-
Findings correlate directly with increasing hydrostatic pressure—evolving from simple cardiac enlargement to life-threatening alveolar edema.
-
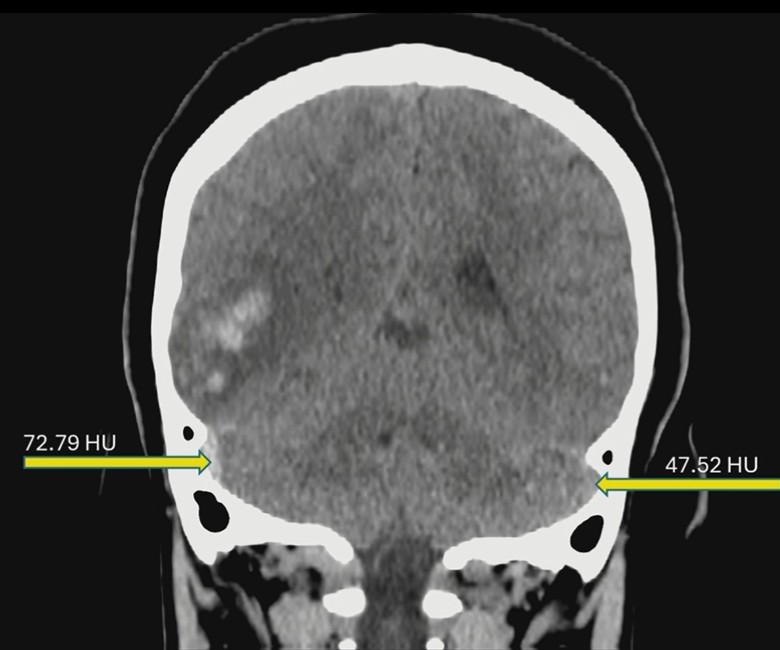
Rads often encounter normal non-contrast head CTs for headaches, but the real art lies in identifying dural venous sinus thrombosis (DVST) before that CTA is even ordered.
-
To ensure rads-in-training provide useful interpretations in real-world practice, residency programs must shift their emphasis to areas “above the diaphragm.”
-
PCCT offers a massive leap in spatial resolution for detecting submillimeter metastatic nodules in children. But it isn’t a free lunch either.
-
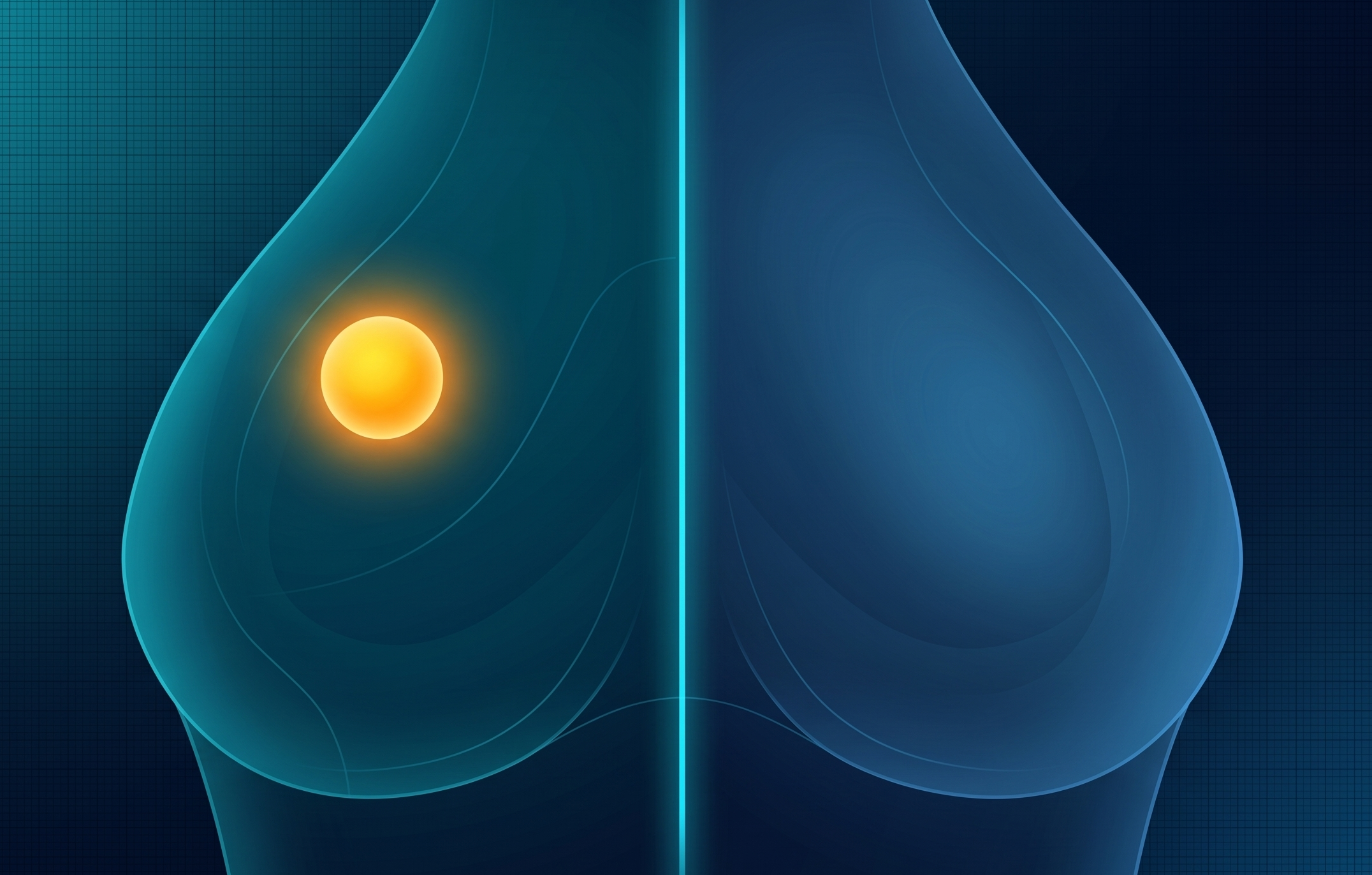
Molecular breast imaging continues to gain traction as an efficient supplemental screening tool, balancing clinical utility with ease of implementation for rads and patients alike.
-
While US is the primary screening tool, MRI should be utilized as a problem-solving resource when your US findings are inconclusive or complex.
-
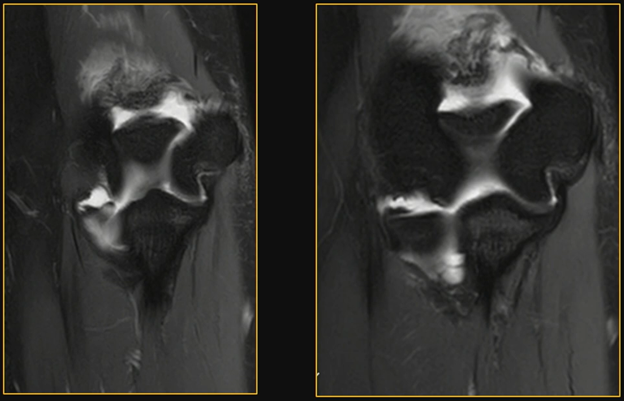
The most common manifestation is medial epicondyle apophysitis, an injury occurring during the acceleration phase of pitching when valgus stress creates significant medial traction.
-
When done correctly, legal consulting offers rads a significant path to income expansion, all the while providing a frontline look at how to protect their practices from, well, malpractice.

-
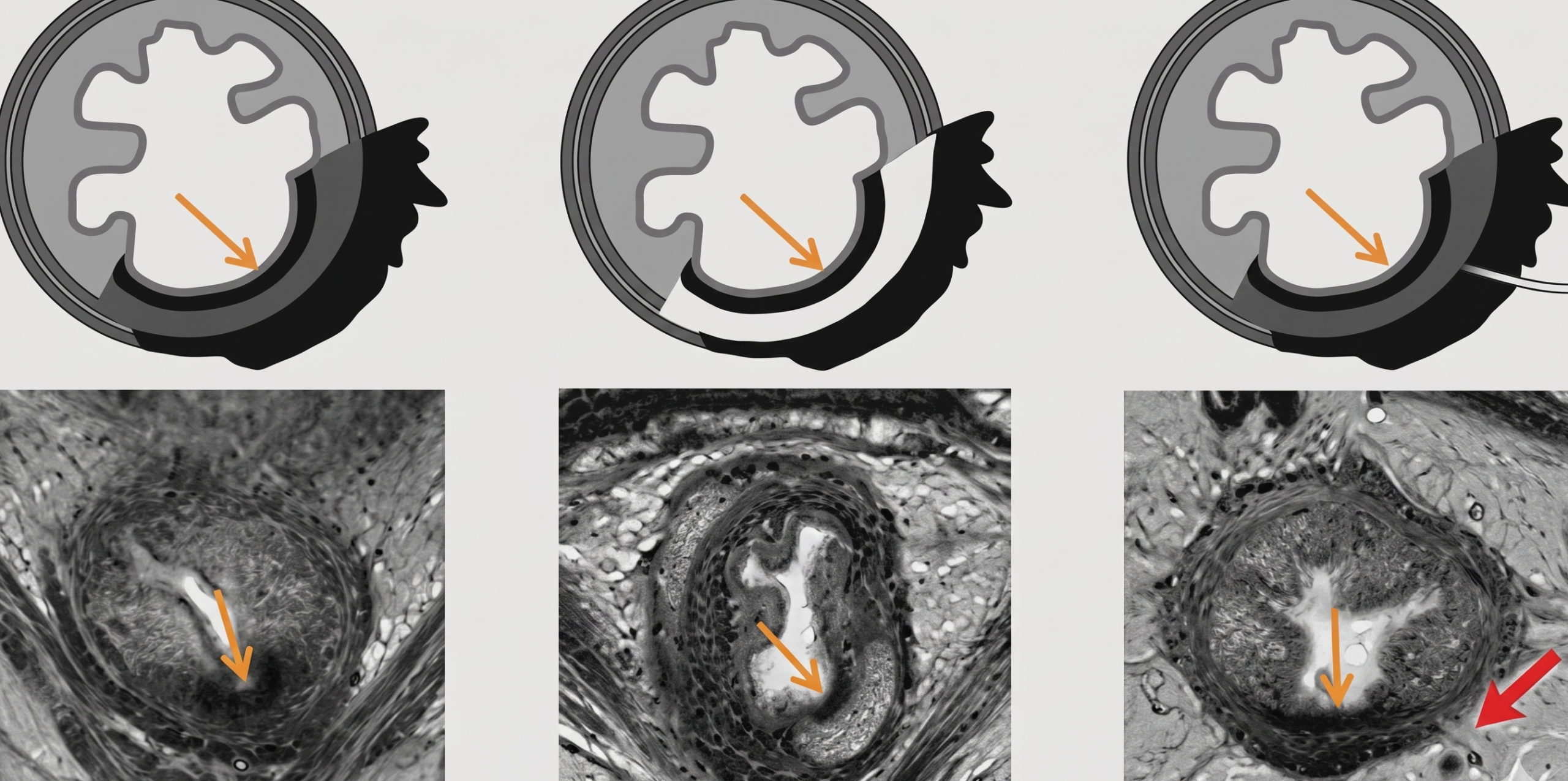
To determine if a split scar sign is positive, simply use the continuous line rule.
-
Many patients are managed primarily by medical oncologists—who may only trigger a referral to a rad onc if they see the specific term: oligometastatic.

