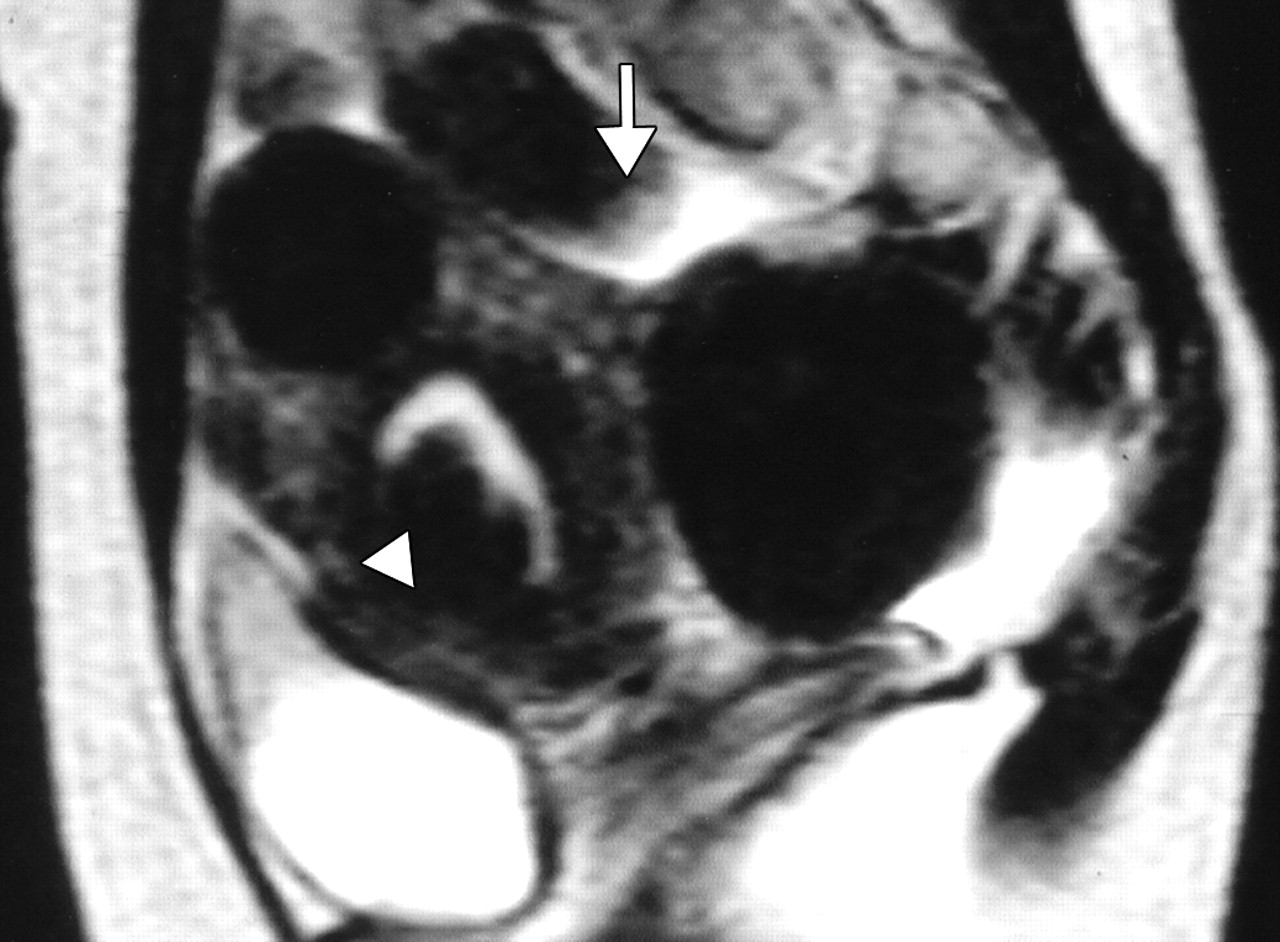
Uterine fibroids are benign tumors that develop in the uterus. While common among all women, fibroids disproportionately affect women of color. Fibroids are the leading cause of hysterectomy, with the average age of women undergoing this major surgery being just 39 years old (Fig. 1).
Fig. 1—44-year- old woman with menorrhagia and bulk-related symptoms caused by multiple uterine fibroids. T2-weighted MR image obtained before embolization reveals submucosal fibroid (arrowhead) and pedunculated subserosal fibroid 6 cm in maximal diameter. Diameter of stalk (arrow) is 2 cm.
Why Patients Should Consider Uterine Fibroid Embolization
UFE offers numerous benefits compared to hysterectomy or other surgical options:
Minimally Invasive
Performed by an interventional radiologist, UFE involves no surgical incisions
Outpatient Procedure
Patients typically go home the same day
Shorter Recovery Time
Recovery from UFE takes only 5–7 days compared to the 6–8 weeks often required after a hysterectomy
Uterus Preservation
Unlike a hysterectomy, UFE allows women to keep their uterus, maintaining their fertility and hormonal balance
Safe and Effective
UFE has a success rate of 90%, providing relief from fibroid symptoms like heavy menstrual bleeding, pelvic pain, and increased urinary frequency (Fig. 2)
Fig. 2—44-year- old woman with menorrhagia and bulk-related symptoms caused by multiple uterine fibroids. Contrast-enhanced T1-weighted MR image obtained 1 year after embolization reveals pedunculated subserosal fibroid, now 4.5 cm in maximal diameter, is not enhancing. Diameter of stalk (arrow) is now 1.1 cm. Rate of volume reduction in pedunculated subserosal fibroid is 61%. Menorrhagia and bulk-related symptoms markedly improved.
Why Keeping Your Patient’s Uterus Matters
Even for women not planning to have children, the uterus plays a vital role in overall health. Removing the uterus through hysterectomy can lead to serious complications, such as:
Psychological distress (often compared to the emotional impact of castration in men)
Sexual dysfunction, including reduced libido and loss of orgasm
Urinary incontinence
Significant bone loss
Increased risks of high blood pressure, heart attack, and stroke
Nearly all patients who qualify for surgery are also candidates for UFE, and UFE is covered by all major insurance providers, including Medicare and Medicaid.
Artificial intelligence (AI) now impacts radiologists at all stages of training and in all practice settings. Every day, radiologists hear of new opportunities and new challenges that AI will bring to their work and lives. Most practicing radiologists, and many radiologists in training, have not received the education necessary to navigate this new world, discern truth from hype, and recognize the dangers and responsibilities facing them as they integrate these systems into hospitals and clinics.
In order to safely, responsibly, and successfully develop, implement, and use AI systems to improve patient care and our work lives, radiologists must learn the basics in key areas. On Sunday, April 27 during the 2025 ARRS Annual Meeting at Marriott Marquis San Diego Marina, “Critical Education for Safe, Ethical, and Successful AI in Radiology” will provide expert guidance in:
Reliable AI: From Research to Production;
Practical AI: Implementation, Workflow and Monitoring;
Successful AI: Product Development, Validation, and Regulation;
Ethical AI: Bias, Diversity, Accessibility, and Privacy.
Most practicing radiologists have not received basic, trustworthy education that will allow them to understand, assess, implement, and successfully utilize AI products in their practices. Training programs now offer basic education about AI, but this often lacks teaching from those with broad experience and the ability to provide a comprehensive overview, including research, ethics, clinical implementation, and the business and economics of AI. Radiologists in practice and in training must be prepared to evaluate products, understand the important role of standards for AI integration into workflow, and be aware of pitfalls and dangers that could harm patients and the practice if not recognized. Led by course director Wende Gibbs, MD, attendees of “Critical Education for Safe, Ethical, and Successful AI in Radiology” will benefit from the unique group of speakers who are trailblazers in the areas of AI research, education, and business, and current and future leaders who are breaking down silos and facilitating multidisciplinary, multispecialty cooperation in the creation of safe, successful, and ethical AI for all.
Later in the afternoon on Sunday, April 27 in San Diego, CA, “Clinical Implementation of AI” will provide a timely review of best practices for selecting and a primer for deploying AI products to maximize return on investment. Course director Manisha Bahl, MD, has assembled four leading researchers in AI who also practice in different subspecialties. Their goal? Enhancing the overall value of any AI system by streamlining clinical workflows, while instilling effective methodology for monitoring said system’s practical impacts. Combining expert-led lectures with an interactive Q&A session, this ARRS Annual Meeting Sunday Session is open to all registrants.
Going into 2025—the 125th anniversary of the American Roentgen Ray Society (ARRS)—I will be using my remaining InPractice columns as your president to provide more context regarding working happier as a radiologist. Centered in worker voice and equity, the happy radiologist is connected most to a safe and secure community—where everything from mentorship to scheduling works together to help foster a true sense of belonging. Opportunities for learning and accomplishment afford radiologists a dignity and meaning beyond our workstations, too.But let us start in 2022. I think we can all remember then. In the wake of the COVID pandemic, the United States Surgeon General, Dr. Vivek Murthy, released an updated framework for mental health and wellbeing in the workplace, outlining the foundational roles that workplaces must play in promoting health and wellbeing alike in our communities [1]. The U.S. Department of Health and Human Services was formally recognizing that our health care industries had to start focusing on working well. I want to share an accompanying figure from this federal framework with InPractice readers because it provides a great platform to think about ground-up, actionable initiatives that could work for our own specific radiological workplaces (Fig. 1).
Fig. 1—The five essentials for workplace mental health and wellbeing help organizations develop, institutionalize, and update policies, processes, and practices that best support the mental health and wellbeing of all workers.
Let’s turn our attention to the right side of this graphic: specifically, making connections and belonging to a community. The first step here is developing a culture. What does your chair or section chief value? What does your CEO treasure? We always talk about mission and vision, and answering these big questions are critically important to those conversations. Personally, I would like to know what my chair and my section value. And what are their goals for my own department? Additionally, what resources are our leaders able to provide to ground us in the institution’s values?
Lately, I’ve been looking at how the social supports of community are connected to a crucial distinction that the Surgeon General’s chart makes here. At the end of the workday, it’s not really a “balance” between that work and our lives at home. It is much more about work-life “harmony,” which Dr. Murthy’s office also notes is based in autonomy and flexibility.
When I was in training, we worked from seven to six o’clock, and then, we’d call from six o’clock to the next morning. Our schedule was rigid. It didn’t allow for a family, much less proper family time. During residency, I didn’t even go to the dentist; I simply didn’t have the time! And as a fellow, I remember tearing up when I got home from a RiteAid, of all places. I was crying because I’d never taken enough care of myself to go and buy products. I was just working so hard.
Given all the types of scheduling we have now, there are such wonderful opportunities with shift work. In January, our group moved to shift-type areas, where some people arrive at noon, some people come in at 4pm. This flexibility has provided a lot of satisfaction for our group, as directors have empowered us to choose the shifts that best fit our lives at that moment.
Moving clockwise, you’ll notice another essential element of working happier. Everyone reading this piece right now is a leader, or a valued member of a group with a leader at the helm. So, how do good leaders accommodate the group’s varied interests, while making individuals feel that they matter? In an academic setting, we can further foster flexibility with research and education, especially subspecialty experience. As you know, data have come out noting that if only 20% of your workday is spent doing something you like, you will be a much happier worker.
For me, my happiness at work is temporal bone. When I see a temporal bone case, I just start smiling because it brings me such great joy. Of course, our colleagues are happier when they’re reading cases that spark joy, so until next time, let’s really think about related worklist opportunities. I’ve seen some creative solutions in which worklists are done not by modality, but by image or imaging interests. Overall, reported happiness is much higher.
Athanasios Pavlou, MD University of Maryland School of Medicine R Adams Cowley Shock Trauma Center
Patient History
31-year-old female with no significant past medical history presented with multiple injuries after a motor vehicle accident. On arrival, the patient was conscious and moving her upper extremities but progressively developed lethargy.
Imaging Findings—Radiographs and CT Scan
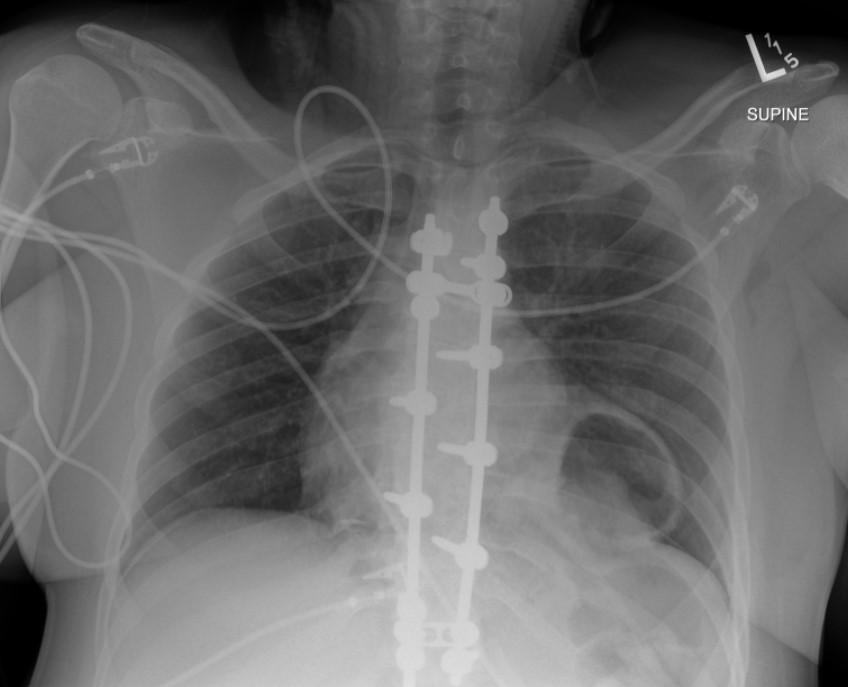
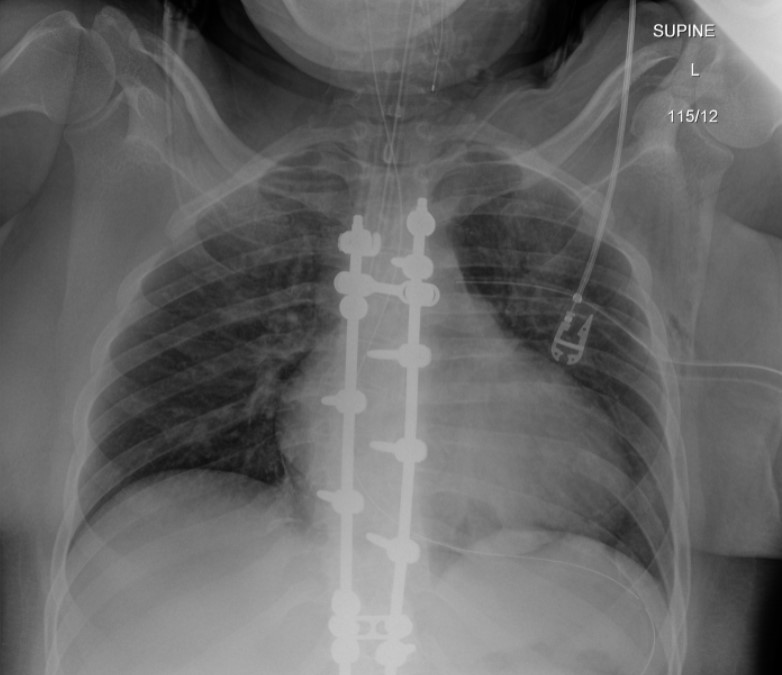
The initial chest radiograph (Figure 1) demonstrated a rounded retrocardiac partially lucent mass interpreted as a hiatal hernia.
Fig. 1—Initial radiograph showing retrocardiac partially lucent mass
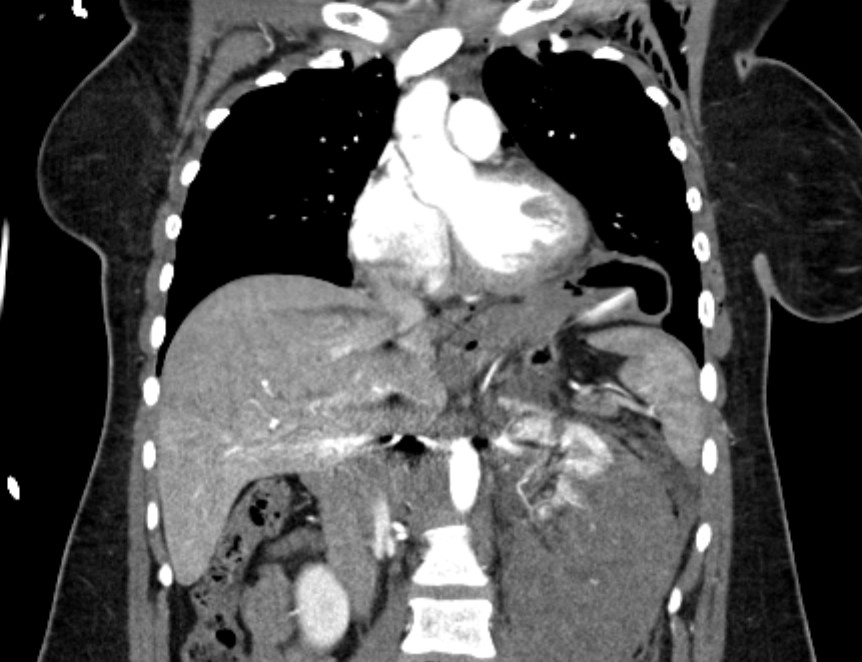
CT scan (Figure 2) revealed multiple clinically significant injuries, including a high-grade left renal injury. The stomach was elevated into the left hemithorax which was interpreted as the consequence of diaphragmatic eventration; medial diaphragm free edge was not appreciated.
Fig. 2—CT scan showing stomach herniating into left hemithorax
Postintubation radiograph (Figure 3) showed resolution of the retrocardiac mass with normal appearance of the diaphragm contour.
Fig. 3—Radiograph after intubation showing resolution of retrocardiac lucency
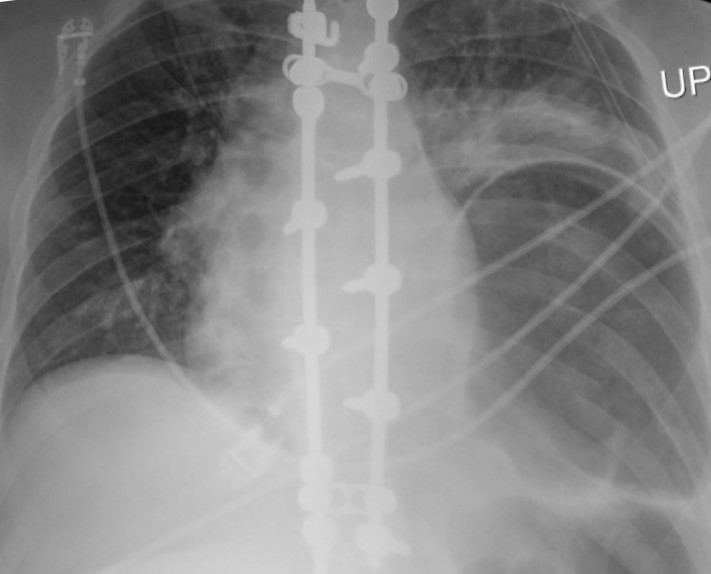
The patient subsequently underwent laparotomy for surgical repair of the renal injury. The follow-up radiograph (Figure 4) after extubation showed a recurrent lower left hemithorax partially lucent mass, increased in size compared to the initial radiograph.
Fig. 4— Radiograph postextubation showing recurrent large lower left hemithorax partially lucent mass
Which Is the Correct Diagnosis? Click on the arrows to reveal the correct answer.
Phrenic Nerve Injury
Incorrect. Please try again.
Congenital diaphragmatic hernia
Incorrect. Please try again.
Traumatic diaphragmatic injury
Correct! Read Further Discussion for more details.
Intraoperative diaphragmatic injury
Incorrect. Please try again.
Further Discussion
Traumatic diaphragmatic ruptures are infrequent with a reported incidence of 0.8-8% in patients who suffer blunt diaphragmatic trauma. They more commonly involve the posterolateral aspect of the left hemidiaphragm. Reported symptoms include chest or abdominal pain, dyspnea, cough, and even a presentation of hemodynamic instability.
The main radiographic finding suggesting diaphragmatic injury is the elevation of the “diaphragmatic contour” either with or without visualization of a herniating hollow viscus. This may be difficult to differentiate from preexisting hiatal hernia, basilar atelectasis, diaphragmatic eventration, congenital hernias, and phrenic nerve injury which may have a similar appearance. Furthermore, as with our case, positive pressure ventilation may lead to delayed diagnosis due to temporary reduction of the intraabdominal contents. The reported rate of missed diaphragmatic injury on chest radiographs is variable and ranges from 12 to 66%. CT has higher sensitivity and specificity for the diagnosis of diaphragmatic injuries. CT findings include visualization of the discontinuity of the diaphragm (73% sensitivity, 90% specificity), intrathoracic herniation of viscera (55% sensitivity,100% specificity), the collar sign (63% sensitivity, 100% specificity), which refers to a waist like constriction of the herniated viscera where it extends through the diaphragmatic defect, and the dependent viscera sign (90% sensitivity, 100% specificity) which describes the positioning of the abdominal viscera directly anterior to the posterior ribs due to loss of the diaphragmatic structural support.
Management of blunt diaphragmatic injury is surgical repair. Laparotomy or thoracotomy with direct suturing or surgical mesh is the mainstay of treatment.
The prognosis is favorable if diagnosed early and repaired. Missed injuries can lead to delayed herniation of abdominal viscera with resulting morbidity and mortality due to the risk of strangulation.
Points InPractice
Radiographic diagnosis of blunt left diaphragmatic injury may be suggested by elevation of the “diaphragmatic contour,” which can be misinterpreted as the result of other abnormalities.
Positive pressure ventilation can reduce the herniated viscera into the abdominal cavity and conceal the radiographic findings of a diaphragmatic injury.
In the setting of acute trauma, CT finding of intrathoracic herniation of abdominal contents has very high specificity for diaphragmatic injury and should be managed as such until proven otherwise.
References
Hammer MM, Raptis DA, Mellnick VM, et al. Traumatic injuries of the diaphragm: overview of imaging findings and diagnosis. Abdom Radiol 2017; 42:1020–1027
Iochum S, Ludig T, Walter F, et al. Imaging of diaphragmatic injury: a diagnostic challenge? RadioGraphics 2002; 22:S103–S116
Sliker CW. Imaging of diaphragm injuries. Radiol Clin N America 2006; 44:199–211
Zarour AM, El-Menyar A, Al-Thani H, et al. Presentations and outcomes in patients with traumatic diaphragmatic injury: a 15-year experience. Journ Trauma Acute Care Surg 2013; 74:1392–1398
McDonald AA, Robinson BRH, Alarcon L, et al. Evaluation and management of traumatic diaphragmatic injuries: a practice management guideline from the Eastern Association for the Surgery of Trauma. Journ Trauma Acute Care Surg 2018; 85:198–207
Min Lang, MD, MSc Department of Radiology, Massachusetts General Hospital Harvard Medical School
John Conklin, MD, MS Department of Radiology, Massachusetts General Hospital Harvard Medical School
Claire White-Dzuro, MD Vanderbilt School of Medicine
Neuroimaging plays a truly critical role in the initial evaluation of acute stroke. Although noncontrast head CT, followed by CT angiography (CTA), has historically been the standard imaging algorithm, it is well established in the literature and clinically that MRI is more sensitive for diagnosing acute ischemic stroke. Specific MRI sequences can provide vital information to help guide patient treatment decisions, especially for those with delayed presentation. For example, diffusion-weighted imaging (DWI) and fluid-attenuated inversion recovery (FLAIR) sequences often offer a better estimate for the onset of ischemia in patients with wake-up stroke.
As noted in our original AJR manuscript, “Triage of Patients With Acute Stroke for Endovascular Therapy: Point—Moving Toward MRI-Based Acute Stroke Triage With Ultrafast Protocols [1],” identification of DWI and FLAIR mismatch on MRI is suggestive of ischemic stroke with a duration of less than 4.5 hours, which is an important patient selection criterion for IV tissue-plasminogen activator (tPA). Additionally, MRI remains superior to CT perfusion imaging (CTP) for assessment of parenchymal integrity, tissue viability, and ischemic core—all of which can help determine thrombectomy and late-window thrombolysis candidacy.
Despite MRI’s superiority, CT remains the most commonly performed exam for code-stroke evaluation for two reasons. First, CT scanners continue to be much more accessible than MRI machines in emergency department (ED) and inpatient settings. Secondly, the imaging time for a head CT is on the order of seconds, whereas a brain MRI typically takes 10-15 minutes, depending upon which sequences are included in the protocol. The longer scan time for MRI results in the patient being more prone to motion, which could degrade the examination’s sensitivity.
Yes, we learned from the THRACE (Mechanical Thrombectomy After Intravenous Alteplase Versus Alteplase Alone After Stroke) Trial that there was a significant difference in acquisition time of a few minutes between patients who underwent CT versus MRI as their first imaging examination [2]. However, this slight delay in acquisition did not impact workflow or outcomes. And while CT remains the faster modality, when it is paired with additional imaging (e.g., CTA and CTP), overall imaging time ends up similar to MRI.
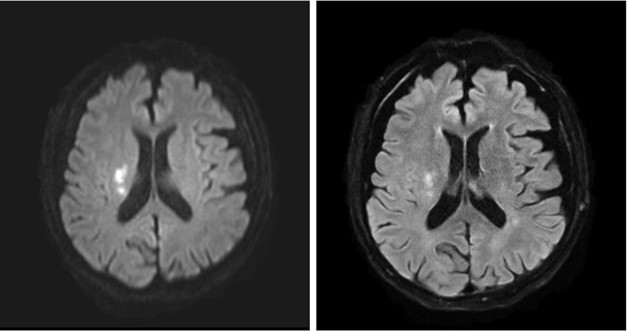
MRI’s intrinsic advantages over CT for evaluating acute infarction, as well as ongoing technological advances, have led to increases in MRI utilization within the ED: 38% from 1999 to 2008, though a more modest 18% from 2012 to 2019 [3-4]. (An increasing number of hospitals are moving toward 24/7 on-site MRI availability to obtain certification from The Joint Commission for Comprehensive Stroke Center, too.) In addition, newer ultrafast brain MRI protocols—comprised of T2/T2*-weighted, FLAIR, and DWI sequences—have been developed to further reduce acquisition times and increase the modality’s accessibility for acute stroke evaluation (Fig. 1).
Fig. 1—Images from axial ultrafast DWI sequence (left) of 21 seconds and axial ultrafast FLAIR sequence (right) of 51 seconds show clear diffusion restriction and T2-FLAIR hyperintensity, respectively, in right corona radiata, consistent with late-acute to early-subacute infarct.
The total acquisition time of the ultrafast brain MRI protocol is approximately 2-3 minutes. This ultrafast protocol uses the multi-shot echoplanar imaging (EPI) technique, a highly efficient interleaved EPI technique using multiple excitations, to decrease geometric distortion and increase SNR. Recent clinical validation of the ultrafast brain MRI protocol published in the American Journal of Neuroradiology showed similar sensitivity for detecting acute intracranial findings and acute ischemic infarct as compared to standard brain MRI protocol [5]. Motion artifacts were also significantly reduced on the ultrafast protocol images. Application of deep learning-assisted reconstruction techniques will only continue to improve image quality and SNR, increasing the confidence of radiologists’ interpretations.
CT will remain the first imaging modality for any unstable patient, as well as for patients where MRI is contraindicated or where a facility faces limited scanner availability. But look at all the benefits of choosing MRI over CT for initial acute infarct screening, including:
Differentiating stroke from mimickers
Migraine
Seizure
Demyelinating process
Infection
Neoplastic process
No radiation
Lower risk for hypersensitivity reaction to gadolinium-based contrast agents
To conclude, with newer MR acceleration techniques, ultrafast MRI-based acute stroke evaluation has been shown to be fast, safe, and accurate. Therefore, MRI should be considered a suitable initial triage imaging modality for the appropriate patient and facility.
References
Lang M, Conklin J. Triage of patients with acute stroke for endovascular therapy: point—moving toward MRI-based acute stroke triage with ultrafast protocols. AJR May 2024. doi: 10.2214/AJR.24.31303
Provost C, Soudant M, Legrand L, et al. Magnetic resonance imaging or computed tomography before treatment in acute ischemic stroke. Stroke 2019; 50:659-664
Burke JF, Kerber KA, Iwashyna TJ, Morgenstern LB. Wide variation and rising utilization of stroke magnetic resonance imaging: data from 11 states. Ann Neurol 2012; 71:179-85
Wang JJ, Pelzl CE, Boltyenkov A, et al. Updated trends, disparities, and clinical impact of neuroimaging utilization in ischemic stroke in the Medicare population: 2012 to 2019. J Am Coll Radiol 2022; 19:854-865
Lang M, Clifford B, Lo WC, et al. Clinical evaluation of a 2-minute ultrafast brain MR protocol for evaluation of acute pathology in the emergency and inpatient settings. Am J Neuroradiol Mar 2024. doi:10.3174/ajnr.A8143
Katerina Dodelzon, MD, FSBI Associate Professor of Clinical Radiology Associate Director Breast Imaging Fellowship Vice Chair of Clinical Operations Weill Cornell Medicine
Physician burnout was its own epidemic, with radiologists consistently ranking among the most burned-out medical specialties, well before the COVID pandemic. The acute and now chronic stressors of COVID further exacerbated radiologists’ wellness with 54% of radiologists reporting symptoms of burnout, according to a recent Medscape report [1]. In addition to radiologists’ wellness, burnout has significant adverse implications on patient care and outcomes [2].
In its most simplistic dissection, burnout is composed of three parts:
Depersonalization
Physical and emotional exhaustion
Low sense of personal accomplishment
As such, the very fundamental aspect of our job as physicians, that of connecting and communicating with patients, may play a central role in physician wellness. A direct association can be observed between physicians’ level of satisfaction with their job and their ability to build rapport and connect with patients [3]. Rapport and relationship building both decrease depersonalization and increase a sense of personal accomplishment. Although anxiety related to challenging physician interactions, which have been shown to last for days beyond the interaction, can lead to fatigue, if cumulative, these interactions may lead to exhaustion [4]. Furthermore, anxiety surrounding challenging patient interactions, like delivering bad news, is more likely to occur if one is faced with such interactions infrequently, and thus feel unprepared or unskilled to navigate them.
Demonstrating the critical impact of patient-physician communication interaction on physician mental health, a recent national study of breast radiologists’ wellness found that less time spent connecting with, educating, and consulting patients was statistically significantly associated with greater odds of reporting psychological distress and anxiety [5]. Interestingly, although increase in frequency of more negative and charged patient interactions were reported by some radiologists in the study, no association between negative interactions and mental health was found. Therefore, it appears that it’s the length of time allotted for physicians to build rapport and make meaningful connections with their patients to educate and inform, rather than the nature of the interactions themselves, which significantly affects radiologists’ wellness.
As institutions, practices, and individual physicians devise strategies for burnout mitigation, time and adequate focus should be allotted to patient-centered communication. Operational leadership should be intentional in incorporating sufficient time for radiologists to discuss results and consult with patients into the daily workflow, not limiting interactions in favor of increased volume. Communication skill training should be increasingly integrated into radiology training curricula. In addition, training and effective communication skill resources should be emphasized and made readily available for all faculty to equip radiologists with the confidence to approach a variety of challenging patient interactions, thus diminishing communication-related anxiety [6]. Radiologists, themselves, should emerge from behind the workstation, seeking out opportunities to consult and educate patients—as our very own wellbeing depends on it.
Panagioti M, Geraghty K, Johnson J, et al. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med 2018; 178:1317–1331
West CP, Dyrbye LN, Shanafelt TD. (Mayo Clinic, Rochester, MN; and Stanford University Medical Center, Stanford, CA, USA). Physician burnout: contributors, consequences and solutions (Review). J Intern Med 2018; 283:516–529
Ptacek J, Fries E, Eberhardt T, et al. Breaking bad news to patients: physicians’ perceptions of the process. Support Care Cancer 1999; 7:113–120
Dodelzon K, Grimm LJ, Plimpton SR, et al. Ongoing impact of COVID-19 on breast radiologists’ wellness. Journ Breast Imag 2023; 3:287–296
Dale West, CAE, has been named incoming Executive Director for the American Roentgen Ray Society (ARRS). West will serve as the administrative and strategic partner to the ARRS Executive Council, overseeing day-to-day operations of the Society, as well as the financial and business operations of the Society’s products and service offerings.
“Dale West has led health care associations to achieve operating excellence and strategic success,” said Angelisa M. Paladin, MD, 2024-2025 ARRS President.
“Dale is skilled in creating growth strategies, ensuring operational efficiencies, driving change, and effectively staffing teams with the talent and drive to achieve our Society’s mission and goals,” Dr. Paladin continued.
Dale West has a strong and established history of successfully developing vibrant association communities, working collaboratively with Boards of Directors, and guiding cross-functional teams to exceed the objectives of the associations he supports.
Currently, West serves as Vice President of the Health Care Clinical and Administrative Unit and Executive Director of the Commission on Accreditation of Athletic Training Education at Smithbucklin, the world’s largest association management company.
“I am truly honored to join the American Roentgen Ray Society as its new Executive Director,” Dale West said.
“ARRS has a rich legacy, and I am excited to work with our dedicated volunteers and staff to build on that success. We will strengthen our community and advance our mission and the field. I am excited about the opportunities ahead and look forward to what we will accomplish in the coming years.”
“Among a field of outstanding candidates, Dale rose to the top,” noted Erik K. Paulson, MD, chair of the search committee and past president of ARRS.
“We are delighted to move forward with him as our new Executive Director,” Dr. Paulson added.
Dale West officially assumes the position on January 2, 2025—following the retirement of longtime ARRS Executive Director, Susan B. Cappitelli, MBA, CAE. The American Roentgen Ray Society thanks Susan for her many years of exceptional service and contributions, always prioritizing member service and the advancement of the specialty.
The American Roentgen Ray Society (ARRS) is pleased to announce Erin Alaia of NYU Langone Health in New York City as the 2025 Melvin M. Figley Fellow in Radiology Journalism. ARRS also recognizes Domen Plut from Slovenia’s University Medical Centre Ljubljana as the 2025 Lee F. Rogers International Fellow in Radiology Journalism.
Supported by The Roentgen Fund® and named for two distinguished Editors Emeriti of ARRS’ own American Journal of Roentgenology (AJR), the Melvin Figley and Lee Rogers Fellowships offer practicing radiologists an unparalleled opportunity to learn the tenets of medical publishing via “the yellow journal”—the world’s longest continuously published radiology journal. Through hands-on experience with ARRS staff and AJR personnel—as well as personal apprenticeship with AJR’s 13th Editor of Chief, Andrew B. Rosenkrantz—Drs. Alaia and Plut will receive expert instruction in scientific writing and communication, manuscript preparation and editing, peer review processes, journalism ethics, and digital publication.
Additionally, Drs. Alaia and Plut will attend the 2025 ARRS Annual Meeting in San Diego, CA, where they will co-present the AJR Year in Review Sunday Session and participate in the Editor’s Forum.
Founded in 1907, AJR is one of the specialty’s leading peer-reviewed journals, publishing clinically oriented content across all imaging subspecialties and modalities relevant to radiologists’ daily practice. Publishing hundreds of articles annually in a diverse range of formats, including original research, reviews, clinical perspectives, editorials, and other short reports, AJR further engages its audience through a spectrum of social media and digital communication activities. In 2023, the journal garnered 32,133 citations and received an impact factor of 4.7, placing AJR at the 89.5th percentile in the radiology, nuclear medicine, and medical imaging category (as reported by Clarivate Analytics).
Since 1990, The Roentgen Fund has granted millions of dollars to hundreds of imaging professionals for both research pursuits and professional development. Today, through six vital scholarship and fellowship programs, the generosity of The Roentgen Fund’s donors is channeled to every corner of the globe—establishing dual foundations in innovation and leadership for a true diversity of radiology’s next generation.
Erin F. Alaia, MD, is an associate professor of radiology and orthopedic surgery at NYU Langone Health in New York, NY. Chair of ARRS’ Radiology Review Track Musculoskeletal Imaging Section, her research, clinical interests, and areas of expertise include sports imaging, postoperative sports imaging, and musculoskeletal infection. As the recipient of a 2022 Research Seed Grant from the Radiological Society of North America, Dr. Alaia focused on the utility and cost-effectiveness of MRI in older patients with hip and knee pain. Prior chair of the Society of Skeletal Radiology Research Committee, presently, she serves on the consulting editorial board of Skeletal Radiology, having received certificates of distinction for her contributions as a reviewer from 2021-2023. Guest editor for an upcoming issue of Seminars in Musculoskeletal Radiology focused on post-operative imaging, Dr. Alaia is also a member of the American College of Radiology’s Committee on Body Imaging, Musculoskeletal Section.
Domen Plut, MD, PhD, completed his medical studies and radiology residency at the University of Ljubljana’s Faculty of Medicine and University Medical Centre Ljubljana in Slovenia. In 2021, he received the European diploma in pediatric radiology, marking him among the first generation in this subspecialty on the continent. In 2022, Dr. Plut was appointed assistant editor at AJR. An assistant professor at the Medical Faculty of Ljubljana, chief of University Medical Centre Ljubljana’s pediatric radiology department, and recipient of the 2023 Lavrič “Best Teacher” Award, teaching is his passion. Dr. Plut is extensively involved in research, having published 45 articles in reputable journals—28 as first or lead author—and serving as a reviewer for many other publications. General Secretary of the Slovenian Association of Radiology and a member of both the European Society of Radiology and European Society of Paediatric Radiology (ESPR), he is a part of ESPR’s Musculoskeletal and Cardiothoracic Taskforce. Dr. Plut’s primary work and research interests include imaging of neonates and contrast-enhanced ultrasound, and he has presented his findings at numerous international radiology conferences, including several annual meetings of the ESPR and Radiological Society of North America.
ARRS Scholar Update: Steven Rothenberg
Steven Rothenberg, MD, is in the second year of his ARRS Scholarship program, investigating methods for mitigating the nocebo effect in diagnostic reporting of lumbar spine MRI. Currently, he is recruiting for his first prospective randomized controlled clinical trial: NCT06103474. Since receiving his ARRS Scholarship during the 2023 ARRS Annual Meeting in Honolulu, HI, Dr. Rothenberg has been awarded Most Prolific Inventor by the Herbert Institute for Innovation and Entrepreneurship and the Light Bulb Award from the University of Alabama at Birmingham’s radiology department. His submission of eight invention disclosures have led to three distinct patent applications and one notice of allowance (US20240257947A1) from the United States Patent and Trademark Office. Meanwhile, Dr. Rothenberg’s research findings have yielded five co-authored published articles, two related editorials, and two AJR Original Research manuscripts presently in press. As an ARRS Scholar, thus far, he has presented 19 scientific abstracts, earning a Certificate of Merit during the 2024 ARRS Annual Meeting in Boston, MA. Dr. Rothenberg continues to donate to The Roentgen Fund to give back in support of other early-stage faculty applying for future ARRS Scholarships.
Steven Rothenberg, MD, is in the second year of his ARRS Scholarship program, investigating methods for mitigating the nocebo effect in diagnostic reporting of lumbar spine MRI. Currently, he is recruiting for his first prospective randomized controlled clinical trial: NCT06103474. Since receiving his ARRS Scholarship during the 2023 ARRS Annual Meeting in Honolulu, HI, Dr. Rothenberg has been awarded Most Prolific Inventor by the Herbert Institute for Innovation and Entrepreneurship and the Light Bulb Award from the University of Alabama at Birmingham’s radiology department. His submission of eight invention disclosures have led to three distinct patent applications and one notice of allowance (US20240257947A1) from the United States Patent and Trademark Office. Meanwhile, Dr. Rothenberg’s research findings have yielded five co-authored published articles, two related editorials, and two AJR Original Research manuscripts presently in press. As an ARRS Scholar, thus far, he has presented 19 scientific abstracts, earning a Certificate of Merit during the 2024 ARRS Annual Meeting in Boston, MA. Dr. Rothenberg continues to donate to The Roentgen Fund to give back in support of other early-stage faculty applying for future ARRS Scholarships.
2023 ARRS Scholars Andrew Wentland, assistant professor at the University of Wisconsin School of Medicine & Public Health, and Steven Rothenberg, assistant professor at the University of Alabama at Birmingham
The Roentgen Ray Review (R3) website is live: R3journal.org. All R3 social media handles have been staked. And as of July, unsolicited submissions for the American Roentgen Ray Society’s (ARRS) first journal launch since President Teddy Roosevelt was in office are open to everyone. Starting early next year—and coinciding with ARRS’ own 125th anniversary celebration—R3 is poised to publish image-rich, clinically relevant content for one of radiology’s busiest memberships. Our brand-new online journal will post a weekly mix of “Pictorial Essays,” “Clinical Practice Challenges,” “Case Reports,” “Practice Solutions,” and six other types of articles—three of which offer CME credit. Commissioning and curating R3’s pixels will be the charge of John R. Leyendecker, MD, on faculty at the University of Texas Southwestern in Dallas since 2015. His is a name well-known among us. Present ARRS Executive Council member and chair of our Science and Innovation Committee, Dr. Leyendecker’s association with North America’s first radiological society extends back to his in-training days, when he participated in ARRS’ inaugural “Introduction to Research” course during the 1990 Annual Meeting in Boston, MA. He’s done just about everything else at ARRS ever since: reviewing for AJR, writing for InPractice, directing Categorical Courses, etc. ad inf.
In his first InPractice interview as the very first editor of the Roentgen Ray Review, the abdominal radiologist, amateur astronomer, and United States Air Force veteran outlines a vision as clear as day. Responding to our members’ many educational needs, while being respectful of their time, his R3 is one packed with practical, easily digested information that can be applied immediately.
InPractice: Unlike other peer-reviewed journals, which solicit exclusively from presentations delivered during their societies’ respective Annual Meetings, Roentgen Ray Review will be decidedly less gatekept. How does this more ecumenical approach to submissions align with your overall editorial vision?
JRL: Between our Educational Exhibits and Categorical Course chapters, we are very fortunate to have great material presented at our Annual Meeting to solicit for the journal. However, I wanted to include additional categories of articles that might not be reflected in the meeting content and to open the journal to authors who might not be able to attend our meeting. We want the best content for our readers, regardless of where it originates, and I believe including both solicited and unsolicited articles helps accomplish that goal.
IP: For “Pictorial Essays,” images and figures are king. Radiology is an inherently visual speciality, yes, but are there any risks, practical or pedagogical, with paring down background discussions or future implications?
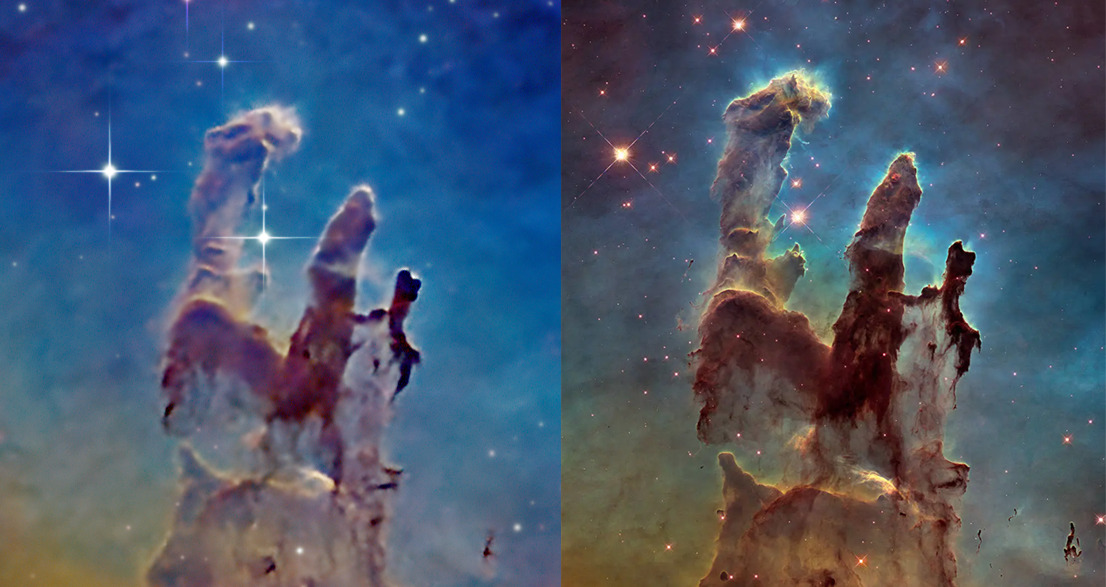
JRL: In-depth details aren’t useful if no one reads them. R3 was born out of a need for relevant content that fits with the realities of today’s busy radiology practices. That’s why we focus on short articles and images. I’m an amateur astronomer, and there is saying in our hobby that the best telescope is the one you use every night (Fig. 1). The same could be said of journals.
Fig. 1—Left: Dr. Leyendecker’s reproduction of the “Pillars of Creation” from the M16 Eagle Nebula…with just an 8-inch diameter backyard telescope! Right: Those same towering tendrils of cosmic dust and gas, care of the Hubble Space Telescope (courtesy of NASA, ESA, and Hubble Heritage Team.)
My goal is to make R3 the go-to journal for our busy members struggling to balance the need to stay current with the many other aspects of life vying for attention. There are only risks with this approach if critical information is withheld in the name of brevity. On the other hand, there might be substantial risk of missing critical information if it is hidden within a barrage of extraneous details. I believe images are an inherently efficient means of conveying information. That’s why emojis are so popular. When images are combined with succinct and relevant text, you have a powerful combination. And for readers wanting more details, there are many options now available online. I want to emphasize, however, that R3 has no intention of dumbing down content or shying away from complex topics. We just want to distill the information prior to consumption. If your typical journal is a pint of lager, we’re like a shot of tequila.
IP: Specific “Clinical Practice Challenge” scenarios will be followed by a question on next steps. Is the multiple-choice format here tailored for the busy radiologist, to mirror portions of the American Board of Radiology (ABR) exam, or something else entirely?
JRL: I include the multiple-choice question to encourage the reader to actively engage with the material and compare what they might do with a content expert’s approach to the scenario. I envision this eventually incorporating a polling function which will allow for comparisons across readers. Of course, there might be some relevance for those taking the current ABR exam, but we aren’t specifically targeting that group. And we certainly don’t want to dredge up any unpleasant memories for our readers who have already taken the exam.
IP: “WTF” is R3’s abbreviation for “What’s That Finding?” Be it new and novel or a fresh take on a classic sign, in the eyes of the editor, what makes for a good “WTF?”
JRL: A good WTF is a new observation, complication, sign, or implanted device that might be unfamiliar to a typical practicing radiologist. Anyone who reads a high volume of imaging examinations can relate to being stumped by something they haven’t encountered before. New devices are constantly being introduced in medicine, and radiologists are not always in the loop when their colleagues start placing them in patients. Novel systemic therapies can be associated with new imaging findings or complications, and recognizing the association between treatment and imaging finding might be critical to management. Finally, new contrast agents or imaging techniques can alter the appearance of an imaging examination or classic sign, and radiologists need to be aware of these alterations so they can appropriately adjust their interpretations. The “WTF” feature of the journal is one means of alerting readers to something new or different that they might encounter, so they can manage their patients appropriately.
IP: Nowadays, so much scholarly content is appearing on preprint repositories—more than 75 at last count. Quality control remains a sticking point, but there is rigorous and robust research, too. Would you reject a submission because it was posted on a preprint server?
JRL: Preprint servers allow authors to quickly disseminate their work and to claim primacy. Since many of our article types are unique, it is unlikely that many of our submissions will have been previously posted on a preprint server. Regardless, our main concern is whether or not an article is under consideration by another journal. There are plenty of reasons to reject an article that has been posted to a preprint server—for example, if the information presented isn’t sufficiently novel, accurate, or relevant. But I don’t think that posting on a preprint server alone would dissuade me publishing a high-quality paper that is not under consideration by another peer-reviewed journal.
IP: Although generative AI is everywhere in biomedical publishing, alas, disclosures and attribution of its use are not. What is the journal’s official stance on using this paradigm-shifting technology, like ChatGPT and its ilk, in drafting an R3 article?
JRL: Authors are not prohibited from using tools such as generative AI to draft their articles for R3. However, they must disclose details of its use and accept full responsibility for whatever the technology produces. In other words, the use of AI does not obviate authors of their responsibility to ensure their manuscripts are accurate, free of plagiarism, and that all appropriate attributions are included. This is one reason why R3 does not recognize AI programs as authors. This might change once humanity is enslaved by its creation.
John R. Leyendecker, MD, is adjunct professor of radiology at UT Southwestern, where he has been a faculty member since 2015. Previously, he served as vice chair of clinical operations, followed by vice chair of academic affairs. Dr. Leyendecker completed his residency at Emory University in 1993, serving as chief resident. In 1994, he completed vascular and interventional radiology fellowship at Wilford Hall United States Air Force (USAF) Medical Center, and after serving an additional six years as an interventional radiologist and abdominal imager in the USAF, Dr. Leyendecker completed body MRI fellowship at the Mallinckrodt Institute in St. Louis, MO. He has since worked clinically as an abdominal imager, while co-authoring two popular textbooks: A Practical Guide to Abdominal and Pelvic MRI and Problem Solving in Abdominal Imaging. Dr. Leyendecker has published numerous peer-reviewed scientific papers and clinical review articles and co-authored many award-winning scientific abstracts and educational exhibits presented at national and international meetings. His ability to distill complex topics and connect with his audience led to speaking engagements around the world, and in 2014, he served as the Society of Abdominal Radiology’s (SAR) Igor Laufer Visiting Professor. For many years, he served as an oral examiner for the American Board of Radiology and was awarded fellowship in the SAR in 2013 and the American College of Radiology in 2021. His intense dedication to educating and elevating his peers and future generations of radiologists has yielded many teaching and mentorship awards. Dr. Leyendecker’s teaching efforts now focus on leadership and emotional intelligence, and in 2022, he was co-recipient of an Association of Academic Radiology Strategic Alignment Grant to develop a nationwide course to cultivate leadership and emotional intelligence skills in early-career radiology faculty.
Department of Diagnostic Imaging, Rhode Island Hospital Warren Alpert Medical School, Brown University
John Scaringi, MD
Department of Diagnostic Imaging, Rhode Island Hospital Warren Alpert Medical School, Brown University
First question: should radiologists really be performing inpatient fludeoxyglucose (FDG) PET/CT? Our recent nuclear medicine editorial in the American Journal of Roentgenology (AJR), “Inpatient FDG PET/CT: Counterpoint—A Costly Yet Subpar Evaluation That Prolongs Hospital Length of Stay,” highlights key problems with this diagnostic pathway [1], as well as why it may be preferably to defer inpatient PET examinations in most clinical scenarios.
No doubt, the volume of imaging studies is increasing nationwide. According to ARRS’ own estimates [2], U.S. radiologists perform some 80 million CTs each year—probably more. Those are just the examinations we are able to track via billing data.
PET/CT is no exception to rising volumes. In fact, one Journal of Nuclear Medicine single-center study reported a greater than five times increase in inpatient PET/CT examinations over a 10-year period at the authors’ institution [3]. Despite the increasing utilization of inpatient PET/CT, the procedure, itself, can be limited by both questionable clinical rationale and poor study quality. Moreover, due to distinct differences in reimbursement between inpatient and outpatient PET procedures, your health care system will likely get paid less for performing inpatient studies.
Quite often, the quality of PET/CT is limited in inpatient settings. Contributing factors to this suboptimal image quality include higher mean blood glucose levels. Patient motion remains a factor, too. As noted in Annals of Nuclear Medicine, acute processes (e.g., infection) also continue to confound our interpretations [4].
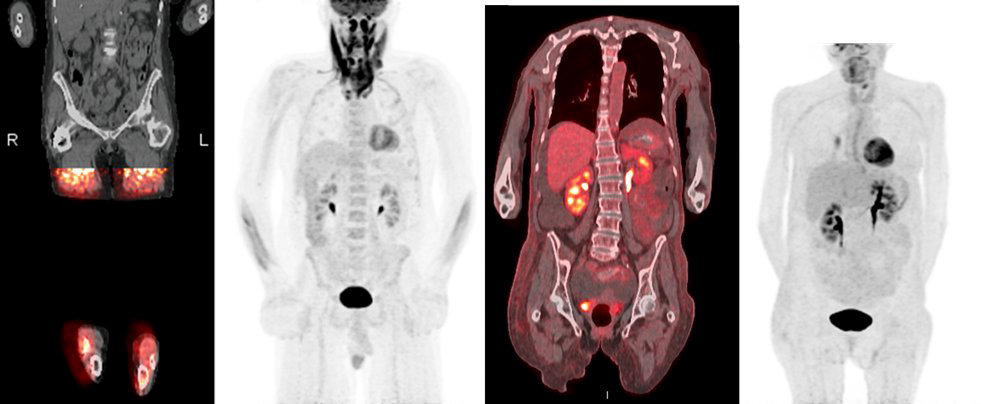
So, another question: what do all three of these FDG PET/CT studies here (Fig. 1) have in common that could be contributing to their poor image quality?
Fig. 1—First patient could not tolerate examination. Second patient suffering from respiratory distress. Third patient receiving course of high-dose steroids, resulting in altered biodistribution of fludeoxyglucose F18.
PET/CT is often ordered on an inpatient basis for initial oncologic staging. However, if there is no plan to initiate treatment while admitted to the hospital, an inpatient PET may only result in a substandard examination, while not changing patient management.
Given that PET/CT examinations are regularly booked weeks in advance, scheduling an inpatient study is challenging, frequently requiring a cancellation in the outpatient setting. This disruption can lead to prolonged patient stays, which increase overall costs and the risk of health care-associated adverse events.
Speaking of cost, inpatient PET/CT is costly to the health care system. Private insurance may not cover an inpatient PET, since the examination is typically viewed as an outpatient study. It is also worth noting that the Centers for Medicare & Medicaid Services bundle inpatient costs—with hospitals possibly receiving reduced or even no payment for high-cost items (i.e., PET/CT).
To reiterate our points, PET/CT in the inpatient setting is a pricey, subpar test that can potentially provide misleading diagnostic information to referring clinicians and patients. With rare exceptions, radiologists should counsel referring providers to skip the inpatient PET…and order an outpatient study instead.
Not everyone agrees with us, of course. For the opposing perspective, we urge you to cross-reference the original AJR Point, “A Strategic Path to Patient-Centered Yet Cost-Effective Care,” by two diagnostic radiologists from Oregon Health & Science University in Portland: Laszlo Szidonya, MD, PhD, and Nadine Mallak, MD [5].
References
Dietsche E, Scaringi J. Inpatient FDG PET/CT: Counterpoint—A Costly Yet Subpar Evaluation That Prolongs Hospital Length of Stay. AJR 2024. Jul; 223:e2330655. doi: 10.2214/AJR.23.30655
Munden RF. Disruptors of the Radiology Workforce—The Next Generation. ARRS InPractice website. www.radfyi.org/2024-arrs-in-training-issue. Published August 12, 2024. Accessed August 16, 2024.
Crandall J, Gajwani P, Wahl R. Trends in Utilization of FDG PET/CT in an Inpatient Population. J Nucl Med 2016. May; 57(suppl 2):1771
Yan X, Kang J, Zhou Y, et al. Imaging Quality of F-18-FDG PET/CT in the Inpatient Versus Outpatient Setting. Ann Nucl Med 2013. Jul; 27:508-14. doi: 10.1007/s12149-013-0714-8
The American Roentgen Ray Society (ARRS) is proud to announce that the Society of Radiologists in Ultrasound (SRU) will present “A Sound Investment: SRU Consensus Statements, 2022–2024” on Sunday, April 27, during the 2025 ARRS Annual Meeting at Marriott Marquis Marina in San Diego, CA.
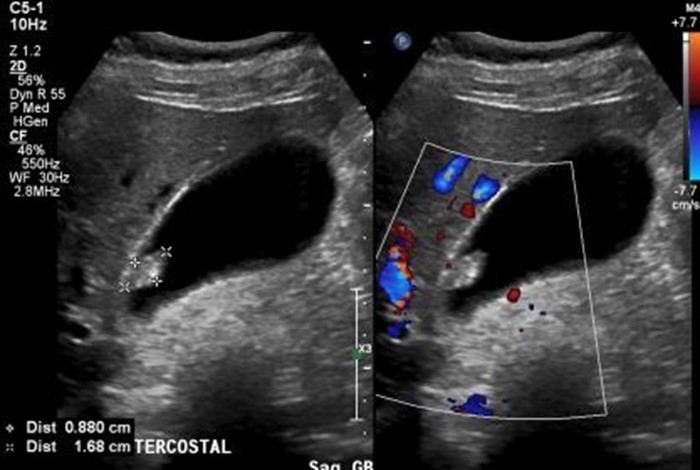
Part of a new SRU initiative, known as “SRU Presents,” this ARRS Featured Session will host the lead author of each of SRU’s four consensus statements [1–4] published over the past two-and-a-half years (Fig. 1), including routine pelvic ultrasound for endometriosis; ultrasonography of superficial soft-tissue masses; management of incidentally detected gallbladder polyps; and a lexicon for first-trimester ultrasound.
Fig. 1—Pathologically proven adenoma with high-grade dysplasia (courtesy of SRU)
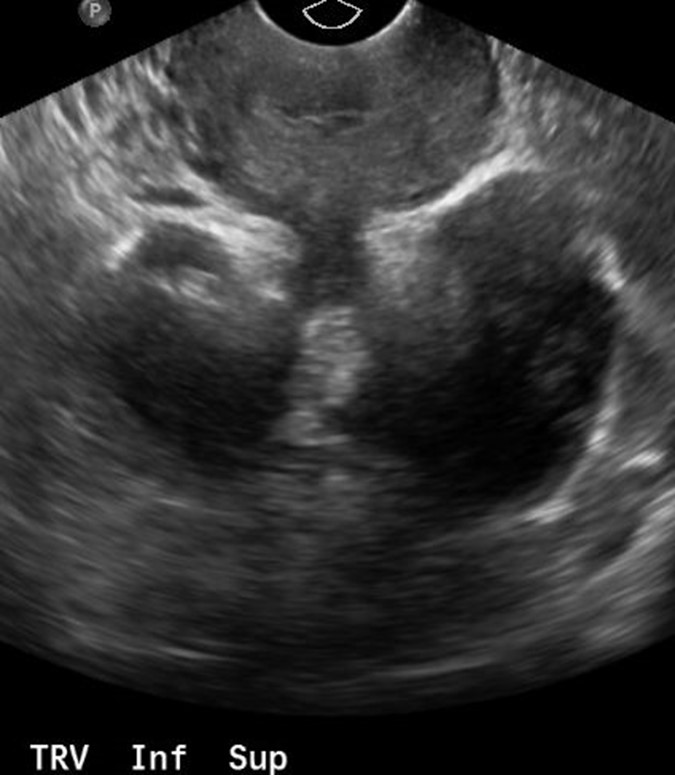
Delivered as a quartet of didactic summaries, alongside practical cases from each corresponding publication (Fig. 2), “A Sound Investment: SRU Consensus Statements, 2022–2024” will detail the recent high-quality recommendations from these consensus panels, all of which included practicing radiologists and clinical experts in relevant fields.
Fig. 2—Transverse view of lower uterus with adhesions of deep endometriosis (arrows) to both ovaries, resulting in “kissing ovaries” typical of deep endometriosis (courtesy of SRU)
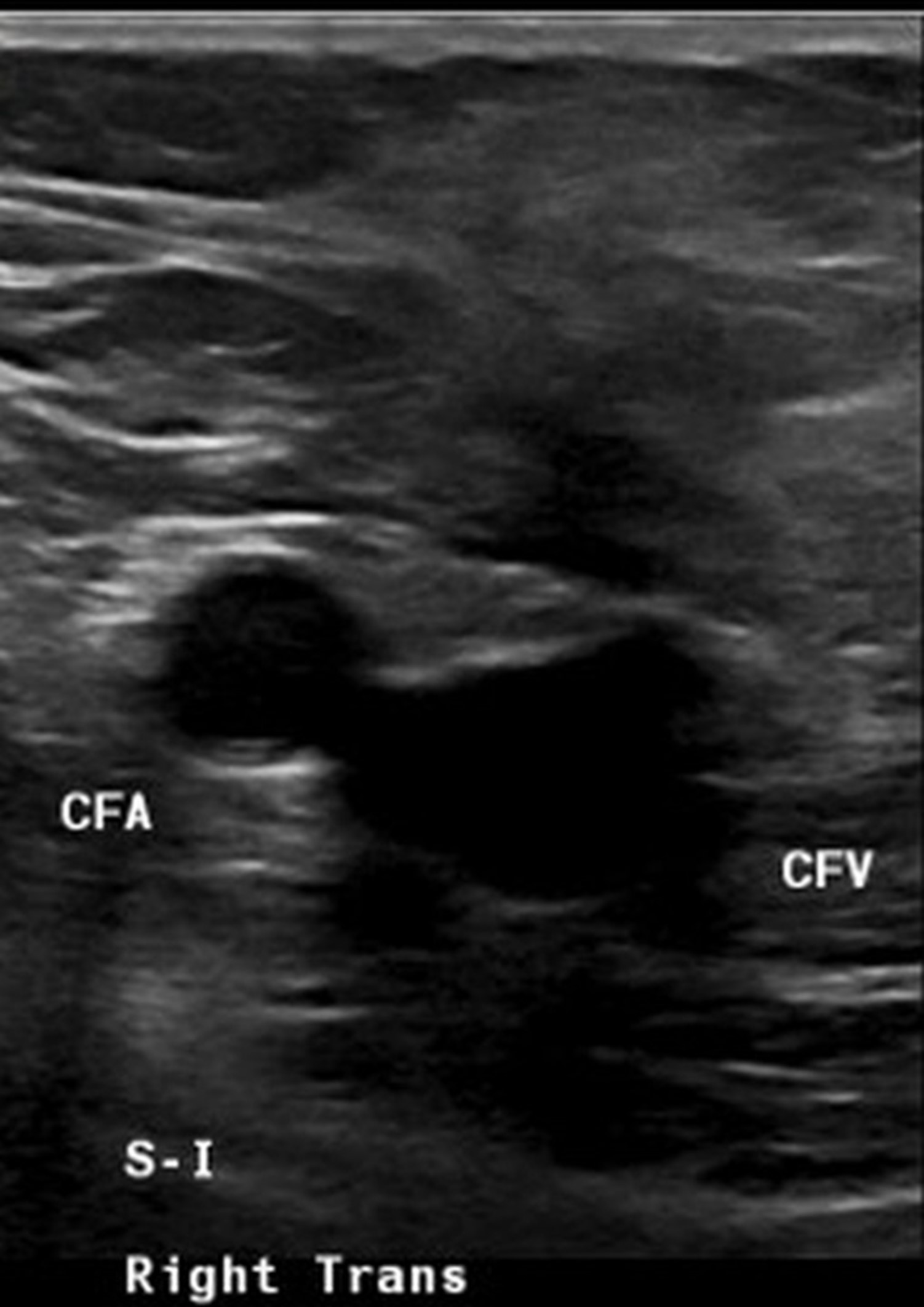
The expert moderators and lecturers for this ARRS Featured Session—all SRU fellows, as well as several past presidents of the society—will reinforce the modality’s most up-to-date nomenclature and guidelines (Fig. 3).
Fig. 3—Palpable “mass” (arrows) in right groin of patient with catheterization for cardiac ablation one month ago, corresponds to ill-defined, avascular region of increased echogenicity in subcutaneous fat, typical of fat necrosis (courtesy of SRU)
Specific “SRU Presents” lectures will focus on determining which gallbladder polyps do not require further imaging; how to describe and manage superficial soft-tissue masses; methods for augmenting routine pelvic ultrasound to detect endometriosis; and developing preferred terms and synonyms, as well as words to avoid, during first-trimester ultrasound.
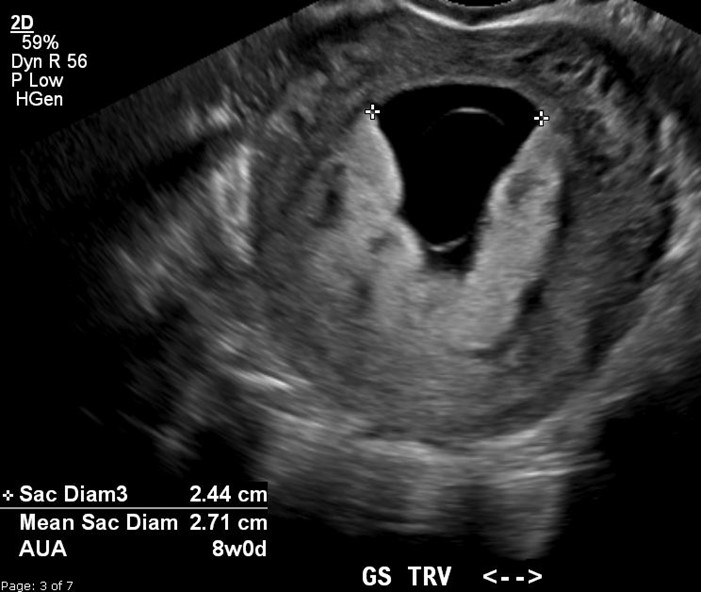
All 2025 ARRS Annual Meeting registrants, in-person attendees and virtual participants, will be shown illustrative examples and have the opportunity to ask questions of the lead authors of these SRU Consensus Statements (Fig. 4), expediting their incorporation into routine dictation templates.
Fig. 4—Example of definite early pregnancy loss (EPL) with intrauterine gestational sac with mean sac diameter of 27 mm and no visible embryo (courtesy of SRU)
AJR Finds Interreader Agreement on SRU Incidental Gallbladder Polyp Recommendations
Earlier this year in ARRS’ own American Journal of Roentgenology (AJR), 10 abdominal radiologists showed substantial agreement for gallbladder polyp risk categorizations and surgical consultation recommendations, although areas of reader variability were identified [5].
“The findings support overall reproducibility of the Society of Radiologists in Ultrasound (SRU) recommendations,” wrote Mark A. Anderson, MD, from the department of radiology at Massachusetts General Hospital in Boston. “Nonetheless, efforts should seek to further improve the consistency of polyp risk categorization by radiologists.”
Anderson et al.’s AJR accepted manuscript included 105 patients (median age, 52 years; 75 women, 27 men) with a gallbladder polyp on ultrasound—without features highly suspicious for invasive or malignant tumor—who underwent cholecystectomy (January 1, 2003–January 1, 2021). Ten abdominal radiologists independently reviewed ultrasound examinations and, using SRU recommendations, assessed one polyp per patient for risk category (extremely low, low, indeterminate) and possible recommendation for surgical consultation. Interreader agreement was evaluated between five radiologists with less than 5 years of experience and five more experienced (≥ 5 years) radiologists. Polyps were classified pathologically, either neoplastic or nonneoplastic.
Ultimately, among 10 abdominal radiologists applying the SRU’s recommendations from 2022, interreader agreement for risk category assignments was substantial among all readers (k = 0.710), less-experienced readers (k = 0.705), and more-experienced readers (k = 0.692). Interreader agreement for surgical consultation recommendations was substantial among all readers (k = 0.795) and more-experienced readers (k = 0.740), and almost perfect among less-experienced readers (k = 0.811).
References
Young SW, Jha P, Chamié L, et al. Society of Radiologists in Ultrasound Consensus on Routine Pelvic US for Endometriosis. Radiol 2024 Apr; 311:e232191. doi: 10.1148/radiol.232191
Jacobson JA, Middleton WD, Allison SJ, et al. Ultrasonography of Superficial Soft-Tissue Masses: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiol 2022 Jul; 304:18–30. doi: 10.1148/radiol.211101
Kamaya A, Fung C, Szpakowski JL, et al. Management of Incidentally Detected Gallbladder Polyps: Society of Radiologists in Ultrasound Consensus Conference Recommendations. Radiol 2022 Nov; 305:277–289. doi: 10.1148/radiol.213079
Doubilet PM, Benson CB, Bourne T, et al. Diagnostic Criteria for Nonviable Pregnancy Early in the First Trimester. Ultrasound Q 2014 Mar; 30:3–9. doi: 10.1097/RUQ.0000000000000060
Anderson MA, Mercaldo S, Cao J, et al. Society of Radiologists in Ultrasound Consensus Conference Recommendations for Incidental Gallbladder Polyp Management: Interreader Agreement Among 10 Radiologists. AJR 2024 May; 222:e2330720. doi: 10.2214/AJR.23.30720
In radiology, the new so often begets the novel. For imaging lung cancer, specifically, as innovative therapeutic options become more readily available, updated quantitative biomarkers are required to better buttress treatment selection, patient surveillance, and pharmaceutical development.
To be fair, Florian J. Fintelmann, MD, was already hard at work developing and validating imaging’s next generation of lung cancer biomarkers before becoming the 2019 ARRS Scholar. He just needed more time. Time to hone his understanding of critical oncological concepts in cohorts receiving mutation-specific therapies or immunotherapy. Time to investigate the relationship between CT body composition metrics, frailty, and cardiopulmonary function, while establishing reference values to support sarcopenia diagnosis. Time to define a leading role for chest CT beyond lesion detection, tumor staging, and surgical planning to patient-level prognostication.
Armed with a two-year, $90,000 grant from The Roentgen Fund®, as the assistant professor of radiology at Harvard Medical School and Massachusetts General Hospital staff radiologist explains, he got exactly what he wanted when he needed it the most.
InPractice: How has receiving The Roentgen Fund’s ARRS Scholarship informed your current research?
Florian J. Fintelmann, MD: My work as an ARRS Scholar has allowed me to dive deep into methodological questions, taking the time required to lay a solid foundation for many of the questions my Thoracic Imaging Percutaneous Thermal Ablation Team at Massachusetts General Hospital is addressing these days. The time afforded by this scholarship has allowed me to build up a multidisciplinary team, as well as apply for additional grant funding. The initial project that formed the basis for my ARRS Scholarship, “Advancing Lung Cancer Care With Imaging Biomarkers,” has morphed into multiple other projects. In addition, the Roentgen Fund’s provisioning of resources has since allowed me to develop a wide portfolio with three successful lines of research.
IP: And how has becoming an ARRS Scholar supported you, personally?
FJF: The Roentgen Fund’s support was instrumental in two distinct ways. Firstly, it enabled me to take classes at the Harvard School of Public Health. They have a wonderful summer course on clinical effectiveness, which allowed me to brush up on a lot of skills, learn several new ones, and connect with a very motivated community of budding researchers. Again, the other big aspect was protected time. Starting in 2019, I opted for the two-year model, meaning I had 50% of my time devoted to research during the duration of the scholarship. Of course, this ran right into the COVID-19 pandemic. So, while the world was being turned upside down, after initial trials and errors, I was able to claw back some of that protected time. Being an ARRS Scholar was a truly wonderful experience that allowed me to make significant inroads in terms of my own expertise and the team-building I do now with colleagues.
IP: Any advice for emerging researchers interested in applying for a Roentgen Fund fellowship?
FJF: My advice is simple: apply early. And if you’re not successful, apply again. In fact, I received my ARRS Scholarship on a second attempt. If you are at all interested in applying for any of the six Roentgen Fun scholarship programs, I strongly encourage you to do so because receiving one is a life-changing opportunity. It can take some practice, though. No one knows how to apply for a research or career award just by virtue of being a radiologist. Applying, and especially winning, are additional skills that you will need to learn to be successful. From writing up a plan to connecting with the right people, don’t be afraid to ask for help either.
IP: To whom did you look for help with your application, Dr. Fintelmann?
FJF: Particularly, I would like to shout out Dr. Anthony Samier, who was instrumental in helping me with the ARRS Scholarship application. Of course, my chair, Dr. Jim Brink, my division chief, Dr. Jo-Anne Shepard—the list goes on and on. There are a number of people who have made themselves available to help me move this forward. I appreciate everyone who supported me along the journey, and I want to say thank you to all those who believed I could do it.
IP: Since 1992, some 50 radiologists have been named ARRS Scholars. What’s it like knowing you, too, are on this list?
FJF: Becoming part of this legacy has been a critically important aspect of my research career. Looking back at so many prior scholars, and the community that’s been shaped by this shared experience, is really quite humbling. There are incredibly accomplished people on that list, some of whom I’ve had the pleasure of meeting or working with. Also, I think about those ARRS Scholars who will come after me. We’re all one big, happy family!