Associate Professor, Radiology Boston University Medical Center
Course Director 2023 ARRS Global Exchange Featuring Korean Society of Radiology (대한방사선학회)
The mission of ARRS’ Global Partner Society (GPS) program is to build long-standing relationships with key leaders and organizations in the worldwide imaging community—increasing awareness of our society’s services in specific nations, while raising the stature of Global Partner Societies among ARRS members. Every year, the ARRS Annual Meeting Global Exchange incorporates one partner society into the educational and social fabric of our meeting. ARRS members then reciprocate at the partner society’s meeting that same year.
The GPS partner to be featured at the 2023 ARRS Annual Meeting on the stunning island of Oahu in Honolulu, HI, will be our longtime colleagues from the Korean Society of Radiology (KSR). Established in 1945, KSR remains the official society representing all physicians of Korea working in the field of radiology. With a membership of more than 3,000 practicing imaging professionals—including 500 in-training members—KSR also publishes two scholarly journals: the Korean Journal of Radiology and Journal of the Korean Society of Radiology.
The 2023 ARRS Global Exchange Featuring KSR, “Changing Paradigms in Tumor Response Assessment,” will be the latest in a very long succession of successful educational partnerships between the Americans and Koreans. These two vaunted societies joined forces to present a GPS symposium on breast imaging back in 2017. For that fourth KSR/ARRS online collaboration, respective faculty curated 15 lectures across five breast imaging topics that were delivered during the 72nd Korean Congress of Radiology and the 2016 ARRS Annual Meeting in Los Angeles, CA [1].
On Sunday, April 16, live, virtually, and on-demand from Hawaii, the ARRS Annual Global Exchange Program will deliver a panel of experts from both the United States and Korea discussing a variety of topics and approaches regarding the quickly evolving role of radiologists in tumor response assessment. All participants, regardless of registration type, will gain functional familiarity with treatment response criteria across a wide swath of tumors, treatments, and techniques, learning from esteemed ARRS faculty from Brigham & Women’s Hospital, Memorial Sloan Kettering Cancer Center, and Rhode Island Hospital. I know I speak for the entire ARRS leadership and membership when I note how much we are all looking forward to hosting KSR’s leading experts from Seoul National University Hospital, Yonsei University Health System, Soonchunhyang University College of Medicine, and the Catholic University of Korea. Our Korean friends will help us understand locoregional treatment response evaluation for hepatocellular carcinoma (HCC).
Immune Checkpoints: No Inhibitions?
Be it in America, across the Pacific, or anywhere else in the world for that matter, a chief radiological concern moving forward is recognizing the spectrum of responses and progressive diseases typically encountered in patients treated with immunotherapies, especially immune checkpoint inhibitors (ICI). Right now, indications for ICI therapy already include more than 16 different cancers. As this number will only continue to increase in the coming years, academic and private practice imagers (in addition to radiology residents and fellows) need to know the hang-ups of ICIs.
Recently, on the AJR Podcast episode “Chest CT Findings of Immune Checkpoint Inhibitor Therapy-Related Adverse Events,” Kerem Ozturk, MD, discussed why awareness of early chest CT findings is required for early detection and accurate diagnosis of ICI therapy-related adverse events [2]. Said events are myriad, including pneumonitis, new consolidation, worsening thoracic tumor burden, pleural/pericardial effusion, and pulmonary emboli in the emergency department.
We need to know about combinations, too. Promising results have been published in KSR’s own Korean Journal of Radiology regarding ICI combination therapy and ICI combined with radiotherapy. Specifically, as Kim et al. pointed out in their systematic review and meta-analysis, ICI combination therapy or ICI combined with radiotherapy can work wonders, showing better localized efficacy than ICI monotherapy for treating melanoma brain metastasis [3]. Inevitably, the ever-increasing adoption of ICIs will lead to more and more practical applications.
HCC: Mimics and Machine Learning
Due to its distinct imaging, HCC can be diagnosed noninvasively, typically via multiphasic CT and MRI. As Yoon et al. reminded us in their survey and pictorial review for the Journal of the Korean Society of Radiology, while imaging features like arterial phase hyperenhancement and washout on portal or delayed phase images is classic for HCC, the ability to distinguish HCC-mimicking lesions (e.g., arterioportal shunts, combined HCC-cholangiocarcinoma, intrahepatic cholangiocarcinoma, hemangioma, etc.) on initial imaging examinations is critical for management and treatment alike [4].
Radiologists of tomorrow will need to recognize more than just mimics. We must become familiar with multiple machine learning models, as applied to presently underutilized imaging features that could help construct more reliable criteria for organ allocation and liver transplant eligibility. Apropos, recent findings suggest that machine learning-based models can predict recurrence before therapy allocation in patients with early-stage HCC initially eligible for liver transplant.
As described in AJR OnTrend, 120 patients diagnosed with early-stage HCC, who were initially eligible for liver transplant and underwent treatment by transplant, resection, or thermal ablation, underwent pretreatment MRI and post-treatment imaging surveillance. Imaging features were extracted from postcontrast phases of pretreatment MRI examinations using a pretrained convolutional neural network. Pretreatment clinical characteristics (including labs) and extracted imaging features were integrated for recurrence prediction to develop three ML models: clinical, imaging, combined. Ultimately, all three models predicted posttreatment recurrence for early-stage HCC from pretreatment clinical, MRI, and both data combined [5].
Paradigm and Response Changes
Fortunately, the many recent advances in oncologic patient care are allowing physicians to move beyond nonselective cytotoxic therapies. Increasingly, our specialty will come to rely upon more targeted and personalized treatments for cancer: immunotherapies, stereotactic radiation, image-guided interventions, and theranostics. Alongside these novel approaches to cancer treatment, all houses of radiology will need to prop the door open for our specialty to evolve beyond tumor size measurement—recognizing the cumulative variability in the appearance of treatment responses and associated treatment toxicities by CT, MRI, PET, and a host of hybrid imaging. Given the proliferation of still evolving precision treatment pathways, abdominal, gastrointestinal, and genitourinary subspecialists must stay vigilant and informed. “Changing Paradigms in Tumor Response Assessment” aims to provide precisely that—a contemporary, rigorous update regarding the changing appearances of tumor response on multiple modalities and across a wide spectrum of tumors. I cordially invite you to join Jin-Young Choi, Joon-Il Choi, Natally Horvat, Katherine Krajewski, Jeong Min Lee, Sanghyeok Lim, Don Yoo, and me for the 2023 ARRS Global Exchange Featuring Korean Society of Radiology (대한방사선학회).
Kim PH et al. Immune checkpoint inhibitor with or without radiotherapy in melanoma patients with brain metastases: a systematic review and meta-Analysis. J Korean Soc Radiol 2022; 83:808–829
Yoon J et al. Atypical manifestation of primary hepatocellular carcinoma and hepatic malignancy mimicking lesions. Korean J Radiol 2021; 22:584–595
On Friday, December 9, the final ARRS Virtual Symposium for 2022, Update on Breast Imaging and Multimodality Biopsy, will address timely topics, including digital breast tomosynthesis (DBT), breast ultrasound (US), breast MRI, molecular breast imaging (MBI), and contrast-enhanced mammography (CEM). Didactic lectures will emphasize the most appropriate biopsy methods and procedures for every one of these aforementioned breast imaging modalities—allowing multiple opportunities for radiologists to improve patient outcomes, using current technologies available for early detection of breast cancer.
Digital Breast Tomosynthesis
I will begin the presentation at noon, Eastern Time, on December 9. Focusing on clinical implementation of DBT, I will review DBT technology and important factors to consider for practical application, such as improved breast cancer detection, synthetic digital mammography, and workflow for screening and diagnostic populations.
Recognizing the need for DBT-guided breast biopsy, Sarah M. Friedewald, MD, of Northwestern University will present on advantages and disadvantages of prone and upright biopsy systems, as well as interpretive outcomes for biopsy-proven, DBT-only findings. Earlier this summer in AJR [1], Dr. Friedewald coauthored the first study of its kind comparing pathologic outcomes between patients with single and multiple architectural distortion visualized by DBT. Ultimately, for those patients with multiple architectural distortions identified on DBT, biopsy of all areas may be warranted, given the variation of pathologic diagnoses.
Breast Ultrasound
Liane Philpotts, MD, of the Yale School of Medicine will describe how to optimize breast US in symptomatic patients, pointing out tools to enhance correlations between sonographic, mammographic, and DBT findings. Additionally, Dr. Philpotts will describe methods for reducing false positives (false negatives, too). Meanwhile, 2004 ARRS Scholar Jessica W. T. Leung, MD, of MD Anderson Cancer Center [2] will help us define the clinical indications, benefits, and limitations of US-guided procedures of the breast, while assessing the post-biopsy imaging/pathologic concordance.
Breast MRI
As recent clinical perspectives have affirmed [3], MRI remains the most sensitive tool for detecting breast cancer; however, cost and acquisition time continue to be deterrents in adopting the technology for routine screening purposes. Following our first question and answer session of the afternoon, fellow InPractice breast imaging contributor [4] Linda Moy, MD, of NYU Langone Health will discuss the present role of screening breast MRI, alongside the roles that AI is poised to play in the very near future. Dr. Moy will also bring everyone up to speed on abbreviated or “ultrafast” MRI protocols for supplemental screening [5]. For her session, Laurie R. Margolies, MD, of Mount Sinai will detail the equipment and techniques required to perform MRI-guided breast biopsy procedures, pointing out both pearls and pitfalls to improve the overall patient experience.
Molecular Breast Imaging and Contrast-Enhanced Mammography
Increasingly, MBI continues its integration into routine breast imaging practice. Haydee Ojeda-Fournier, MD, from University of California San Diego Health will present on this topic, describing the variety of MBI indications for use in clinical practice. Her lecture will incorporate discussions of the MBI lexicon, which is well-timed given that, as AJR acknowledged in July [6], we shouldn’t have to wait too much longer for the American College of Radiology’s BI-RADS committee to initiate its own incorporation of MBI lexicon into the BI-RADS Atlas. Finally, Janice S. Sung, MD, of Memorial Sloan Kettering Cancer Center will deliver a must-see session regarding a relatively new breast imaging modality that is quickly gaining acceptance: CEM [7]. CEM renders density and morphologic information on low-energy images in conjunction with physiologic enhancement via the recombined (i.e., subtracted and processed) images. CEM-guided biopsy is not only FDA-approved, as noted in the most recent issue of InPractice [8], it is frequently necessary for proper patient management. Dr. Sung will detail real-world considerations for setting up a CEM program at your institution and practice, followed by another high-impact question and answer session with the entire faculty.
The experts above continue to enjoy an extensive range of clinical experience with each breast imaging modality presently impacting patient care, so I urge diagnostic radiologists, full-time, or even part-time breast imagers—academic and private practice alike—to join us for Update on Breast Imaging and Multimodality Biopsy on the 9th of December. Offering 4 CME credit hours for ARRS members, the entire program will remain available on demand for practicing radiologists, as well as fellows, residents, and allied medical students, who are unable to attend our live event.
References
Wang LC, Philip M, Bhole S, et al. Pathologic outcomes in single versus multiple areas of architectural distortion on digital breast tomosynthesis. AJR 2022; 1–13:10.2214/AJR.22.27625
Mango VL, Grimm LJ, Harvey JA, Plecha DM, Conant EF. Abbreviated Breast MRI for Supplemental Screening: The Why and How of Clinical Implementation. ARRS InPractice site. www.radfyi.org/abbreviated-breast-mri-supplemental-screening. Published May 13, 2022. Accessed October 29, 2022
Hunt KN, Conners AL, Samreen N, Rhodes DJ, Johnson MP, Hruska CB. PPV of the molecular breast imaging lexicon. AJR 2022; 1–9:10.2214/AJR.21.27047
Division of Musculoskeletal Imaging and Intervention Department of Radiology Massachusetts General Hospital
Joao R.T. Vicentini, MD
Division of Musculoskeletal Imaging and Intervention Department of Radiology Massachusetts General Hospital
Connie Y. Chang, MD
Division of Musculoskeletal Imaging and Intervention Department of Radiology Massachusetts General Hospital
The ankle and foot are challenging areas to image and diagnose, due to complex anatomy. In advance of the 2023 ARRS Annual Meeting Categorical Course, “Pitfalls and Challenging Cases: How to Triumph and Make the Diagnosis,” our InPractice article is a collection of cases that we hope will help you conquer some of these pathologies.
Nearly all ankle and midfoot cases begin with radiographs, because radiography is the modality we usually encounter initially, and x-rays can often give us many clues about the diagnosis, especially in the ankle. In the midfoot, which has more complicated anatomy, cross-sectional imaging, especially MRI, is often required to make the diagnosis.
Case No. 1
For the classic inversion injury or ankle “sprain,” we typically think of lateral ankle ligament injuries, or a fibular avulsion fracture. Since the foot and ankle are relatively flexible, injuries can occur in many places. Our first case is a 27-year-old man who injured his ankle in a rollover car accident. In the lateral aspect of the talar dome—left image above—there is a curvilinear subchondral lucency (dotted curve) seen on the frontal radiographic view, compatible with an osteochondral lesion (arrow).
Osteochondral lesions (OCL) of the talus can be quite difficult to see on x-rays, and OCLs are often missed, especially when they occur with other bony injuries. For example, a patient may have a fibular fracture, which is adequately treated, and then experience persistent pain later on [1]. If the mechanism of injury involves shearing (e.g., tibiotalar subluxation), compression (e.g., falling from a height) or avulsion (e.g., distraction of the tibiotalar joint), the index of suspicion for an osteochondral injury should be higher, although these details may be difficult to ascertain from the patient or the medical record [2]. Impaction of the talus on the distal tibial plafond leads to microfractures in the cartilage and subchondral bone plate, and the increased pressure from weight-bearing can cause osteonecrosis [3]. This process can take a variable amount of time; therefore, presentation may be delayed up to 6–12 months. Even if the OCL is seen on radiographs, cross-sectional imaging is frequently needed. CT may be more helpful to evaluate small or comminuted OCLs, as ossific fragments may be difficult to visualize on MRI [4]. Apropos, the coronal reconstruction CT image of this case—right image above—demonstrates the mildly displaced, dominant osteochondral fragment (solid arrow). There is an additional punctate ossific fragment (dashed arrow) along the lateral aspect of the osteochondral injury, not seen on the x-ray. It would be unlikely to see this fragment on MRI, simply because of the inadequate spatial resolution.
Case No. 2
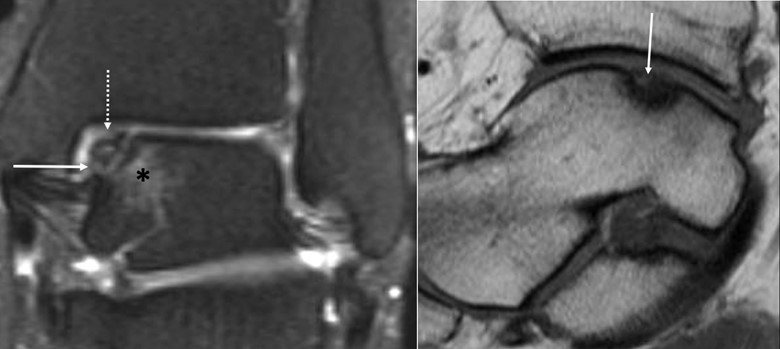
When an ossific fragment is not displaced, as in this case of a 39-year-old who twisted her ankle on the stairs 6 months ago, MRI can be helpful to evaluate for stability. On the coronal T2 fat-suppressed image—left image above—we can see that the fragment is somewhat irregular at the articular surface, but there is fluid signal intensity completely undercutting the fragment (solid arrow), and bone marrow edema in the adjacent talus, suggesting that the fragment is unstable [5]. There is mild subchondral bony irregularity and depression (dashed arrow), too. Other signs of instability may be cystic change or partial or complete separation of the fragment from the donor site [8].
The sagittal T1 image—right image above—shows that a large portion of the fragment is low in signal intensity, which persists on all sequences, and there is articular surface collapse, suggesting that the portion is at least partially osteonecrotic [8]. Another portion still demonstrates fat signal intensity (solid arrow) on T1 and high signal on the T2 fat-suppressed image, suggesting that tis portion remains viable.
This patient was placed on a trial of conservative treatment, including a lace-up ankle brace and semi-rigid orthosis, which had just begun at the time of writing this article. Management depends on patient symptoms, as well as size and stability of the OCL. In general, small (< 15mm2), stable fragments in ankle fractures are treated conservatively, whereas large, unstable fragments are managed operatively [3, 6–7, 9]. Surgical options include arthroscopic drilling, excision and debridement, or osteocartilaginous grafting [2].
Case No. 3
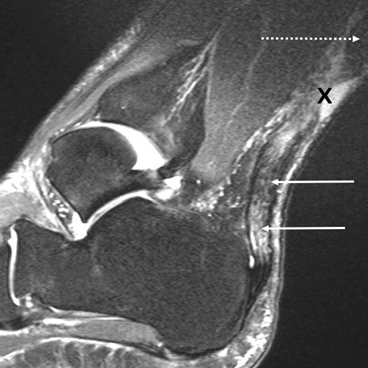
Our third and final case is a 33-year-old woman, playing tennis two hours prior to presentation, who had planted her foot, tried to run forward, then felt something like “a hit behind her ankle.” The patient could no longer walk without significant pain. The initial radiograph demonstrates distal Achilles thickening, and more proximally, a focally irregular anterior margin, consistent with Achilles tendinopathy and tear. Achilles tendon ruptures account for 20% of all large tendon ruptures [10]. Showing bimodal age distribution, the first peak occurs around the third to the fifth decade of life, due to high-energy injuries, while the second peak occurs in the elderly, due to low-energy injuries to a degenerated tendon. Men are more commonly affected. Achilles tears are more common in sports with forceful and repetitive jumping or “push-off,” often seen in cyclists, gymnasts, runners, and divers, as well as tennis, basketball, and volleyball players. Risk factors include poor conditioning before exercise, prolonged use of corticosteroids, fluoroquinolone antibiotics, and overexertion [11].
Because the Achilles tendon is bound by the Kager fat pad anteriorly and subcutaneous fat posteriorly, an abnormal appearance can often be detected on radiographs [12]. The lateral radiograph—left image above—demonstrates diffuse fusiform thickening of the Achilles tendon (dashed arrow). More proximally, the tendon is irregular anteriorly, consistent with a tear. There is edema in the Kager fat pad (“K”), also indicating acute tear. It can be difficult to determine partial versus full-thickness tear, and in this case, the posterior margin of the tendon appears intact, suggesting that it is a high-grade partial, rather than full-thickness tear, although MRI later confirmed that it was a full-thickness tear. Ossific foci, if present, suggest chronic tears (not seen in this case) [13].
On MRI, we first observe that the foot was placed in plantar flexion, which may underestimate the tendon gap. While this typically does not preclude diagnosis of the tendon tear, it inevitably brings torn pieces of tendon closer together, and the maximum tendon gap cannot be determined.
The sagittal T2 fat-suppressed image—right image above—demonstrates a full-thickness tear (“X”) and severely degenerated proximal (dashed arrow) and distal (solid arrows) tendon. The uniformly thickened and hyperintense distal tendon is probably a combination of chronic tendon degeneration and acute edema from the tear, especially as individual fibers within the tendon are relatively well seen. It is important to comment on tendon quality and the length of tendon, which appears severely degenerated, because this tendon may not be useable for repair [14]. Many of the internal strands appear wavy, compatible with retraction. MRI is considered the gold standard for imaging Achilles tendon tears (sensitivity, 80–100%; specificity, 100%) (8, 15). Ultrasound also has high sensitivity (full thickness, 95%; partial thickness, 94%) and specificity (full thickness, 99%; partial thickness, 97%) for the detection of Achilles tendon tears, given the tendon’s superficial location and possibility of dynamic imaging with the modality (16, 17). This patient’s tear was also well seen on ultrasound (not shown).
Since the patient was only visiting the United States, she was placed in a boot for her trip home, although surgical intervention was required soon after arriving. Management of Achilles tendon ruptures is controversial and evolving. Overall, there has been a general trend moving toward immobilization with functional rehabilitation, rather than treating all ruptures exclusively with surgical repair [18, 19].
Focusing on interpretative skills for avoiding misdiagnoses across a wide spectrum of musculoskeletal imaging pitfalls, the 2023 ARRS Annual Meeting Categorical Course, “Pitfalls and Challenging Cases: How to Triumph and Make the Diagnosis,” will also tackle challenging cases within neuroradiology, abdominal, and chest imaging. Topics will emphasize real-life clinical scenarios, while providing tips and tricks for optimal performance. We invite you to join us on the beautiful island of Oahu in Honolulu, HI (or virtually or even on demand) for this exciting, 18-hour Categorical Course, purposefully designed to enhance your ability to add value to patient management.
References
StatPearls Publishing; www.ncbi.nlm.nih.gov/books/NBK556139. Cited Accessed Aug 18 2022
Badekas T, Takvorian M, Souras N. Treatment principles for osteochondral lesions in foot and ankle. Int Orthop 2013; 37:1697–706
Rikken QGH, Kerkhoffs GMMJ. Osteochondral lesions of the talus: an individualized treatment paradigm from the Amsterdam perspective. Foot Ankle Clin 2021; 26:121–36
Yasui Y, Hannon CP, Fraser EJ, et al. Lesion size measured on MRI does not accurately reflect arthroscopic measurement in talar osteochondral lesions. Orthop J Sports Med 2019; 7:2325967118825261
Rios AM, Rosenberg ZS, Bencardino JT, Perez Rodrigo S, Garcia Theran S. Bone marrow edema patterns in the ankle and hindfoot: distinguishing MRI features. AJR 2011; 197:720–729
Pedersen ME, DaCambra MP, Jibri Z, Dhillon S, Jen H, Jomha NM. Acute osteochondral fractures in the lower extremities–approach to identification and treatment. Open Orthop J 2015; 9:463–474
Gianakos AL, Yasui Y, Hannon CP, Kennedy JG. Current management of talar osteochondral lesions. World J Orthop 2017; 8:12–20
Szaro P, Geijer M, Solidakis N. Traumatic and non-traumatic bone marrow edema in ankle MRI: a pictorial essay. Insights Imaging 2020; 11:97
van Dijk CN, Reilingh ML, Zengerink M, van Bergen CJA. Osteochondral defects in the ankle: why painful? Knee Surg Sports Traumatol Arthrosc 2010; 18:570–580
Shamrock AG, Varacallo M. Achilles tendon rupture. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; www.ncbi.nlm.nih.gov/books/NBK430844. Cited Accessed Aug 18 2022
Theobald P, Bydder G, Dent C, Nokes L, Pugh N, Benjamin M. The functional anatomy of Kager’s fat pad in relation to retrocalcaneal problems and other hindfoot disorders. J Ana 2006; 208:91
Paoloni J. Tendon injuries–practice tips for GPs. Aust Fam Physician 2013; 42:176–180
Bäcker HC, Wong TT, Vosseller JT. MRI assessment of degeneration of the tendon in Achilles tendon ruptures. Foot Ankle Int 2019; 40:895–899
Dams OC, Reininga IHF, Gielen JL, van den Akker-Scheek I, Zwerver J. Imaging modalities in the diagnosis and monitoring of Achilles tendon ruptures: a systematic review. Injury 2017; 48:2383–2399
Chang A, Miller TT. Imaging of tendons. Sports Health 2009; 1:293–300
Aminlari A, Stone J, McKee R, et al. Diagnosing Achilles tendon rupture with ultrasound in patients treated surgically: a systematic review and meta-analysis. J Emerg Med 2021; 61:558–567
Park SH, Lee HS, Young KW, Seo SG. Treatment of acute Achilles tendon rupture. Clin Orthop Surg 2020; 12:1–8
Deng S, Sun Z, Zhang C, Chen G, Li J. Surgical treatment versus conservative management for acute Achilles tendon rupture: a systematic review and meta-analysis of randomized controlled trials. J Foot Ankle Surg 2017; 56:1236–1243
Since its introduction nearly 20 years ago, score-based peer review has not been shown to have a meaningful impact on or be an accurate measurement of radiologist performance [1]. A new paradigm—peer learning—has emerged, which is a group activity where practicing professionals review each other’s work, actively give and receive feedback in a constructive manner, teach and learn from one another, and mutually commit to improving performance as individuals and as a group. As my colleague, coauthor, and present chair of ARRS’ Professional & Performance Improvement Committee, Nadja Kadom, MD, first noted here in the pages of InPractice back in 2019, peer learning is “a system that uses accuracy of interpretation as a surrogate marker for competency” [2].
Many radiology practices are beginning to transition from score-based peer review to peer learning, but these same practices face distinct challenges and multiple barriers to implementation, especially considering the variety of leadership styles Dr. Kadom has recently detailed [3]. Case in point: nearly half of the 742 members of ARRS who participated in our 2020 AJR Original Research article, “Current Status and Future Wish List of Peer Review: A National Questionnaire of U.S. Radiologists,” reported insufficient learning outcomes from peer review [4]. Clarifying a minimum number of cases that required monthly review, as well as how interpretive discrepancies would be communicated, were two big factors where some level of standardization was clearly needed.
Perhaps most importantly, the demographics of our survey respondents reflected the current composition of this country’s imaging workforce. A total 742 (4.2% response rate) ARRS members replied to our 21-question, multiple-choice questionnaire. Among those respondents, 547 (73.7%) were board-certified, practicing radiologists also participating in a form of peer review. As you can see, most responders were in private practice (51.7%, 283/547), while the next largest cohort was in academic practice (32.4%). The most common practice size was 11–50 radiologists (50.5%), followed by groups of up to 10 radiologists (21.2%). The majority of responders practiced in urban settings (61.6%), too.
Practice Characteristic
No. (%)
Type
Private
283 (51.7)
Academica
177 (32.4)
Hybridb
45 (8.2)
Government
42 (7.7)
No. of radiologists
0–10
116 (21.2)
11–50
276 (50.5)
51–100
85 (15.5)
>100
70 (12.8)
Setting
Urban
337 (61.6)
Suburban
158 (28.9)
Rural
52 (9.5)
aAcademic practices had medical school and radiology residency program. bHybrid practices had radiology residency program without a medical school.
Nonetheless, in this largest nationwide questionnaire to imaging professionals regarding the present state of and their future needs for peer review, most radiologists working in the United States felt a better system is not only necessary, but that said system could even be feasible in daily practice.
To our knowledge, “Updates for Your Peer Learning Activities: Pitfalls, Tips, and Accreditations” remains the only course of its kind. Presented live as a Featured Sunday Session during the 2023 ARRS Annual Meeting in Honolulu, HI, this course is now in its second revised and expanded iteration, packed with practical tips to clinical success, all taught by experts in the field. Summarizing the current status and practice gap in peer review in radiology, sessions will include three didactic lectures to showcase the best practices and challenges of peer learning programs at multiple institutions, including Emory, NYU, Stanford and Mayo Clinic. Esteemed faculty will highlight potential barriers to starting and sustaining peer learning activities in both academic and private practice settings, each instructor sharing their own “top 5 tips” for overcome these challenges. We will also address the latest updates from the American College of Radiology’s Quality and Safety Commission regarding new accreditation pathways for peer learning [5].
The evolution of peer learning is of universal importance for the continuing education of all radiologists—in practice, during fellowship or residency. However, the intersecting concepts of peer learning, just culture, etc. are evolving at a breakneck pace, with brand-new accreditation pathways opening up and multiple acceptable approaches to finding the “right answer” [6]. For imaging professionals already involved in peer learning, come share your experience with our expert panel, ensuring you are getting the most out of your program. For those new to peer learning, come learn how to fish for the pearls, avoid the pitfalls, and hit the ground running. We will conclude with an interactive panel discussion with the audience—there in Hawaii, virtually, or on demand.
References
Larson DB et al. Transitioning from peer review to peer learning: report of the 2020 Peer Learning Summit. J Am Coll Radiol 2020; 17:1499–1508
@OWeaverMD Department of Breast Imaging, Division of Diagnostic Imaging MD Anderson Cancer Center
Contrast-enhanced mammography (CEM) is a relatively new modality which is rapidly gaining acceptance in breast imaging. Many medical centers have already acquired the necessary equipment to implement CEM programs [1], thus creating an ever-increasing demand for trusted CEM educational resources.
At the same time, however, there remains a paucity of quality instructional materials for this emerging tool, a lack of structured, case-based training, and fundamental misconceptions regarding both the technical aspects and the operational/administrative knowledge needed for successful implementation of CEM.
On day one of the 2023 ARRS Annual Meeting, Sunday, April 16, live (and virtually, of course) from Honolulu on the enchanting island of Oahu, HI, Drs. Wendie Berg, Bhavika Patel, and I, will offer a two-hour introductory program on practical CEM for radiologists. Our Featured Sunday Session, “Contrast-Enhanced Mammography: The Essentials and Beyond,” will include interactive didactic and case-based lectures to educate and update practicing radiologists on the important foundational principles of CEM. The course will be supplemented with an optional short pre- and post-test survey to help the audience organize the information and evaluate their learning progress.
CEM Augments Mammography Capabilities in the Digital Era
The strength of CEM is its ability to provide both morphologic information on low-energy images, similar to a standard 2D mammogram, and functional information of contrast distribution on the “recombined” (subtracted and processed) images. This is achieved by software and hardware modifications to modern mammographic equipment and necessitates patient workflow adjustments in breast centers [2]. The course will present the basics of CEM technology, its strengths and limitations, as well as helpful tips on implementing this modality in clinical practice.
Additionally, the course will serve as a guide to CEM image interpretation with a special emphasis on utilization of the newly introduced Breast Imaging Reporting & Data System (BI-RADS®) CEM lexicon [3].
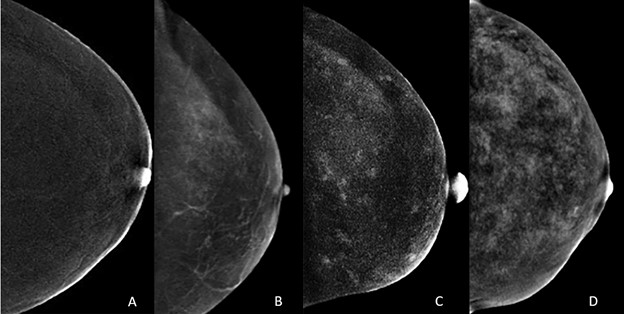
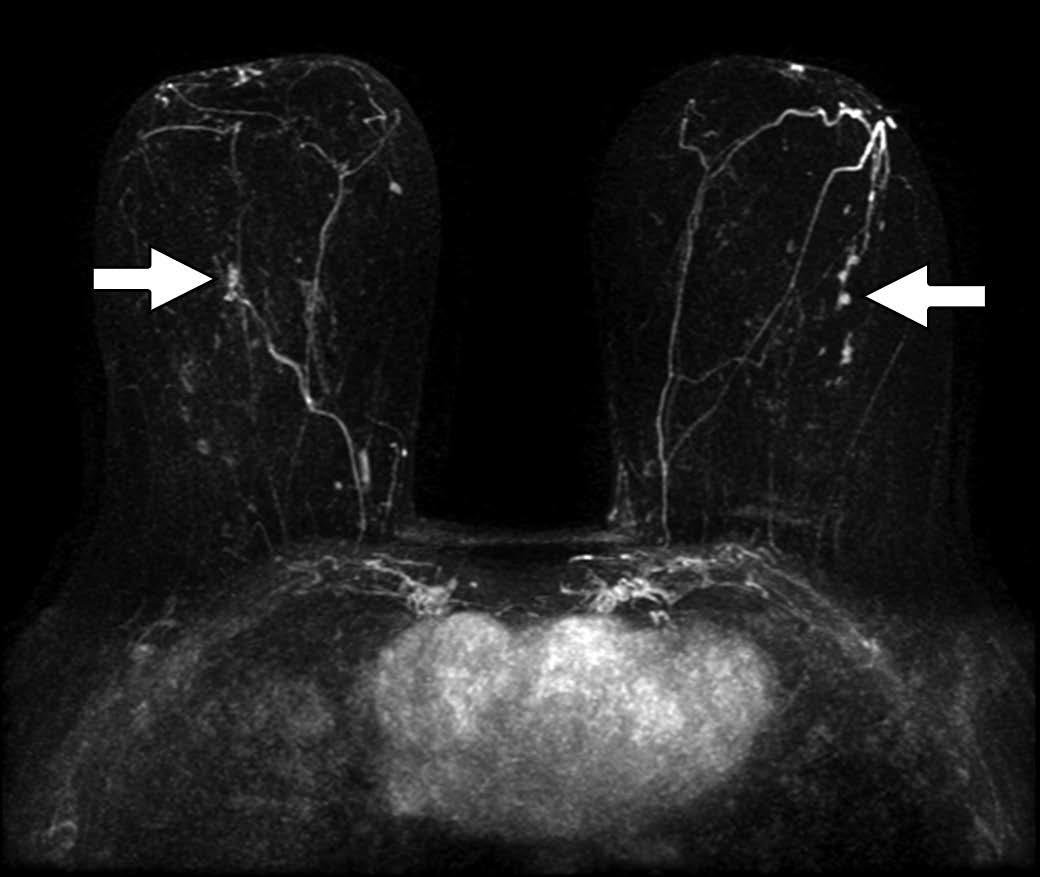
We will also discuss background parenchymal enhancement (BPE) in CEM image interpretation. Similar to breast tissue density of mammography, increased BPE may both mask and mimic cancer on CEM. As on MRI, there are four categories of BPE (Fig. 1), and multiple factors are associated with increased BPE [4]. We will present the audience with a range of appearances for normal BPE on CEM.
Fig. 1—Normal craniocaudal views of recombined images from CEM examination of four patients show different patterns of BPE: minimal (A), mild (B), moderate (C), and marked (D). All enhancement on images caused by normal BPE [4].
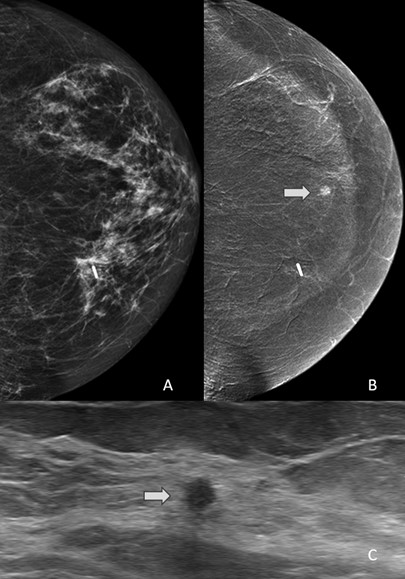
Drs. Berg, Patel, and myself will provide a case-based introduction to the most common artifacts and cancer mimics on CEM, too. This topic is continuously evolving. In the July issue of AJR, enhancing cherry hemangioma has been described as a common benign finding that may be misleading (Fig. 2) [5]. It is helpful for the technologist to make note of skin lesions, which can be marked to facilitate recognition.
Fig. 2—52-year-old woman with dense breasts and family history of breast cancer (estimated lifetime risk, 20.4% by Tyrer-Cuzick model version 8) undergoing high-risk screening CEM. 1A: Right craniocaudal (left) and mediolateral oblique (right) CEM obtained 2.5 minutes after IV injection of 125 mL of iopamidol (Isovue 370, Bracco) show superficial 3-mm focus (circle) with medium enhancement in superior aspect of breast approximately 5 cm from nipple. 1B: Clinical photograph shows 3-mm cherry hemangioma (circle) on skin of right breast at 10-o’clock position approximately 5 cm from nipple found clinically by radiologist performing ultrasound. Finding corresponds to enhancing focus in A [5].
CEM Screening and Diagnostic Applications
Chief among the topics discussed will be the role of CEM, alongside other legacy modalities, in today’s screening and diagnostic guidelines and society-endorsed consensus recommendations for breast cancer imaging. CEM is already recommended as an alternative to MRI in screening of women at high risk of breast cancer and in average-risk women with dense breasts [6]. An AJR article from 2021 demonstrated that CEM shows promise as a breast cancer screening examination in patients with a personal history of lobular neoplasia [7].
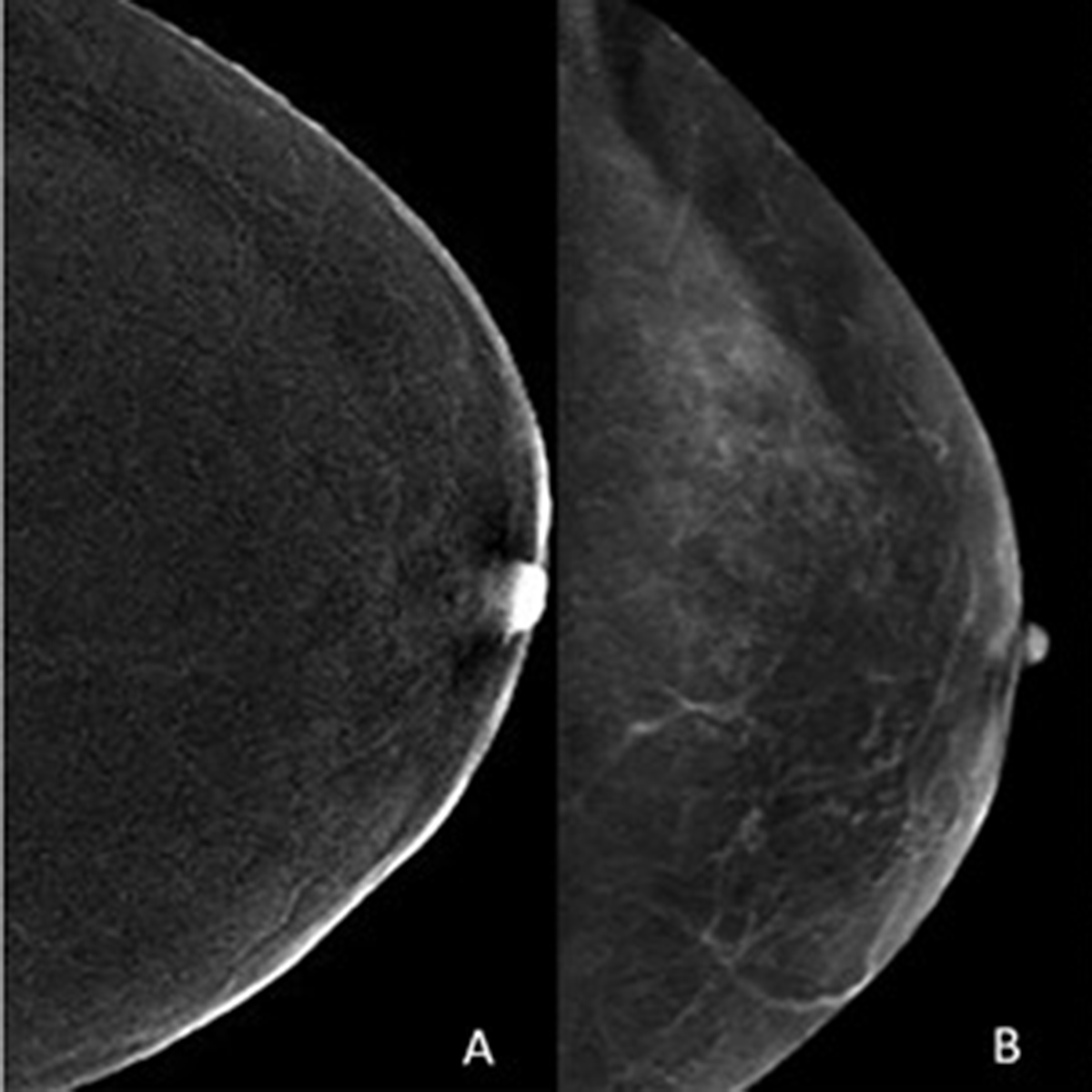
Of clinical importance is the fact that enhancing CEM-detected lesions that have an ultrasound correlate are more likely to be malignant. These data were also published by AJR in 2021 [8]. Among 153 enhancing lesions detected on CEM in 144 patients, the authors found ultrasound correlates in 47 (31%). Furthermore, this means that a substantial number of enhancing findings can potentially be sampled with ultrasound-guided biopsy (Fig. 3).
Fig. 3—57-year-old woman with history of left breast excision for lobular carcinoma in situ who underwent CEM. A: Low-energy mammogram shows no abnormality. B: Recombined mammogram shows enhancing 0.4-cm mass in 6-o’clock axis of left breast (arrow). Mass was evident only on recombined images. C: Image obtained during targeted ultrasound-guided core biopsy shows ultrasound correlate (arrow). Pathology result was invasive lobular carcinoma [8].
Diagnostic applications of CEM in breast imaging continue to evolve. In the July issue of AJR, CEM was compared with MRI for neoadjuvant therapy (NAT) response assessment [9, 10]. After NAT for breast cancer, CEM and MRI yielded similar assessments of lesion size (both slightly overestimated vs. pathology) and RECIST categories, and no significant difference in specificity for complete pathologic response. Duly noting that MRI had higher sensitivity for complete pathologic response, Bernardi et al. showed preliminary data suggesting that a delayed CEM acquisition 6 minutes after contrast injection could help detect residual ductal carcinoma in situ (DCIS) [10]. The authors concluded that while MRI remains the preferred test for NAT monitoring, the findings support CEM as a useful alternative when MRI is contraindicated or not tolerated [10, 11].
CEM may be a useful alternative to MRI in women with newly diagnosed breast cancer and breast augmentation. The findings of Carnahan et al. published in AJR last year suggest the plausibility of CEM for disease extent assessment in women with breast augmentation and contraindication or limited access to MRI [12].
The study evaluated 17 female breast cancer patients with breast implant augmentation, who underwent both CEM and MRI for staging. CEM and MRI were concordant for the index cancer in all 17 women. Six additional lesions were demonstrated by CEM and confirmed by MRI in 6 (35%) women: three multifocal, one multicentric, and two contralateral; two (33%) were malignant (one each invasive ductal and invasive lobular carcinoma). MRI did not identify any additional cancers not seen on CEM.
CEM-Guided Biopsy
Perhaps the largest unmet need for expertly curated CEM education surrounds CEM-guided biopsy. Case in point: recently FDA-approved—but not yet widely available—direct CEM-guided biopsy is often a necessary step in patient management. In the absence of CEM-guided biopsy capability, suspicious enhancing findings that have no definite correlate on low energy images, tomosynthesis, or ultrasound require possible MRI-guided biopsy for diagnosis. This increases cost and prolongs diagnostic workup. With the introduction of CEM-guided biopsy technology, this workflow is expected to become more streamlined and efficient. Our subspecialized presenters have personal experience with this technology and will deliver a comprehensive overview of the current state of knowledge and the future directions of CEM-guided biopsies.
CEM Essentials—and Beyond—at the ARRS Annual Meeting
Contemporary breast imagers must become more familiar with the range of indications and contraindications on CEM, such as normal variants, BPE, pathology, and artifacts. Focused sessions will also address interpretative skills in CEM—including appropriate use of the recently released BI-RADS CEM lexicon from the American College of Radiology—giving radiologists in private and academic practices alike applied insights from real-life cases.
Although the target audience for our course is predominantly medical imaging professionals considering or actively implementing CEM in practice, the curriculum presented live on Sunday, April 16 will also be relevant and valuable for recent residency or fellowship graduates, particularly those transitioning to imaging practices with established CEM services.
As the field moves forward, medical centers with established CEM programs will inevitably need to educate an incoming imaging workforce and new trainees who have not experienced enough clinical exposure to this modality in their previous practices or training programs. Apropos, “Contrast-Enhanced Mammography: The Essentials and Beyond” will also offer participants a unique opportunity to test and evaluate a newly developed online teaching module for CEM, purposefully designed to train the radiologists of today and tomorrow in clinical implementation of CEM in their own practices.
Perry H, Phillips J, Dialani V, Slanetz PJ, Fein-Zachary VJ, Karimova EJ, et al. Contrast-Enhanced Mammography: A Systematic Guide to Interpretation and Reporting. AJR 2019; 212:222–223
Breast Imaging Reporting & Data System (BI-RADS®) Contrast Enhanced Mammography (CEM) Supplement. ACR website. www.acr.org/-/media/ACR/Files/RADS/BI-RADS/BIRADS_CEM_2022.pdf. Published 2022. Accessed September 12, 2022
Karimi Z, Phillips J, Slanetz P, Lotfi P, Dialani V, Karimova J, et al. Factors Associated With Background Parenchymal Enhancement on Contrast-Enhanced Mammography. AJR 2020; 216:340–348
Lu AH, Zuley ML, Berg WA. Enhancing Cherry Hemangioma: A Mimic for Breast Cancer on Contrast-Enhanced Mammography. American Journal of Roentgenology. 2022;219(1):160-1.
The ACR Appropriateness Criteria® American College of Radiology Appropriateness Criteria. Supplemental Breast Cancer Screening Based on Breast Density. ACR website. acsearch.acr.org/docs/3158166/Narrative. Published 2021. Accessed September 12, 2022.
Hogan MP, Amir T, Sevilimedu V, Sung J, Morris EA, Jochelson MS. Contrast-Enhanced Digital Mammography Screening for Intermediate-Risk Women With a History of Lobular Neoplasia. AJR 2021; 216:1486–1491
Coffey K, Sung J, Comstock C, Askin G, Jochelson MS, Morris EA, et al. Utility of Targeted Ultrasound to Predict Malignancy Among Lesions Detected on Contrast-Enhanced Digital Mammography. AJR 2021; 217:595–604
Woodard S. Editorial comment: evidence supporting contrast-enhanced mammography (CEM) for monitoring neoadjuvant chemotherapy response and showing the potential of delayed CEM. AJR 2022;11
Bernardi D. et al. Contrast-enhanced mammography versus MRI in the evaluation of neoadjuvant therapy response in patients with breast cancer: a prospective study. AJR 2022; 14:1–11
Carnahan MB et al. Contrast-enhanced mammography for newly diagnosed breast cancer in women with breast augmentation: preliminary findings. AJR 2021; 217:855–856
Division of Pediatric Neuroradiology Orlando Health—Arnold Palmer Hospital for Children
Avery Wright, DO
Division of Pediatric Neuro-Oncology Orlando Health—Arnold Palmer Hospital for Children
Mohit Agarwal, MD
Division of Neuroradiology Medical College of Wisconsin
Lily Wang, MBBS, MPH
Division of Neuroradiology University of Cincinnati Medical Center
Karen L. Salzman, MD
Division of Neuroradiology University of Utah Medical Center
Primary brain tumors are the most common solid tumors in children, second only to leukemia in terms of cancer incidence, and are the leading cause of childhood cancer-related mortality [1, 2]. Tumors may present across all pediatric age groups, including infants, children, adolescents, and young adults, with the majority of cases presenting in the first decade of life. Clinical presentations vary, based upon the type of tumor, location, and patient age; however, the most common presenting symptoms include headaches, nausea and vomiting, and gait abnormalities [3]. In infants and very young children, obstructive hydrocephalus results in macrocephaly with bulging fontanelle [4]. Brainstem tumors commonly have symptoms associated with involved tracts and cranial nerves.
Imaging plays a crucial role in the initial workup, management, and post-treatment follow-up of primary pediatric posterior fossa tumors. Treatment options vary, based upon the tumor type, location, and patient age, and are beyond the scope of this InPractice review. The most common primary posterior fossa tumors in children that we will discuss and illustrate during our 2023 ARRS Annual Meeting Categorical Course session include (in descending order of frequency): medulloblastoma, pilocytic astrocytoma, ependymoma, diffuse midline glioma, and atypical teratoid-rhabdoid tumor.
Medulloblastoma
Medulloblastomas are high-grade (WHO grade 4) embryonal tumors and represent the most common malignant and the most common primary posterior fossa brain tumors in children [5]. Various subcategories of medulloblastomas have been described and used in the past; however, the latest molecular classification lists the following subtypes: wingless/integrated (WNT)—activated, sonic hedgehog (SHH)—activated, and non-WNT/non-SHH (also known as groups 3 and group 4), with additional subcategories for SHH-activated and non-WNT/non-SHH variants [6]. Classically, medulloblastomas were thought of as midline cerebellar tumors, but certain subtypes have a propensity for off-midline presentations.
General Imaging Features
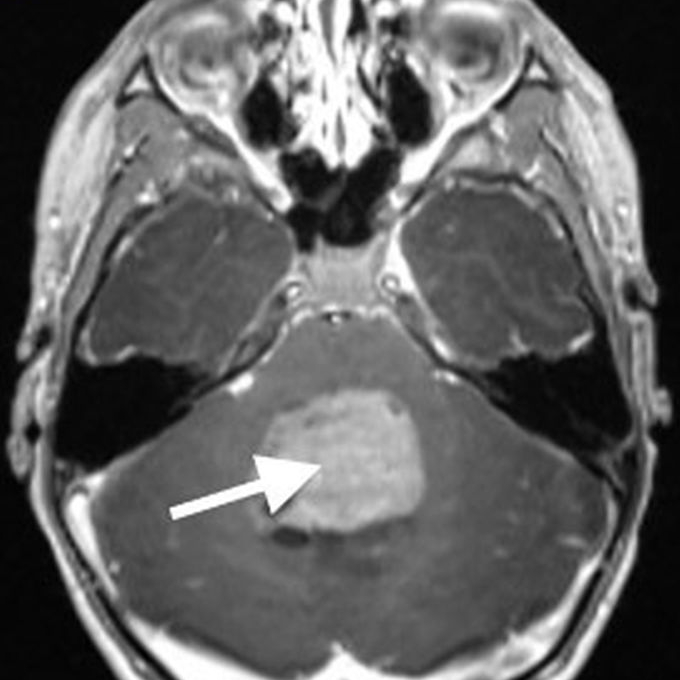
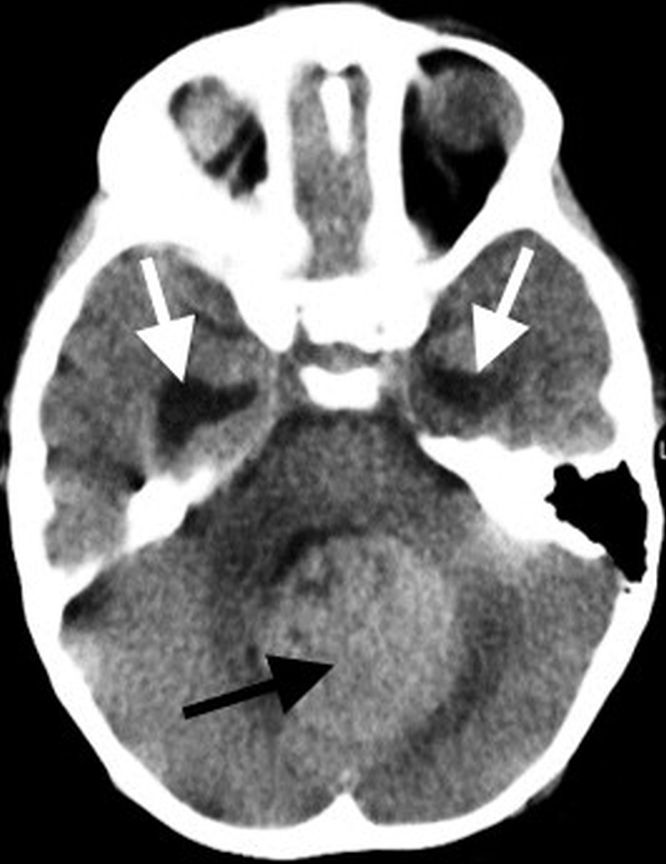
Imaging characteristics for the various subtypes of medulloblastoma are overall similar, reflecting that of densely packed, highly cellular tumors. Masses tend to be spherical in shape and displace adjacent structures, as opposed to the more pliable appearance of ependymomas. Increased density on CT and diffusion restriction on MRI are characteristic of medulloblastomas, reflective of their high cellularity. T2 signal intensity is variable, typically having areas of both increased and decreased T2 signal compared to cerebellar parenchyma. Small intralesional cysts are common, while intralesional hemorrhage and calcification are uncommon, though may occasionally be seen. Enhancement ranges from patchy to more robust solid enhancement [7, 8] (Fig. 1).
Fig. 1—8-year-old boy with progressive nighttime headache, nausea, vomiting. Surgical pathology confirmed medulloblastoma. Top, left to right: Axial CT image in brain window shows circumscribed hyperdense midline posterior fossa mass (black arrow) with dilatation of temporal horns of lateral ventricles secondary to obstructive hydrocephalus (white arrows); axial T2-weighted image shows mass (arrow) has signal intensity predominantly similar to gray matter, with additional small internal cystic components; axial T1-weighted postcontrast image shows avid enhancement of solid components of mass (arrow). Bottom, left and right: Characteristic restricted diffusion (arrows) is seen as increased signal intensity on DW image and decreased signal intensity on ADC map.
On MR spectroscopy, a high-grade tumoral spectrum is evident with increased choline and decreased N-acetyl aspartate peaks. A taurine peak just to the left of the choline peak may be a specific marker for medulloblastoma in the posterior fossa [9].
The frequency of metastatic disease varies depending upon the molecular subtype, ranging from approximately 10% to up to 45% at the time of initial presentation [5]. It is therefore important to image the spine prior to surgical resection and with subsequent surveillance imaging to evaluate for disseminated disease.
WNT-Activated Medulloblastoma
WNT-activated medulloblastomas are the least common subset and have the best overall prognosis. These tumors commonly present in older children and adolescents and may occur midline or laterally around the foramen of Luschka, cerebellar peduncle, and cerebellopontine angle [6, 7, 10].
SHH-Activated Medulloblastoma
SHH-activated medulloblastomas are a more heterogeneous subset than WNT-activated, with an overall intermediate prognosis. Tumors tend to be located laterally in the cerebellar hemispheres, since they are thought to arise from precursors in the external granule-cell layer of the cerebellum, but they may occur in the midline as well [6, 11]. There is a bimodal presentation, occurring most commonly in infants and then young adults, though they may also occur in children. The infantile variant tends to have extensive nodularity on histology and more frequently metastasizes [11, 12]. Nearly all nodular or desmoplastic variants fall into this category. SHH-activated medulloblastomas are stratified based on their TP53 status as either TP53-wildtype or TP53-mutant, with TP53-mutant portending a worse prognosis [6].
Non-WNT/Non-SHH Medulloblastoma, Groups 3 and 4
Non-WNT/non-SHH medulloblastomas are the most common molecular subsets, have an increased incidence in boys, present as midline vermian tumors, and often have classic or large cell anaplastic features on histology. Group 3 tumors tend to occur in infants and young children, have a higher incidence of metastases, and have the worst overall prognosis of any medulloblastoma tumor subset. Group 4 tumors are the most common subset, occur in older children and adolescents, and have an intermediate prognosis [6, 11]. In terms of distinguishing imaging features, group 3 tumors often have avid enhancement, while hypoenhancement is preferentially seen with group 4 tumors [13].
Pilocytic Astrocytoma
Pilocytic astrocytomas are the most common primary brain tumor in children, accounting for approximately one-third of all gliomas, and the second most common primary posterior fossa tumor in children after medulloblastomas. They are low-grade, WHO grade 1, tumors with an excellent prognosis in the setting of gross total surgical resection. Pilocytic astrocytomas result from MAPK pathway alterations, often with BRAF fusion or BRAF V600E point mutations. BRAF fusion is common in posterior fossa pilocytic astrocytomas and is associated with improved outcomes [14]. BRAF V600E point mutations, on the other hand, tend to be associated with poorer outcomes [15]. Increased frequency of pilocytic astrocytomas is seen in patients with neurofibromatosis type 1 (NF1), most commonly involving the optic pathways, though they may occur nearly anywhere with NF1 [16].
Posterior fossa pilocytic astrocytomas most often arise within the cerebellar hemispheres and are therefore lateral in location. Less commonly, they may be midline, arising from the cerebellar vermis. The classic imaging appearance is a large cystic mass with a peripheral solid nodule. More heterogeneous presentations, including a multicystic mass, predominantly solid mass with central cystic changes, or partially hemorrhagic mass, are less common [7, 17].
On MRI, the cystic component of the tumor is often similar to CSF signal intensity on T1 and T2 sequences, with the T2-FLAIR signal being more variable, based upon internal proteinaceous content. Solid portions of the mass avidly enhance, and there may also be enhancement along the margins of the cyst wall. A helpful distinguishing feature of a pilocytic astrocytoma, compared to other posterior fossa tumors, is the lack of diffusion restriction within the solid components of the tumor [18, 19] (Fig. 2).
Fig. 2—5-year-old boy with ataxia, nausea, vomiting. Surgical pathology revealed pilocytic astrocytoma. Left to right: Axial T2-weighted image shows off-midline cystic and solid posterior fossa mass (arrow) centered within left cerebellar hemisphere and subtle surrounding edema; coronal T1-weighted postcontrast image shows diffuse enhancement of peripheral solid nodular component of mass (arrow); axial DW shows no diffusion restriction.
Ependymoma
Ependymomas are the third most common primary posterior brain tumors, after medulloblastomas and pilocytic astrocytomas. The majority are classic, WHO grade 2, ependymomas, with more aggressive anaplastic ependymomas being WHO grade 3. Ependymomas are soft, pliable tumors that originate in or near the fourth ventricle and squeeze through the outlet foramina into adjacent spaces and cisterns. Because of their pliability, they often surround or encase neurovascular structures.
There are two subgroups of posterior fossa ependymomas: posterior fossa group A (PFA) and posterior fossa group B (PFB) [20]. PFA variants occur most often in infants, are lateral in location, and have a relatively poor prognosis. Because of the lateral location and common extension into the prepontine cistern, gross total resection is often difficult, and radiation therapy is typically avoided in infants because of the potential for morbidity. PFB variants occur in older children and adolescents, tend to arise from the floor of the fourth ventricle, and have a better overall prognosis than PFA variants [16, 21].
On MRI, ependymomas tend to be heterogeneously T2 hyperintense with variable enhancement. Cystic change and calcifications are common, with calcifications occurring in up to 50% of cases, much more common than is seen with medulloblastomas [7]. Given the relative pliability of the tumor, extension through fourth ventricular outlet foramina is characteristic. The presence of reduced or restricted diffusion is variable, but typically less than is seen with highly cellular medulloblastomas. The exception is with anaplastic ependymomas, which may have areas of restricted diffusion that are similar to medulloblastomas. Anaplastic ependymomas tend to have a higher frequency of disseminated metastatic disease and disease recurrence, with a poorer prognosis compared to lower-grade ependymomas [22]. The frequency of disseminated metastatic disease for ependymomas is less than that for medulloblastomas.
Diffuse Midline Glioma
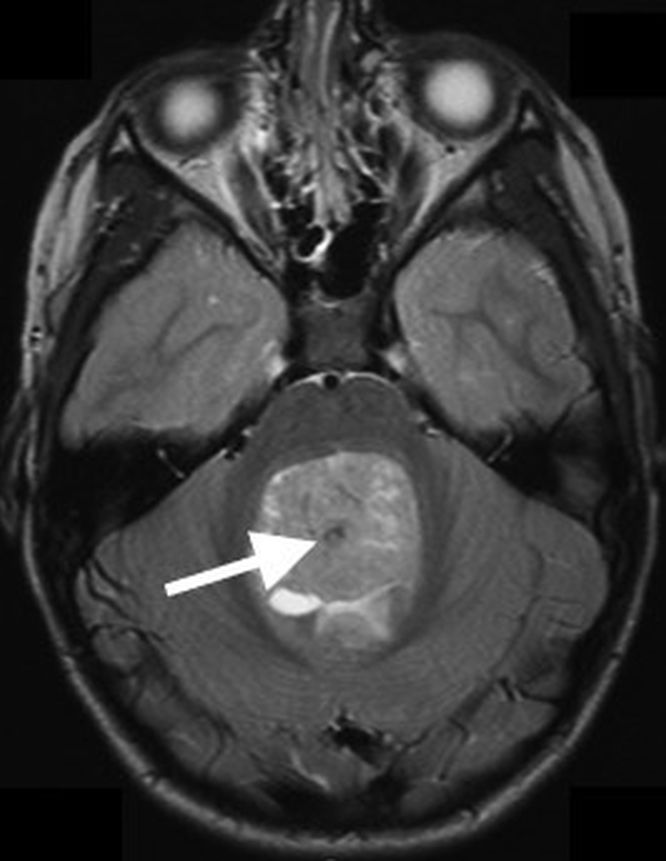
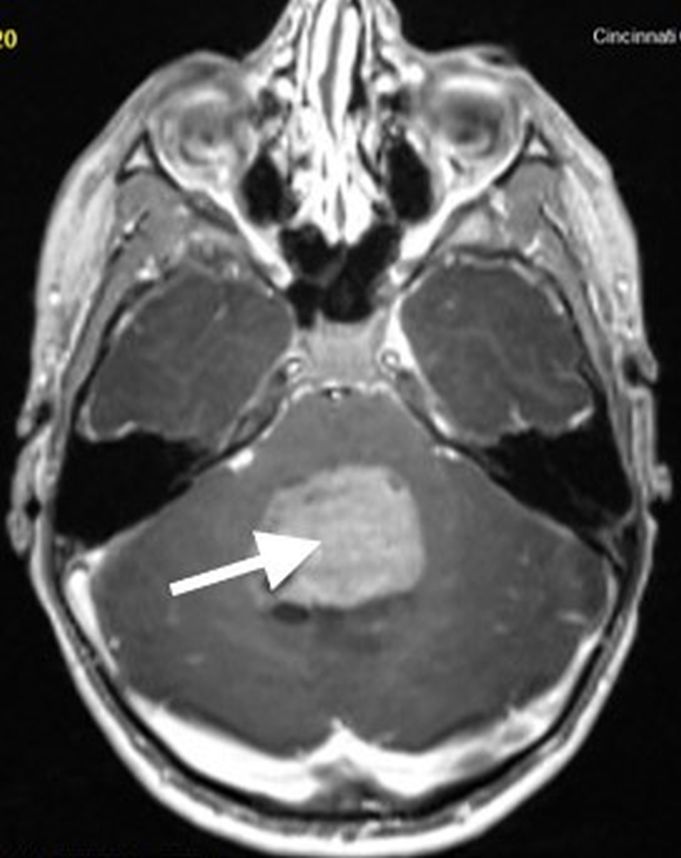
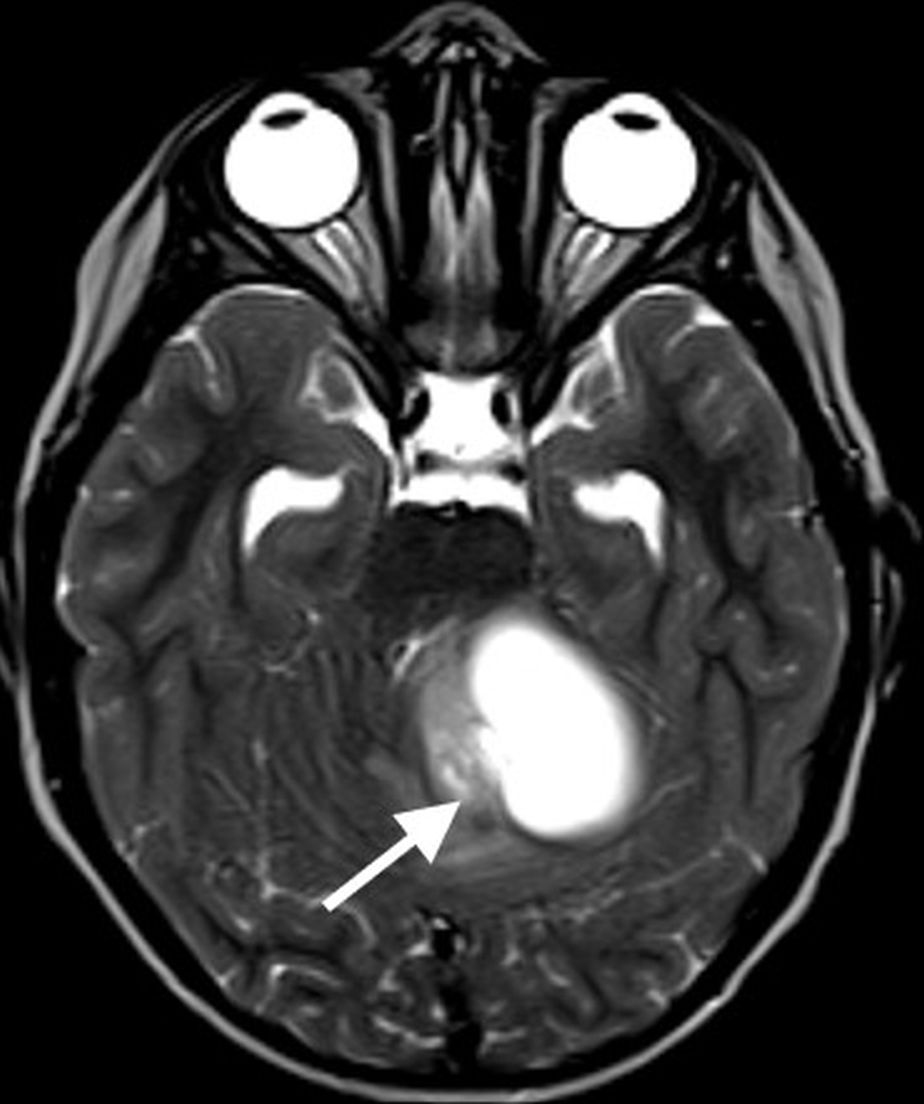
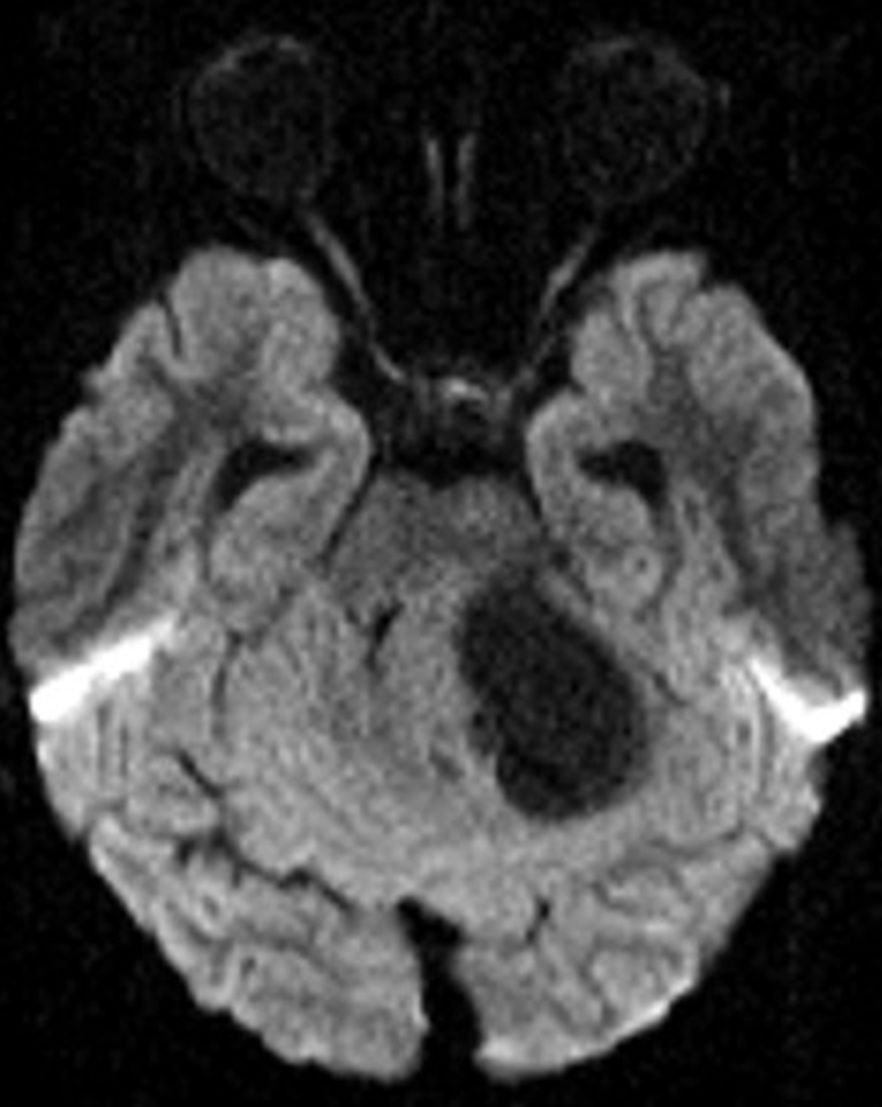
Diffuse midline gliomas (DMGs) “H3K27-altered” are highly aggressive pediatric brain tumors (WHO grade 4) that encompass the majority of lesions previously referred to as diffuse intrinsic pontine gliomas (DIPGs). Prognosis is dismal with a median survival of approximately 11 months from diagnosis [23]. Given the brainstem location, the most common clinical presentations include cranial nerve palsies, pyramidal tract signs (paresis, hyperreflexia, or positive Babinski reflex), and cerebellar signs (dysmetria, ataxia, dysarthria, or nystagmus) [23]. DMGs tend to occur in younger children, with median age at presentation around 6 years [24].
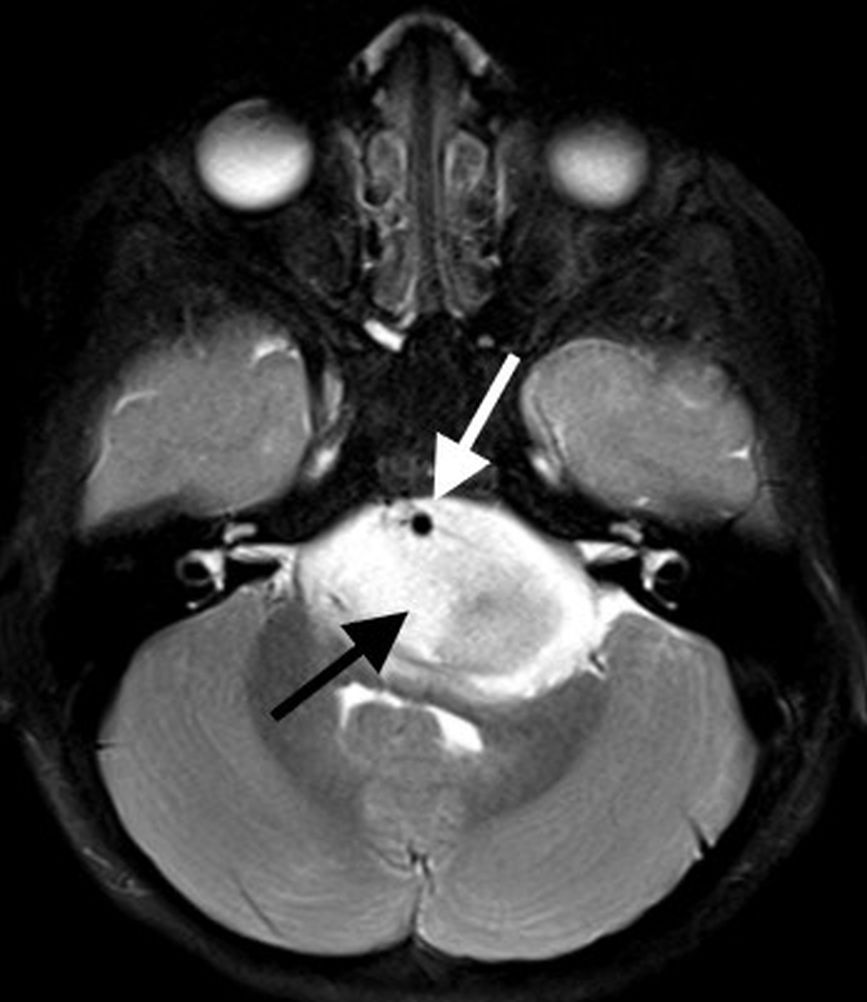
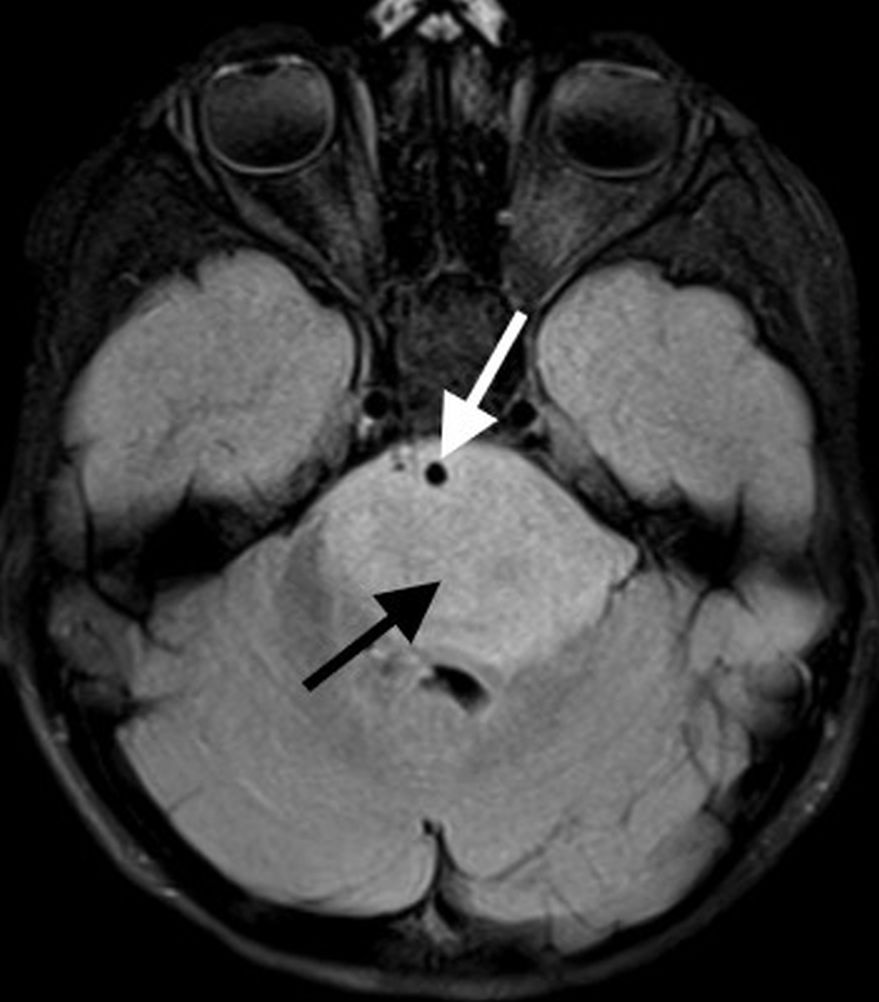
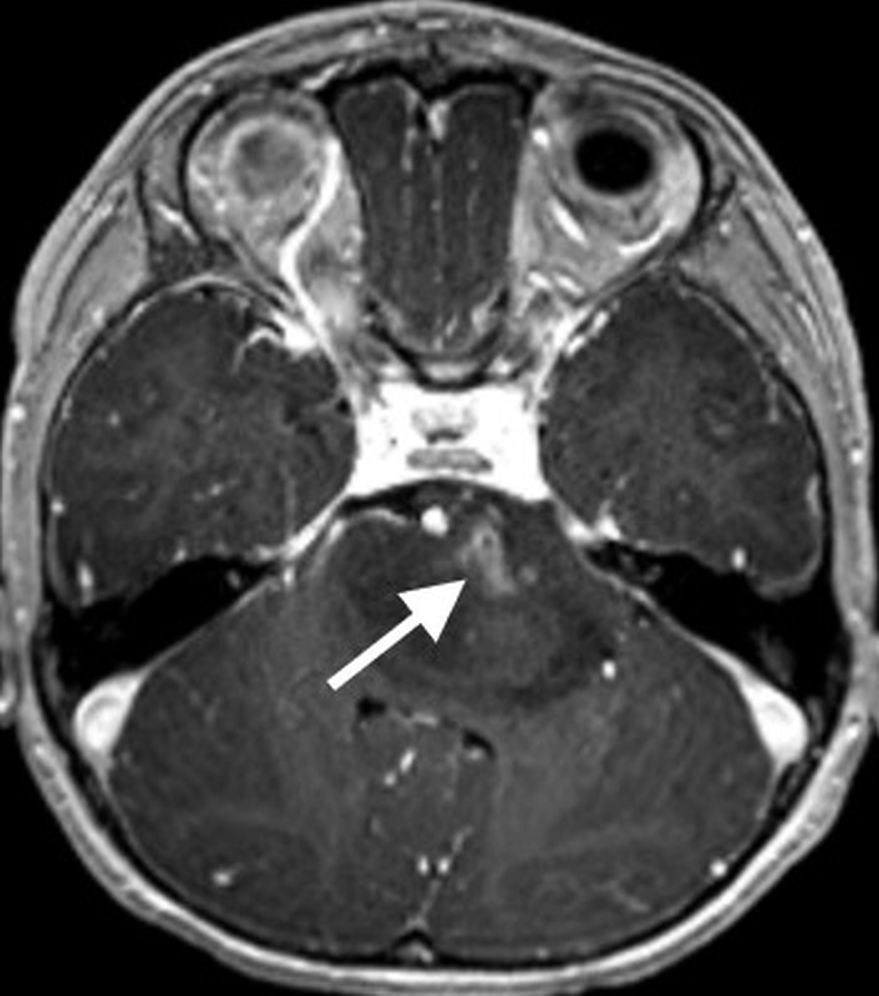
On MR imaging, DMGs present as a diffuse, ill-defined, T2 hyperintense, expansile masses centered within the pons. The degree of enhancement is variable, often absent at initial presentation and typically patchy when present (Fig. 3).
Fig. 3—7-year-old girl with ataxia, nystagmus, torticollis. Patient presumptively treated for DMG. Left and center: Axial T2-weighted and FLAIR images demonstrate infiltrative, expansile brainstem mass (black arrows) centered within pons and extending into brachium pontis on left. Exophytic components engulf basilar artery (white arrows) anteriorly and partially efface fourth ventricle posteriorly. Right: Axial T1-weighted postcontrast image shows mild patchy enhancement along ventral aspect of mass (arrow) on left.
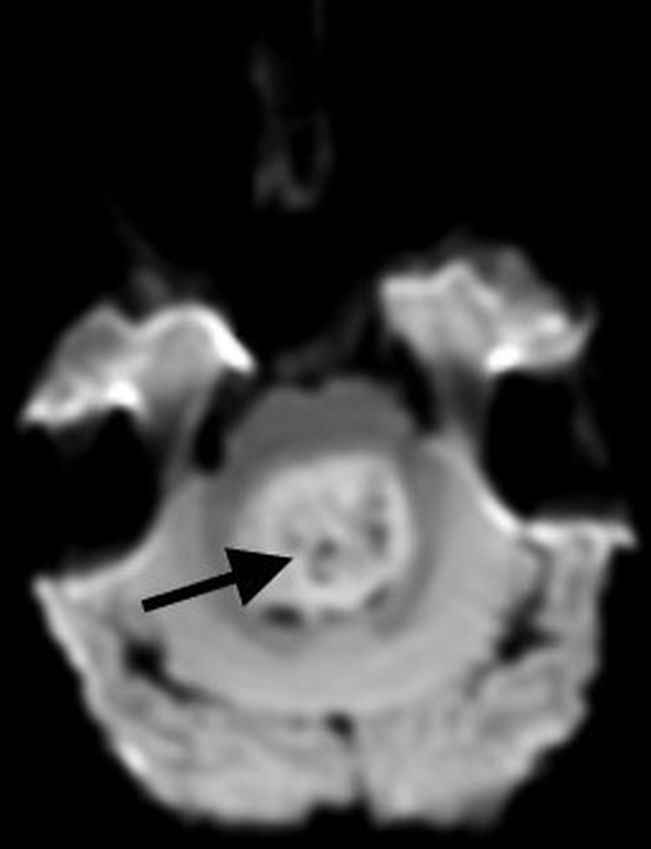
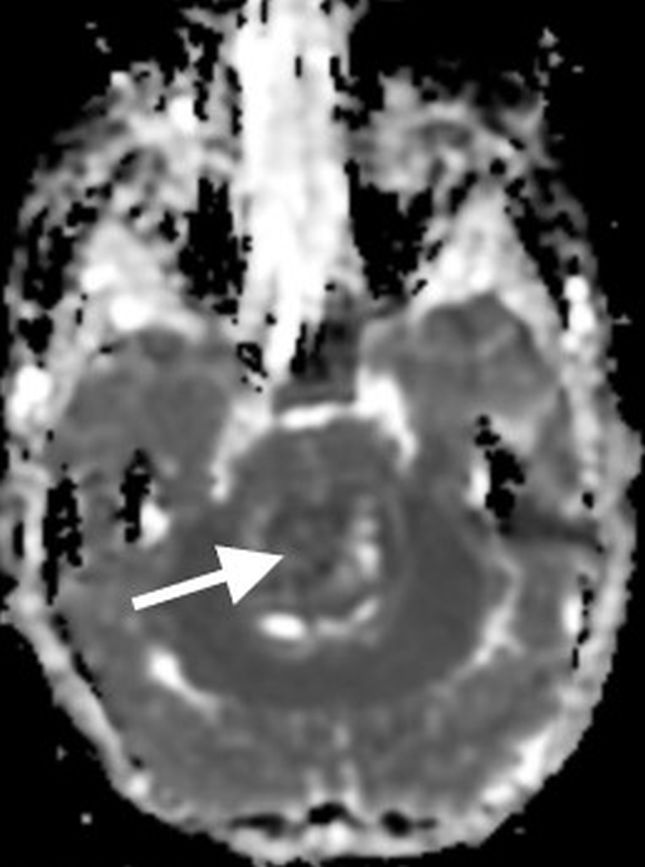
Peripheral enhancement commonly occurs along margins of central necrosis, which occurs more frequently after radiation therapy [25]. Intralesional hemorrhage is uncommon, but areas of hemosiderin deposition may be seen on susceptibility-weighted sequences. Focal areas of restricted diffusion develop in the majority of cases. The presence of central necrosis, diffusion restriction, or enhancement at the time of initial diagnosis has been shown to portend a worse prognosis [24].
Extrapontine spread is common throughout the brainstem, into the thalami and adjacent structures, through the cerebellar peduncles, and into the cerebellar hemispheres. Exophytic components engulf the basilar artery anteriorly and efface the fourth ventricle posteriorly. Disseminated metastatic disease is uncommon, though may be seen occasionally.
Historically, DMGs have been treated presumptively when characteristic imaging features are present, reserving biopsy for cases with nonclassic imaging features or when tissue sampling is required for a clinical trial eligibility. However, more centers are now performing biopsies prior to treatment to confirm molecular classification and histology, shed light on potential prognosis, and help advance investigation of future adjuvant therapies. When biopsy is performed, the posterolateral portion of signal abnormality is typically targeted to minimize potential morbidity. If focal areas of diffusion restriction are present, these areas tend to have the highest diagnostic yield, if they can be safely accessed and sampled [26].
Atypical Teratoid-Rhabdoid Tumor
Atypical teratoid-rhabdoid tumors (ATRTs) are rare and highly aggressive (WHO grade 4) embryonal tumors that tend to occur in infants and young children, with the majority of cases presenting under 3 years of age. As with medulloblastomas, posterior fossa ATRTs may be midline or off-midline and are highly cellular with areas of diffusion restriction. Imaging features significantly overlap with medulloblastoma; therefore, patient age is one of the key features in suggesting ATRT versus medulloblastoma. Compared to medulloblastomas, ATRTs tends to have a more heterogeneous imaging appearance, with a higher incidence of intralesional hemorrhage and calcification, as well as a higher incidence of disease dissemination at the time of presentation [27, 28].
For most cases of primary posterior fossa tumors in children, the correct diagnosis can be suggested based upon distinguishing imaging features, with remaining cases requiring a thoughtful differential diagnosis in the setting of overlapping or nonspecific imaging findings. Our Categorical Course session will focus on recognizing characteristic imaging features for the most common primary pediatric posterior fossa tumors.
References
1. Pollack IF, Agnihotri S, Broniscer A. Childhood brain tumors: current management, biological insights, and future directions. J Neurosurg Pediatr 2019; 23:261–273
2. Pollack IF. Brain tumors in children. N Engl J Med 1994; 331:1500–1507
3. Prasad KSV, Ravi D, Pallikonda V, Raman BV. Clinicopathological study of pediatric posterior fossa tumors. J Pediatr Neurosci 2017; 12:245–250
4. Picariello S, Spennato P, Roth J, et al. Posterior fossa tumours in the first year of life: a two-centre retrospective study. Diagnostics (Basel) 2022; 12:1–12
6. Cohen AR. Brain tumors in children. N Engl J Med 2022; 386:1922–1931
7. Jaju A, Yeom KW, Ryan ME. MR imaging of pediatric brain tumors. Diagnostics (Basel) 2022; 12:1–24
8. Shih RY, Koeller KK. Embryonal tumors of the central nervous system. RadioGraphics 2018; 38:525–541
9. Panigrahy A, Krieger MD, Gonzalez-Gomez I, et al. Quantitative short echo time 1H-MR spectroscopy of untreated pediatric brain tumors: preoperative diagnosis and characterization. AJNR 2006; 27:560–572
10. Patay Z, DeSain LA, Hwang SN, et al. MR imaging characteristics of wingless-type-subgroup pediatric medulloblastoma. AJNR 2015; 36:2386–2393
11. Juraschka K, Taylor MD. Medulloblastoma in the age of molecular subgroups: a review. J Neurosurg Pediatr 2019; 24:353–363
12. Cavalli FMG, Remke M, Rampasek L, et al. Intertumoral heterogeneity within medulloblastoma subgroups. Cancer Cell 2017; 31:737–754.e6
13. Perreault S, Ramaswamy V, Achrol A, et al. MRI surrogates for molecular subgroups of medulloblastoma. AJNR 2014; 35:1263–1269
14. Becker AP, Scapulatempo-Neto C, Carloni AC, et al. KIAA1549: BRAF gene fusion and FGFR1 hotspot mutations are prognostic factors in pilocytic astrocytomas. J Neuropathol Exp Neurol 2015; 74:743–754
15. Nobre L, Zapotocky M, Ramaswamy V, et al. Outcomes of BRAF V600E pediatric gliomas treated with targeted BRAF inhibition. JCO Precis Oncol 2020; 4:561–571
16. AlRayahi J, Zapotocky M, Ramaswamy V, et al. Pediatric brain tumor genetics: what radiologists need to know. RadioGraphics 2018; 38:2102–2122
17. O’Brien WT. Imaging of Primary posterior fossa brain tumors in children. J Am Osteopath Coll Radiol 2013; 2:2–12
18. Novak J, Zarinabad N, Rose H, et al. Classifcation of paediatric brain tumours by diffusion weighted imaging and machine learning. Sci Rep 2021; 11:2987
19. Koral K, Alford R, Choudhury N, et al. Applicability of apparent diffusion coefficient ratios in preoperative diagnosis of common pediatric cerebellar tumors across two institutions. Neuroradiology 2014; 56:781–788
20. Louis DN, Perry A, Wesseling P, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol 2021; 23:1231–1251
21. Wu J, Armstrong TS, Gilbert MR. Biology and management of ependymomas. Neuro Oncol 2016; 18:902–913
22. Yuh EL, Barkovich AJ, Gupta N. Imaging of ependymomas: MRI and CT. Childs Nerv Syst 2009; 25:1203–1213
23. Hoffman LM, Veldhuijzen van Zanten SEM, Colditz N, et al. Clinical, radiologic, pathologic, and molecular characteristics of long-term survivors of diffuse intrinsic pontine glioma (DIPG): a collaborative report from the International and European Society for Pediatric Oncology DIPG Registries. J Clin Oncol 2018; 36:1963–1972
24. Leach JL, Roebker J, Schafer A, et al. MR imaging features of diffuse intrinsic pontine glioma and relationship to overall survival: Report from the International DIPG Registry. Neuro Oncol 2020; 22:1647–1657
25. Aboian MS, Solomon DA, Felton E, et al. Imaging characteristics of pediatric diffuse midline gliomas with histone H3 K27M mutation. AJNR 2017; 38:795–800
26. Biery MC, Noll A, Myers C, et al. A protocol for the generation of treatment-naïve biopsy-derived diffuse intrinsic pontine glioma and diffuse midline glioma models. J Exp Neurol 2020; 1:158–167
27. Arslanoglu A, Aygun N, Tekhtani D, et al. Imaging findings of CNS atypical teratoid/rhabdoid tumors. AJNR 2004; 25:476–480
28. Jin B, Feng XY. MRI features of atypical teratoid/rhabdoid tumors in children. Pediatr Radiol 2013; 43:1001–1008
@RHWiggins Associate Dean of CME Professor of Radiology and Imaging Sciences University of Utah Health Science Center
Subdivided at the hyoid bone, the soft-tissue core of the extracranial segment of the head and neck can be divided further into two discrete areas: the suprahyoid neck and the infrahyoid neck. Whereas the infrahyoid portion lies inferiorly between the hyoid bone and clavicles, the suprahyoid area comprises the deep spaces between the base of the skull and the hyoid bone. While decades ago, lesions in the deep suprahyoid neck lead to a vague report listing a long differential diagnosis, an understanding of the suprahyoid neck anatomic space can lead to an accurate space-specific differential diagnosis. Here, three layers of cervical fascia help to define all the separate spaces in the deep part of our face.
Presented live on Sunday, April 16 during the 2023 ARRS Annual Meeting in Honolulu, HI, our “The Suprahyoid Neck—Pathology Through Anatomy” Featured Session will focus on reviewing important anatomical subunits and common pathologies of the suprahyoid neck: the parapharyngeal, pharyngeal mucosal, masticator, parotid, carotid, retropharyngeal, danger, and perivertebral spaces (Fig. 1).
Fig. 1—Axial drawing depicts relevant anatomy of paramaxillary and submastoid approaches. In submastoid approach, needle takes approach that is out of axial plane to pass caudal to mastoid process. Approximate location of seventh cranial nerve as it courses inferior stylomastoid foramen is labeled.
Examining imaging findings crucial for diagnostic radiologists and neuroradiologists alike to identify, attendees will enhance their clinical performance through a greater, more holistic understanding of cross-sectional anatomy and common pathologies that lead to various lesions in these regions—each a critical check point for accurate interpretation of radiological studies of the suprahyoid neck.
Speaking of studies, our illustrious Featured Sunday Session faculty are especially looking forward to leading breakout sessions regarding the various modalities most frequently found in imaging the suprahyoid neck. The comparative insensitivity of CT for artifacts, CT’s more comprehensive delineation of facial structures, and the promise of contrast-enhanced images to reveal critical vasculature continue to make CT more advantageous than ultrasound guidance (Fig. 2).
Fig. 2—72-year-old with right facial and neck pain and dysphagia associated with 7.7-kg (17-lb) unintentional weight loss. Left: Axial contrast-enhanced CT image of neck shows incidentally identified soft-tissue mass centered in right deep parotid space. Right: Axial CT image obtained with patient positioned with his head angled contralateral to lesion. Needle is advanced percutaneously, caudal to mastoid tip and through sternocleidomastoid muscle. It is then advanced with tip oriented cranially for access to parotid lobe lesion.
And because CT-guided fine-needle aspiration and biopsy can be performed with patients in three positions (supine, prone, lateral decubitus), multiple clinical studies in the imaging literature continue to conclude that this procedure remains safe and effective for obtaining tissue to diagnosis lesions of the head and neck. For quick reference, we encourage you to consult the following preprocedural patient care checklist for fine-needle aspiration and/or biopsy to help promote a professional and efficient imaging encounter with your patients:
Procedure
Relevant to ongoing care?
Anesthesia
Moderate sedation available?
General anesthesia more appropriate?
Consent Approval
Both procedure and sedation?
Imaging
Preprocedural images available for review?
Positioning
Planned trajectory verified?
Patient able to tolerate?
Lab Results
Values within acceptable ranges?
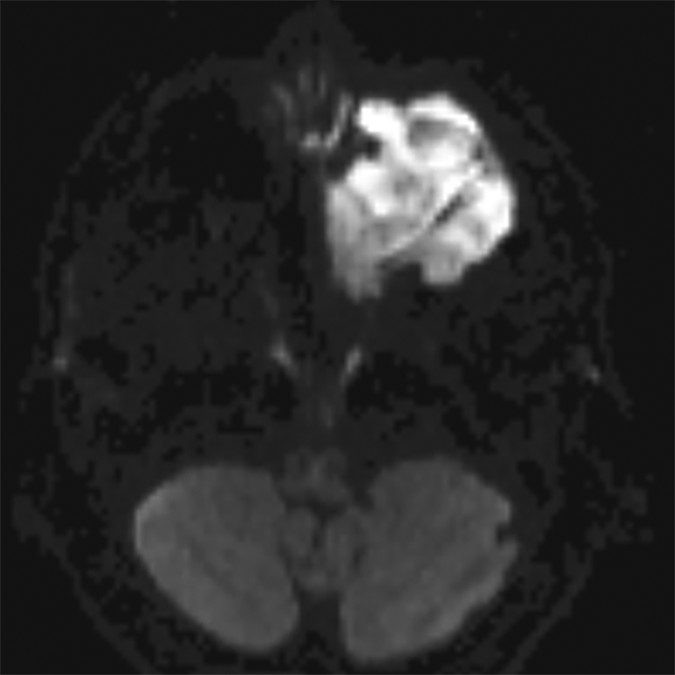
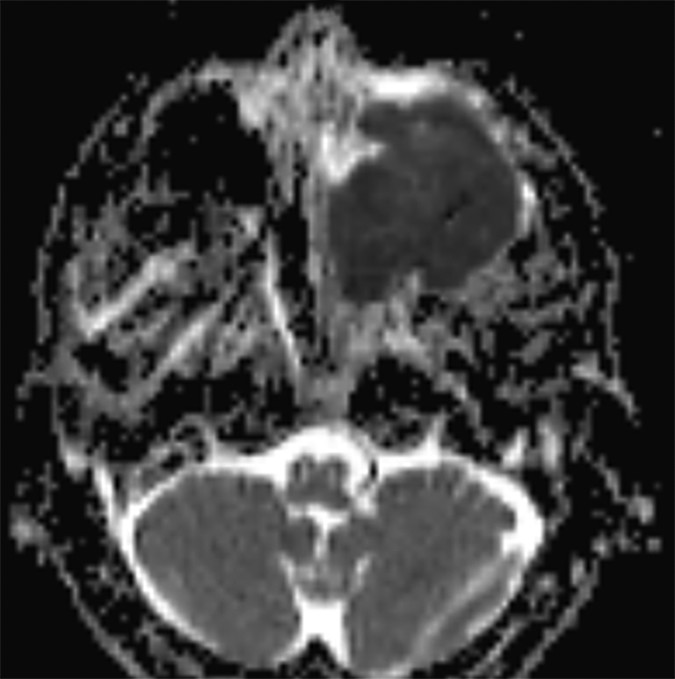
In certain instances, diffusion pulse sequences can offer a complementary adjunct to conventional MR pulse sequences, but neither diffusion-weighted imaging (DWI) or diffusion tensor imaging (DTI) should be utilized as a standalone technique for characterizing the benignity of head and neck lesions. Moreover, since mean apparent diffusion coefficients (ADC) values derived from DTI parameters are characteristically lower than ADC values developed from DWI parameters—frequently lower than reported malignant threshold values—the two should not be used interchangeably (Fig. 3).
Fig. 3—48-year-old with sinonasal neuroendocrine carcinoma. Left: Mass appears bright on diffusion-tensor imaging trace image (left) and dark on corresponding apparent diffusion coefficient (ADC) map (right), consistent with reduced diffusivity in high cellularity lesion.
With personalized, precision medicine becoming increasingly more critical for our patients in today’s value-based health care environment, the topic of the suprahyoid neck is particularly timely for medical imagers at all professional levels and of every practice type, notably so for head and neck radiologists, neuroradiologists, and in-training imagers of both subspecialties. Closely working alongside head and neck surgical teams—often on complex cases of deep space neck masses with widely differential diagnoses—practicing radiologists must intimately understand each significant space of the suprahyoid neck, as well as their surrounding fascial boundaries.
Unique in the quality of the educators and the breadth of the curriculum, our “The Suprahyoid Neck—Pathology Through Anatomy” live event from Oahu Island on Sunday the 16th will also address key concepts for radiologists to improve their accuracy in reporting complex imaging cases. A key didactic point will be how a better understanding of suprahyoid neck anatomy can lead the imager to a space-specific differential and diagnosis. Once again, just as we concluded the ARRS “Temporal Bone Imaging Made Easy” symposium this March, I will then review top points from all the earlier expert presentations. We will officially adjourn after another spirited Q&A block, allowing faculty to address individual questions regarding both anatomical and pathological considerations when imaging the suprahyoid neck spaces.
The Upper Aerodigestive Tract
Also presented live on Sunday, April 16 during the 2023 ARRS Annual Meeting in Hawaii, our “The Upper Aerodigestive Tract” session will review essential anatomy and pathology of this tract surrounding the suprahyoid neck spaces. Each subunit of the upper aerodigestive tract will be examined, including the nasal cavity, nasopharynx, oral cavity, oropharynx, larynx, hypopharynx, cervical trachea, and cervical esophagus. Esteemed faculty for this Featured Sunday Session have prepared clinically focused sessions on important anatomical subunits, examining cross-sectional anatomy and pathology findings that are critical for the head and neck radiologist to understand for each region. Participants will enhance their performance by gaining a greater understanding of common pathologies that occur, honing in on critical check points for accurate interpretation of head and neck imaging studies of the upper aerodigestive tract, which is critical for certain pathologies—especially so for squamous cell carcinoma.
As an instructional topic for medical imaging professionals, the upper aerodigestive tract is timely in today’s health care environment, too. Awareness and appreciation of the many issues that can arise are indispensable to rendering better health care for our patients. Specifically, when collaborating with head and neck surgeons on non-cutaneous head and neck squamous cell carcinoma cases, it is the imaging that determines the staging—and, therefore, the therapy—in these complex cases.
Similar to our “The Suprahyoid Neck—Pathology Through Anatomy” course on the same day, an overall primer on critical spaces will be presented first, before diving into the more detailed subunit lectures our experts have prepared. Once more, each region of the upper aerodigestive tract will be assessed in functional terms alongside normal imaging findings, followed by a thorough analysis of pathologies for common head and neck cancers, as well as important mimics and differentials.
@AChhabraMD Professor of Radiology Chief of Musculoskeletal Imaging UT Southwestern Medical Center Parkland Health & Hospital System
Collectively, ultrasound, electromyography, and even physical findings play a role in diagnosing anomalies of the peripheral nervous system. Increasingly, though, MR neurography (MRN) is becoming very common for the evaluation of peripheral neuropathy. This enhanced adoption is due to technological advancements in imaging quality and acquisition speed, such as newer 3D techniques, improved coil equipment, sparser k-space sampling, and compressed sensing, etc. In fact, in today’s tertiary care setups, MRN is being quickly incorporated for the workups of peripheral neuropathy and plexopathy patients, due to both need and ask from the peripheral nerve physicians, orthopedic surgeons, and pain management specialists. Although many articles about the evolution of MRN have been published in the clinical literature, thus far, no standards for the evaluation and recording of peripheral nerve pathologies on MRI have been acknowledged, much less validated.
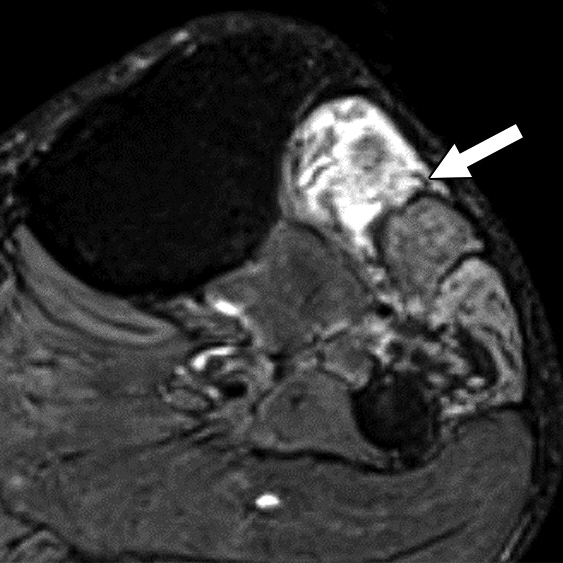
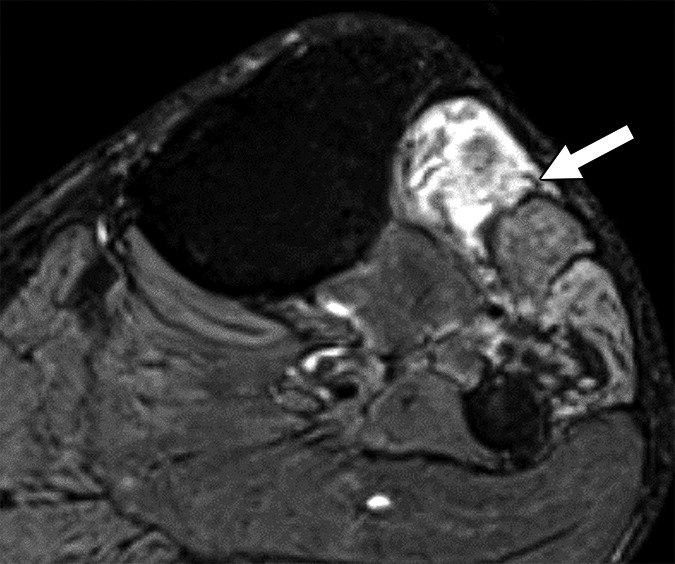
Our retrospective study included 100 patients with nerve imaging examinations and a variety of known clinical diagnoses. Utilizing mutually agreed-upon qualitative benchmarks for classifying and grading peripheral neuropathies, different classes were established to account for the spectrum of underlying pathologies (unremarkable, injury, neoplasia, entrapment, diffuse neuropathy, not otherwise specified, and postintervention state) with subclasses to describe lesion severity or extent. Validation was performed by 11 fellowship-trained musculoskeletal radiologists across 10 institutions, and after initial multimedia training, all 100 cases were blind-presented to readers (Fig. 1).
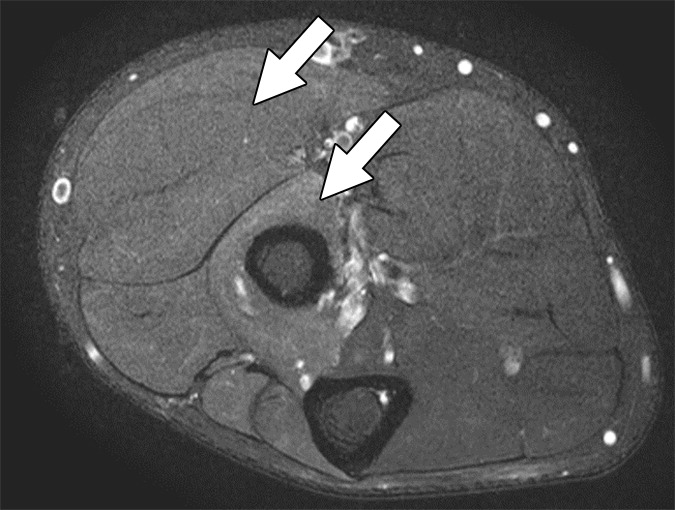
Fig. 1—Neuropathy Score Reporting and Data System (NS-RADS) subclass I3 M2. Axial fat-suppressed T2-weighted (left) and T1-weighted (right) images show extensor compartment and peroneal compartment denervation changes with fatty infiltration, edemalike signal, and mild atrophy (arrows) consistent with NS-RADS subclass M2.
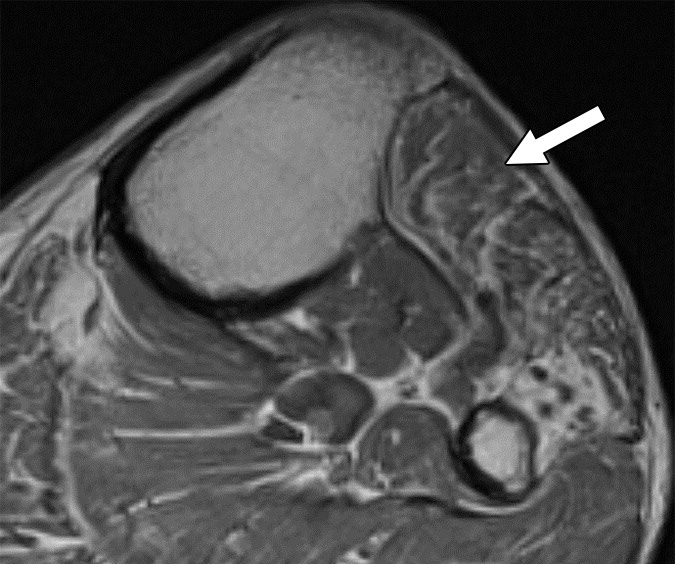
Offering a uniform lexicon and practical guideline for reporting neuropathic conditions on MRI, ultimately, NS-RADS accuracy for determining milder versus more severe categories per radiologist ranged from 88% to 97% for nerve lesions and from 86% to 94% for muscle abnormalities (Fig. 2).
Fig. 2—Neuropathy Score Reporting and Data System (NS-RADS) subclass M1. Axial T1-weighted (left) and STIR (right) images depict denervation edemalike signal of extensor muscles of dorsal and mobile wad compartments with no fatty infiltration or atrophy, consistent with NS-RADS subclass M1. (Arrows in right show edemalike signal of muscles.)
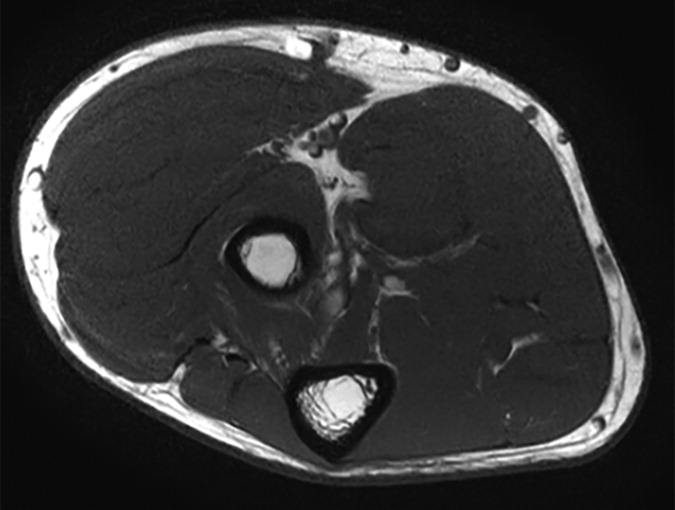
On the basis of the overall promising interrater agreement shown in this study, we believe that the newly proposed NS-RADS classification will perform as well in routine practice as it did in this initial validation study (Fig. 3).
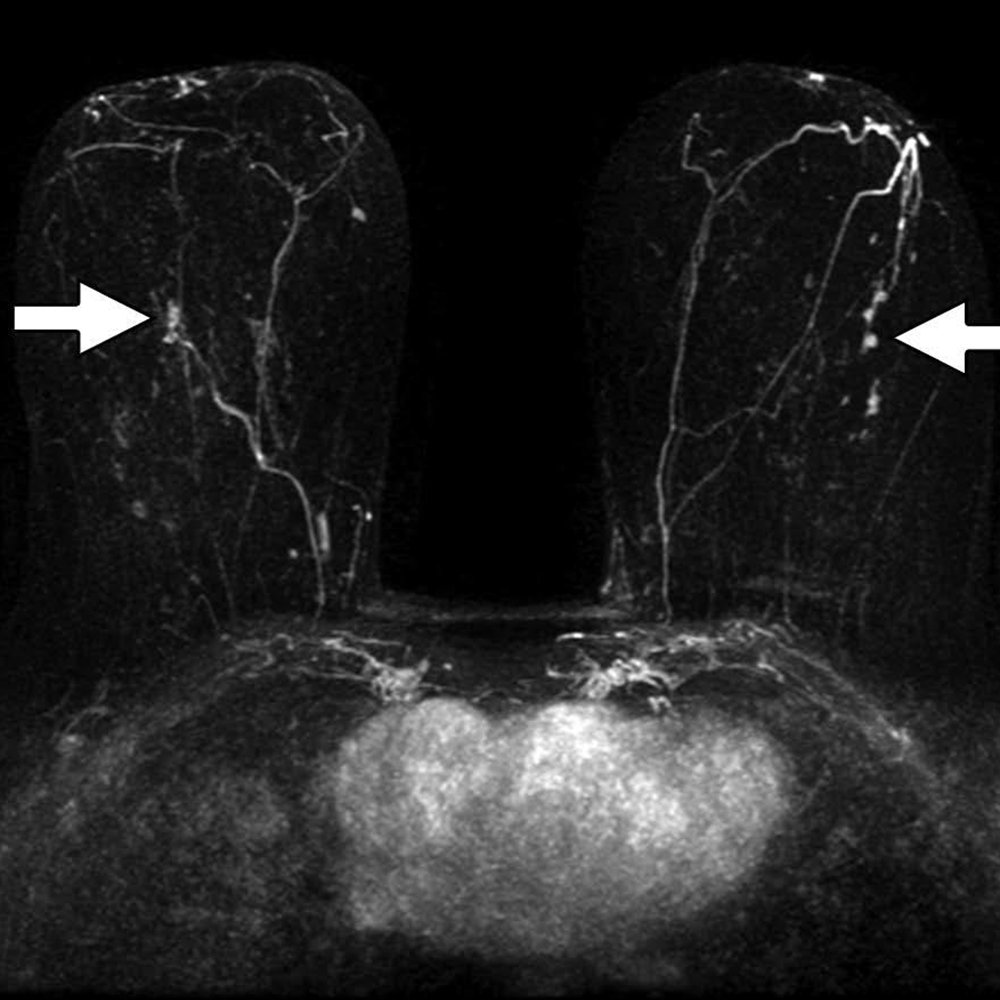
Fig. 3—Neuropathy Score Reporting and Data System (NS-RADS) subclass E2 M0. Axial (left) and oblique coronal (right) fat-suppressed T2-weighted images show proximally enlarged and hyperintense ulnar nerve (arrows) and normal nerve caliber distal to cubital tunnel (arrowhead on right).
However, we must acknowledge several barriers that still exist for learning and successful incorporation of routine MRN in radiology practices:
lack of widespread usage of technology, especially information on recent advancements
optimization for different tissue resolutions
complexity of peripheral nerve anatomy
uniformity of reporting with multidisciplinary teams
paucity of knowledge about diagnostic imaging criteria for lesion classification—something NS-RADS intends to correct
NS-RADS Details at ARRS Annual Meeting in Hawaii
Presented live during the 2023 ARRS Annual Meeting in Honolulu, HI, “MR Neurography and NS-RADS: Assist Your Neuropathy and Pain Patients” will focus on the latest advances in MRN and its practical application in routine imaging practice. Pertinent for practicing radiologists, musculoskeletal and neuroradiology subspecialists, fellows and residents in diagnostic radiology, and even radiologic technologists, six experts in MRI protocol and sequence design will deliver a two-hour categorical session. This session has been expertly curated, covering one anatomic site at a time. The majority of our lectures will be nerve-focused—reviewing and updating NS-RADS and detailing innovative MRN techniques for brachial plexus, LS plexus, facial, intercostal, as well as peripheral nerves. Our panel will also address 2D vs. 3D MRI correlations, highlighting relative advantages and disadvantages of different sequences.
Moving forward, modern MRI readers need to be fluent in the latest MRN features of different neuropathies, as well as related syndromes and classifications. We will also discuss current research projects and future applications. By incorporating these imaging interpretation criteria and expert insights from different tertiary care institutes, imaging professionals can impact diagnostic strategies, thus altering management decisions of neuropathy patients for improved outcomes.
Every year, medical students, early in their educational journeys, are encouraged by deans and other high-ranking medical school administrators to consider primary care (internal medicine, family medicine, or pediatrics) as a career choice. Most of us chose a different, more specialized route and wound up in radiology.
Now, I would like to encourage you to be a primary radiologist. By saying primary radiologist, I am not encouraging you to go into primary care, but rather to be the best radiologist that you can be. Primary radiologists are leading radiologists—working at a very high level, communicating clearly and effectively with referring physicians and patients, and keeping up to date with new developments in imaging and medicine. Most practices or groups have a primary radiologist—the highly accurate radiologist who is consulted on the most difficult cases and who is always available to help.
The primary radiologist’s role is based heavily on earning the respect of others. A primary radiologist is the one you and others turn to when you need an expert opinion. Oftentimes, a colleague will ask, did you show the case to Dr. _____? Alternatively, one may want an opinion on how Dr. _____ would approach a difficult procedure.
It is difficult to be a primary radiologist. There are ongoing global stressors, like the COVID-19 pandemic, and stressors affecting radiologists, including high burnout rates and an ever-increasing workload. Bhargavan et al. noted that when 2006–2007 data was compared to 2002–2003 data, the annual workload per full-time equivalent radiologist increased by 7%. When 2006–2007 data was compared to data from 1991–1992, the annual workload per full-time equivalent radiologist increased by 70.3%! Now, 2006–2007 seems like a long time ago, and, undoubtedly, workloads have continued to rise over the last 15 years.
How do we become primary radiologists in the current milieu? When we think of doing a great job, we need to define success. Success may be defined differently by deans, hospital administrators, chairs, section heads, and individual radiologists. As many of us are working very hard these days, it makes sense to think about what success means. John Wooden served as the basketball coach at the University of California, Los Angeles (UCLA) from 1948 to 1975. During that time, he led the UCLA Bruins to 10 National Collegiate Athletic Association (NCAA) basketball championships. I like John Wooden’s definition of success. Coach Wooden stated that “success is peace of mind which is a direct result of self-satisfaction in knowing you did your best to become the best that you are capable of becoming.”
In Coach Wooden’s Pyramid of Success, industriousness and enthusiasm are major cornerstones. Regarding industriousness, I don’t see radiologists’ workloads diminishing any time soon. In our current world of radiology, I agree with Coach Wooden, who noted that “there is no substitute for work. Worthwhile results come from hard work and careful planning.” When discussing planning and preparation, Coach Wooden stated that “failing to prepare is preparation for failure.” This important maxim applies to individual cases and procedures, as well as to our overall growth and development.
As we strive to be primary radiologists, our continued growth and development is based on self-assessment and identifying educational opportunities to rectify our perceived deficiencies. As we head into a new academic year and try to find top-notch educational content to fill our gaps, I suggest looking into the vast portfolio of educational offerings from our American Roentgen Ray Society. On ARRS.org, you will find information on the 2023 ARRS Annual Meeting in Honolulu, Hawaii, upcoming Live Symposia, Online Courses, Web Lectures, Quick Bytes, and Global Partner Education, including American Journal of Roentgenology (AJR) articles with credit, AJR Webinars, Author Videos, Podcasts, Tweetchats, Visual Abstracts, and much more. Whatever you are looking for, it is very likely that you will find it on the ARRS website and various social media channels.
In our quest to become primary radiologists, a key ingredient is enthusiasm. Coach Wooden noted that enthusiasm “brushes off upon those with whom you come in contact.” He continued, noting that “you must truly enjoy what you are doing.” Being enthusiastic about an unrelenting onslaught of work can be challenging, but we should try to be enthusiastic toward those who really need our services—our patients and our referring providers—and our team members. In general, our teams will function at a higher level if we treat everyone with enthusiastic, professional respect.
In addition to enthusiasm and industriousness, I think that in today’s topsy-turvy world, adaptability is critical. If we are going to be at the top of our game and really be the primary radiologists that we are capable of becoming, we must be able to adapt to new and sometimes unforeseen situations. Coach Wooden defined adaptability as “being able to adjust to any situation at any given time.” Just think of how different October 2019 (pre-COVID) was compared to March 2020 (early in the COVID-19 pandemic). The first COVID-19 outbreak was reported in Wuhan, Hubei, China in November of 2019, and by March 11, 2020, we were involved in a major pandemic with 118,465 confirmed cases of COVID-19 and 4,295 deaths worldwide. As we enter a new academic year, I want to encourage you to be the best radiologist that you can be—to be your best version of a primary radiologist. It won’t be easy, but with industriousness, enthusiasm, and a lot of adaptability, I think that we can do it and enjoy the journey!
Melvin E. Clouse Professor of Radiology, Harvard Medical School Chair, Department of Radiology, Beth Israel Deaconess Medical Center
Lea Azour, MD
Clinical Assistant Professor, Department of Radiology, NYU Grossman School of Medicine Director of Wellness, Department of Radiology
Jonathan Goldin, MD, PhD
Professor of Radiology, Medicine, and Biomedical Physics, UCLA David Geffen School of Medicine Executive Vice Chairman, Department of Radiological Sciences, UCLA David Geffen School of Medicine
The epidemic of stress and burnout among physicians in our imaging field continues unabated, with many commitments, remedies, websites, apps, financial resources, meetings, meals, committees, retreats, articles, and other tactics directed at mitigating the expanding repertoire of undesirable, harmful, and even tragic consequences. The constellation of recognized detractors contributing to our widespread lack of wellness and professional fulfillment continues to grow, and will do so, until an effective and collective strategy is implemented.
Mitigation tactics have been tried—improving practice efficiency amid amassing volumes, personal wellness invocations in times of increased isolation, and efforts to cultivate individual and even practice resilience. Many of these have been Band-Aid attempts to right perceived wrongs, to keep up with current trends, or to respond to newly recognized symptoms. These efforts have had short-term impacts, at best.
One tactic after another. One mole whacked to unearth another. One new personal solution. One new app. And nothing seems to have improved. Our trend lines are heading downwards.
Moving the Wellness Dial?
Most certainly, we have started to move the radiology wellness dial—we have discovered what works and what doesn’t, we have started to recognize the spectrum of manifestations of stress, we have started to explore different personal and practice approaches to wellness, we have started to acknowledge the impact of effective leadership, communities and connections, of having voices heard, of removing the many pebbles from our shoes, and we have started to speak louder and louder about the need for a more organized approach. We have commenced our wellness journey.
There is no better time than now to define where we want to go, how to get there, and how to remove current and future obstacles along the way.
Our efforts have been diverse and well-intended: various manners of resilience-building have been explored, personal wellness strategies were introduced, organizational contributors were recognized, the value of high-functioning teams extolled, as was understanding of the complex preferences of our wonderful multicultural and multigenerational team members. Practices slowly started listening to the voices of their team members. Listening, yet not quite hearing. Conversations slowly started transforming from burnout to wellness, to professional fulfillment, and voices were now being listened to and heard.
Yet the stress and symptoms of emotional exhaustion, detachment, disengagement, and disillusionment persisted, and a great resignation commenced. New challenges emerged, which have become our contemporary opportunities: supporting and sustaining remote teams and flexible work patterns, a staffing challenge like few can recall, rethinking productivity and compensation models, calls for greater transparency, wellness-driving compensation plans and reading environments, and reimagining what a day’s work should look like. The Great Resignation inspired the Great Exploration and Reshuffling, and now the Great Renegotiation—of why and how we work.
So, where does that leave us today? For the past several years, we have responded to the epidemic of burnout by changing the conversation to a more positive focus on wellness, yet our many very well-intended efforts have been largely tactical, rather than strategic.
We have been playing wellness whack-a-mole by responding with tactics to each newly recognized symptom or contributor, rather than thinking strategically.
It’s not too late. As a medical subspecialty, we have the opportunity to change that now, and must. We certainly have the skilled team members, advocates, resources, voices, passions, and energy to do that, and we need to start now. Together, we can and must build a blueprint for wellness that will guide and sustain our efforts towards improved wellness.
This April, please join us in Honolulu, Hawaii for the ARRS Radiology Wellness Summit during the 2023 ARRS Annual Meeting, where all of these will be addressed.
We need to hear your voice; we want to hear your voice.
What Will the ARRS Radiology Wellness Summit in Hawaii Address?
There are moral, ethical, and business imperatives that should drive wellness, and we will explore what strategies are working and which are not. How do we design workflow for wellness, rethink productivity metrics, and explore shift-based comp plans? What does a new day’s work look like for a radiologist? How can one hop off and stay off the hamster wheel that many workplaces have become? What might your AI efficiency wish list look like? What do your wellness numbers and trends reveal? Do you know your current numbers? What are you measuring?
While one might need to measure in order to manage, to quote Albert Einstein, “not all that counts can be counted, and not all that is counted, counts.” Collectively, we have a lot to talk about.
How do we go about stemming the tide of the Great Resignation, or can we, or should we? What are you doing to show appreciation to your faculty who might feel undervalued? What does your peer support program look like? How are you sustaining your talented multigenerational team through different career and life stages? Is your communication strategy effective? How are you introducing appreciative enquiry and positive psychology into your practice? What is your equivalent of a wellness booster clinic, and what are you doing to rediscover the joy and meaning that first led you into radiology? Have you considered coaching, storytelling, micropractices, mindfulness, music, or art? Is your team functioning like Ted Lasso is the coach? How did you train your Chief Wellness Officer and your wellness change agents?
Our inaugural ARRS Radiology Wellness Summit will bring together radiologists across subspecialties and practices to address the many contemporary issues that are top of mind in our postpandemic terrain, with the goal of defining a wellness roadmap that will guide our House of Radiology forward to better navigate the anticipated stormy seas ahead. Together, we plan to transform from a tactic-driven approach to one that is thoughtful, intentional, and strategic. We hope you’ll join us in Honolulu this April for the undertaking. We want your imprint in this timely, necessary, and important effort.
Dr. Barr is a private practice neuroradiologist with Mecklenburg Radiology Associates PA in Charlotte, North Carolina, and incoming President of the American Board of Radiology.
The five years since I joined the Board of Governors has been a period of remarkable change as the American Board of Radiology (ABR) has evolved in response to new requirements and improved stakeholder engagement. The biggest change was the introduction of Online Longitudinal Assessment (OLA) in 2019 to supplant the previous model of recurring high-stakes exams as part of Continuing Certification. The platform has both formative and summative functions and, as a result, satisfies the parts of our social contract as medical professionals that relate to lifelong learning and self-assessment. It positions the ABR as one of the leaders in adopting the American Board of Medical Specialties (ABMS) Standards for Continuing Certification released last November.
In early 2020, recognizing the challenges resulting from the pandemic, we embarked on an aggressive development plan to deliver our Initial Certification exams in a virtual environment. Our early experience with OLA was crucial in guiding the design and implementation of remote exams. In 2021, we successfully administered over 5,000 exams (including both qualifying and certification exams) across all four disciplines (diagnostic radiology, interventional radiology, medical physics, and radiation oncology) and anticipate this will remain an enduring model for Initial Certification.
In addition to the introduction of remote exams and accelerated exam administration, 2021 saw the implementation of a new residency leave policy designed to balance the need for standardization with flexibility to address life events that individuals face during training. We were fortunate to benefit from the vigorous engagement of numerous stakeholders during the development of this policy, including dozens of conversations with trainees and program faculty. Beginning with the 2021–2022 academic year, residents with total time away from residency averaging less than eight weeks (40 workdays) per academic year are eligible for Initial Certification without an extension of training.
Although the programs mentioned above are the most visible to our candidates and diplomates, the behind-the-scenes efforts of our volunteers have been critical in supporting the continuous improvement of our exam content and delivery. We now offer exam candidates increased flexibility in many elements of the qualifying exams, as well as additional dates for the oral exams in medical physics, radiation oncology, and interventional radiology. Several months ago, we embarked on a comprehensive evaluation of the certification exams for diagnostic radiology; as of this writing, external discussions have provided a broad range of perspectives and extremely useful suggestions for potential modifications.
Our executive team and staff have made significant strides in streamlining our administrative processes and improving efficiency, with the goal of mitigating costs. We have reduced redundancy and non-core initiatives and terminated our lease for the Chicago testing center as part of our transition to remote exams. We’ve reduced the cost of some of our products, particularly subspecialty certification exams, and will continue to focus on fee reduction when possible. We are fortunate to maintain healthy capital reserves, which have helped offset investments in technology and software development during the past few years of transition. We continue to maintain our recognition for financial transparency with Platinum Status (per Candid®, formerly GuideStar®).
As I assume the role of ABR president, I look forward to working with our volunteers, staff, and stakeholders to support the ABR’s mission to provide a credential that indicates a high level of professional achievement and commitment to clinical excellence. The ABR Board of Governors, volunteers, and staff remain committed to improving the relevance and value of our exams and programs while avoiding increased costs and unnecessary complication for our candidates and diplomates.
Department of Radiology, Memorial Sloan Kettering Cancer Center
Lars J. Grimm
Department of Radiology, Division of Breast Imaging, Duke University School of Medicine
Jennifer A. Harvey
Department of Imaging Services, University of Rochester Medical Center
Donna M. Plecha
Department of Radiology, University Hospitals Cleveland Medical Center
Emily F. Conant
Department of Radiology, Division of Breast Imaging, Perelman School of Medicine, University of Pennsylvania
Abbreviated breast MRI (AB-MRI) has been shown to maintain the high sensitivity of longer or full breast MRI protocols while decreasing operational costs. The clinical implementation of an AB-MRI program requires collaboration of multiple stakeholders, including administrative, operational, financial, technical, and clinical providers. Institutions must define patient eligibility and imaging protocols and monitor performance metrics to ensure high-quality patient care. The improved efficiency and maintenance of accuracy of AB-MRI may allow more women to access this important supplemental screening modality.
MRI is the most sensitive imaging modality for breast cancer detection [1], and its role as an adjunct to mammographic screening for women at high risk for breast cancer (i.e., a lifetime risk > 20%) is well accepted [2–5]. Although demographic and genetically based risk assessment models are often used to determine breast cancer risk, increased mammographic density increases breast cancer risk and decreases mammographic sensitivity through the obscuration of cancer by adjacent dense breast tissue [6]. Increasing awareness of the impact of increased breast density on patient outcomes has driven the adoption of state and federal legislation mandating that women be notified of their breast density. In response to this increasing awareness, there is growing interest in supplemental screening for breast cancer with breast MRI, which shows improved breast cancer detection for women with dense breasts and otherwise average risk [7]. To accommodate the increasing demand for supplemental breast MRI screening, abbreviated (or fast) breast MRI protocols have been developed that reduce costs, improve workflow, and increase patient access. This article provides details regarding the current literature supporting the utilization of AB-MRI for supplemental screening and the numerous administrative, operational, financial, technical, and clinical elements that must be considered in the implementation of a clinical AB-MRI program.
Review of Abbreviated Breast MRI Outcome Data
The first AB-MRI study, which was published in 2014 by Kuhl et al. [8], included 443 women with a “mildly to moderately increased risk of breast cancer.” The study showed that a 3-minute AB-MRI acquisition that consists of only one unenhanced and one contrast-enhanced sequence has diagnostic accuracy in breast cancer screening that is equivalent to that of a full breast MRI protocol. Multiple studies have since been published, including a prospective multicenter trial [9] and at least three systemic reviews or meta-analyses supporting the use of AB-MRI [10–13] (Table 1).
These studies confirm that the combination of mammography and MRI screening yields the highest cancer detection rate. In addition, cancers detected with MRI are more likely to be invasive and higher grade, compared with cancers detected with mammography [14], and therefore have the potential for greater impact on patient morbidity and mortality.
Because MRI offers improved cancer detection rates and can detect more clinically relevant disease, AB-MRI has been integrated into clinical practice at numerous institutions. Clinical implementation of an AB-MRI program requires consideration of patient eligibility requirements, imaging protocols, and appropriate performance metrics to ensure high-quality patient care.
Patient Selection and Screening Interval
At present, most supplemental screening with AB-MRI is reserved for women with dense breasts, given the superior sensitivity of breast MRI for cancer detection [15]. This recommendation is supported by multiple studies of women with dense breasts, including women who underwent screening with AB-MRI after having negative or benign mammography and ultrasound findings [8], and by a prospective screening study that showed significantly higher rates of invasive breast cancer detection with AB-MRI, compared with digital breast tomosynthesis (DBT) (11.8 vs 4.8 cancers per 1,000 women) [9]. For women with an average risk of breast cancer who have dense breasts and a normal DBT, AB-MRI has shown a breast cancer detection rate of up to 27.4 cancers per 1,000 women [12]. The possible role of AB-MRI in detecting breast cancer in women with nondense breasts who are at intermediate risk for breast cancer has not yet been established.
Although there currently are no data to guide the frequency of AB-MRI screening, given current screening paradigms and the recommendation that high-risk women should undergo annual MRI screening [16], one could consider screening women of average risk who have dense breasts with AB-MRI every 1–2 years [7]. AB-MRI should be performed in addition to an annual mammography examination, and this screening may be performed at the same time as mammography or offset between mammographic screenings.
Imaging Technique
AB-MRI protocols remain institution-dependent; however, consideration should be given to minimizing the total scanning duration and thus the time that the patient spends on the table (i.e., table time). Published AB-MRI acquisition times range from 1.1 to 12 minutes [17, 18], but additional time not related to acquisition must also be allocated to allow the patient to enter and exit the room and to be positioned on the table. The AB-MRI protocol should use parameters similar to those of the full breast MRI protocol, such as magnet field strength, axis of image acquisition, and patient orientation, to facilitate interpretation and comparisons between full and AB-MRI examinations. Postprocessing of sequences, such as subtracted images, maximum-intensity-projection (MIP) images, and multiplanar reconstructions, does not increase actual scanning time and may be performed after the patient has been taken off the table, further improving table-time efficiency.
Published AB-MRI protocol sequences vary greatly but most commonly use an unenhanced T1- and/or T2-weighted sequence, plus one contrast-enhanced sequence [8–11, 19]. A single contrast-enhanced sequence enables generation of subtracted and MIP images but does not provide kinetic information. Despite AB-MRI protocol variation, a systematic review/meta-analysis showed no significant difference in the sensitivity or specificity of AB-MRI versus full breast MRI in studies with 1–2 years of follow-up [12].
Interpretation
The time needed for interpretation of AB-MRI varies depending on the number of protocol sequences [20]. AB-MRI has higher sensitivity than DBT (95% vs 39%) but lower specificity (87% vs 97%) [9]. Improving specificity through minimizing false-positive results should be prioritized when implementing an AB-MRI program.
For interpretation of AB-MRI, it is advised that one first evaluate the MIP image to assess background parenchymal enhancement (BPE) and the symmetry of the breasts and to identify any unique focal findings. AB-MRI interpretation may be more difficult when BPE is moderate or marked [21, 22]. Identification of a unique finding requiring additional evaluation should be based on the morphology of the finding and whether it differs from surrounding or BPE. If available, comparison with prior MIP images will enable determination of whether a finding is new. Correlation with findings on prior mammograms and ultrasounds may also help determine whether the unique finding is benign.
Recognizing benign patterns of BPE may help improve specificity when interpreting screening AB-MRI. Such patterns include multiple scattered foci of enhancement, symmetric regional enhancement, multiple foci with larger enhancing areas, and a picture frame distribution of enhancement along the periphery of the breast [23]. BPE may be asymmetric or, conversely, increased in patients who recently stopped taking antiestrogen medication [24].
Utilization of a T2-weighted sequence in an AB-MRI protocol can assist in the characterization of foci and masses because increased T2 signal intensity, plus a benign morphology, help support a benign diagnosis [25, 26]. T2-hyperintense masses with benign morphologic characteristics, such as round or oval shape, circumscribed margins, dark internal septations, homogeneous enhancement, or a combination of these characteristics, should at most be assessed as a BI-RADS category 3 finding. Inclusion of a T2-weighted sequence in the AB-MRI protocol can decrease BI-RADS category 3 utilization by 37.7% [8]. This is further supported by a retrospective review of T2-hyperintense masses without suspicious features, which had a malignancy rate of 2% [26]. Given that cancers may also show T2 hyperintensity, biopsy should be recommended if a T2-hyperintense finding shows suspicious morphology.
A unique nonmass enhancement (NME) should be biopsied if it is linear, segmental, clumped, heterogeneous, or has clustered ring enhancement (Fig. 1).
Fig. 1—51-year-old with bilateral high-grade ductal carcinoma in situ (DCIS). Axial contrast-enhanced subtracted maximum-intensity-projection image reveals unique, segmental, nonmass enhancement bilaterally (arrows), with pathology from MRI-guided biopsy yielding bilateral high-grade DCIS.
If NME is diffuse or regional with internal homogeneous enhancement with associated T2 fibrocystic changes, it should be considered benign.
Auditing Your Practice
As with auditing any breast MRI practice on the basis of imaging indication (i.e., high-risk screening, diagnostic problem solving, cancer staging), auditing of AB-MRI should be done separately. Performance measures should include, but should not be limited to:
cancer detection rate per 1,000 women;
PPV2 (based on recommendation for tissue diagnosis) and PPV3 (based on results of biopsies actually performed);
outcomes of BI-RADS final assessment categories 0, 3, 4, and 5;
overall sensitivity and specificity.
Complete medical audit data for screening MRI are outlined in BI-RADS 5th edition [27]; however, it is important to note that the benchmarks in BI-RADS 5th edition were based on analyses of prospective, full-protocol screening MRI trials of women with a hereditary predisposition for breast cancer.
In auditing any breast MRI program, BI-RADS category 0 should be used sparingly, reserved for requests of prior imaging that may not have been available at the time of initial interpretation. For example, it may be necessary to correlate MRI findings with those from mammography and/or ultrasound to ensure the stability of MRI findings, such as probable fibroadenomas, lymph nodes, fat necrosis, or a surgical scar. Those MRI findings with benign mammographic or sonographic correlates may be downgraded to BI-RADS category 2 (benign). Careful comparison with prior imaging ultimately helps improves the specificity of MRI and thus patient outcomes.
Although no benchmarks have yet been established for short-term follow-up or the use of BI-RADS category 3 for breast MRI, early outcome data suggest that the limited imaging provided by AB-MRI may increase the rate of short-term follow-up recommendations, compared with full breast MRI protocols [28]. In reporting their first 2 years of experience with AB-MRI, Marshall et al. [28] found that in the first 4 months, their BI-RADS category 3 rate was 14.2%. In an effort to decrease the BI-RADS category 3 rate, they required that all BI-RADS category 3 cases be reviewed by at least two other breast radiologists and that their group would review such cases weekly. After the interventions, the group’s use of BI-RADS category 3 decreased to 8.3% in their first year [28]. As with any breast MRI study, when BI-RADS category 3 is assigned, the next recommendations should clearly be stated in the report.
For cases where an MRI-directed ultrasound is recommended for further evaluation of a mass, the MRI report should provide recommendations for next steps, if a follow-up ultrasound shows no finding. If MRI-directed ultrasound shows a probably benign mass, follow-up of the mass can be performed with ultrasound in 6 months, instead of with MRI. In addition, if follow-up with MRI is recommended, it should be an AB-MRI, not a full-protocol examination, to maintain operational costs and facilitate comparison across similar protocols. A final assessment of BI-RADS category 3 should never be used for an enlarging or new solid mass. Benchmarks are well established for outcomes for BI-RADS categories 4 and 5, as well as for PPV2 and PPV3 [29]. Access to the audit data of each individual reader, as well as to the combined data of the group, is essential, so radiologists can compare their outcomes to those of others and seek additional training as needed.
As expected, there is a learning curve to the interpretation of any new imaging modality or protocol. Auditing allows the identification of outliers among a group of radiologists and may help target individuals for additional training. As with any new imaging modality, a practice may also consider limiting the number of radiologists reading AB-MRI cases early in the implementation, later expanding the number of readers as the volume of examinations increases and a teaching set of images with known outcomes has been collected for sharing across the group. Furthermore, as outcome data from AB-MR studies continue to evolve, benchmarks will be established for best practices.
Financial Considerations
Because there currently is no Current Procedural Terminology (CPT) code for AB-MRI, women must self-pay for their examinations without insurance being billed [15]. According to recent reviews of AB-MRI implementation at sites across the United States, out-of-pocket charges vary from $250 [28] to $500 [30]. When appropriate pricing is considered, the cost of the gadolinium-based contrast agent and table time must be considered [31], as must the costs of any downstream MRI-guided biopsies that may or may not be covered by the patient’s insurance. It should be noted that the out-of-pocket payment may be a barrier for some patients, leading to disparities in access to AB-MRI screening. In a recent survey of 508 patients with dense breasts who were undergoing screening mammography, 67% of patients cited the cost of adjunct screening as the primary deterrent [32], which was independently associated with younger age [33]. A possible solution could include adjustment of the self-payment costs based on financial need.
To determine appropriate pricing based on cost benefit, Mango et al. [34] used a Monte Carlo simulation to analyze a 30-year screening period in which a hypothetical group of 2.5 million women would undergo either digital mammography annually or MRI every 3 years (selected on the basis of no interval cancers being identified during this time frame in another study [35]). At 24 years, MRI became as cost-effective as mammography ($13.02 billion vs $13.03 billion, respectively). When a lower cost of $400 was used for MRI (vs $640 for the full diagnostic protocol), MRI screening became more cost-effective in less than 6 years ($3.41 billion vs $3.65 billion for mammography). However, the comparison of AB-MRI with 2D mammography rather than DBT limits generalizability [34].
Bundled payment models, which include all costs from screening to breast cancer diagnosis over a 364-day period, have been created to control costs and increase value. If AB-MRI reduces overall costs for breast cancer screening (as a triennial examination performed without mammography), compared with digital mammography by 6 years, as suggested by the Monte Carlo simulation [34], bundled payments may be reasonable for incident AB-MRI screening at the cost of $400 per study. The societal costs of screening once every 3 years must also be considered.
With no current insurance coverage for AB-MRI, institutions must engage multiple stakeholders when initiating an AB-MRI program. Certainly, the downstream revenues to the institution from breast cancers detected using AB-MRI are an important consideration. Institutional financial support may be needed, with expectations of downstream revenues.
Implementation of Abbreviated (or Fast) MRI in Your Clinical Practice
A clear protocol that defines which patients should be offered AB-MRI is needed, especially in the early phase of implementation. Additionally, because triage of patients will be needed to ensure appropriateness, it may be prudent to limit the number of schedulers involved in booking AB-MRI examinations, until a smooth process is developed. A telephone script for schedulers can help to ensure that appropriate eligibility is determined before scheduling [7].
Preferably, AB-MRI examinations should be scheduled in time slots that are significantly shorter than the time slots needed for full-protocol breast MRI, which takes longer to perform. To increase operational efficiency for an abbreviated protocol, it will be important to work with MRI technologists to limit the time that patients are positioned on the table to match the abbreviated protocol. For example, it will be important to emphasize that for the greatest efficiency, the processing of reconstructed images (subtracted and MIP images) by technologists should be done after the patient has been removed from the MRI table and imaging room. AB-MRI examinations can also be scheduled sequentially to reduce the time needed to set up and take down the breast coil. This attention to efficient use of the room and table time will optimize operations and allow more rapid turnover of the room for the next patient study, resulting in less downtime for room use [31].
To start a successful program of supplemental AB-MRI screening, it is essential to engage referring health care providers with educational programs that address who may be appropriate for supplemental AB-MRI screening and what the implications of additional screening may be for patients. One of the best methods of educating both patients and providers is lecturing at patient-facing symposia or departmental grand rounds to discuss the implications of increased breast density on both the masking of cancers on mammography and the risk of breast cancer developing. Also, it is helpful to create informational cards on supplemental screening with AB-MRI that can be provided to appropriate patients in either the breast imaging or primary care clinics [7]. As uptake of the new protocol increases and significant results, such as supplemental cancer detection rates and subtypes of cancers detected, become available, follow-up educational sessions should be provided to referring providers and, if possible, consumers.
Future Directions
The imaging sequences for breast MRI protocols, including AB-MRI protocols, are constantly evolving. For example, given the limited temporal information regarding many AB-MRI protocols, several exploratory efforts have included ultrafast sequences [36–39], which may have lower spatial resolution but may include images acquired every 1–10 seconds during the first two minutes after injection of contrast medium. Therefore, while maintaining an abbreviated protocol, measurements of both maximum slope of enhancement and rate of enhancement are possible to help discriminate benign from malignant lesions [39, 40]. There have also been efforts to develop unenhanced abbreviated breast MRI protocols because screening MRI could potentially be performed routinely over many years and because there have been concerns surrounding cumulative deposition of gadolinium [41]. A recent study by Bickelhaupt et al. [42] showed that the performance of unenhanced DWI and AB-MRI was comparable (sensitivity, 0.92 vs 0.85, respectively; specificity, 0.94 vs 0.90, respectively). Although acquisition of DWI is time-consuming, the possibility of DWI replacing contrast imaging is appealing, if performance is maintained [42]. However, according to a recent study that included both DWI and contrast imaging, inclusion of DWI in the abbreviated protocol achieved performance comparable to that of a full protocol (sensitivity, 100% vs 100%, respectively; specificity, 95.0% vs 96.8%, respectively); however, scanning time was extended, and contrast medium was still used [43]. Ideally, DWI will advance so that performance of an abbreviated DWI protocol will rival that of an abbreviated contrast study.
AB-MRI may improve access to high-sensitivity screening breast MRI and decrease overall cost. Successful clinical implementation requires the thoughtful collaboration of multiple stakeholders and ongoing monitoring of performance metrics. Additional data and experience are required to facilitate standardization across institutions. With improved efficiency and maintained accuracy, AB-MRI may enable more women to access this important supplemental screening modality.
A multimodality review—everything from routine ultrasound and mammography to the latest DBT and AI applications—ARRS’ Breast Tumor Imaging Online Course delivers the interpretive, technical, and systems knowledge that practicing radiologists need to provide quality breast cancer screening. Additional lectures address pathology, the BI-RADS lexicon, and even the history and economics of breast cancer, all critical for improving overall care disparities and patient outcomes.
DeMartini W, Lehman C. A review of current evidence-based clinical applications for breast magnetic resonance imaging. Top Magn Reson Imaging 2008; 19:143–150
Sardanelli F, Boetes C, Borisch B, et al. Magnetic resonance imaging of the breast: recommendations from the EUSOMA working group. Eur J Cancer 2010; 46:1296–1316
Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007; 57:75–89
Lee CH, Dershaw DD, Kopans D, et al. Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultra- sound, and other technologies for the detection of clinically occult breast cancer. J Am Coll Radiol 2010; 7:18–27
Mann RM, Balleyguier C, Baltzer PA, et al. Breast MRI: EUSOBI recommendations for women’s information. Eur Radiol 2015; 25:3669–3678
Saftlas AF, Hoover RN, Brinton LA, et al. Mammographic densities and risk of breast cancer. Cancer 1991; 67:2833–2838
Grimm LJ, Mango VL, Harvey JA, Plecha DM, Conant EF. Implementation of abbreviated breast MRI for screening: AJR expert panel narrative review. AJR 2021 Aug 11 [published online]
Kuhl CK, Schrading S, Strobel K, Schild HH, Hilgers RD, Bieling HB. Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection—a novel approach to breast cancer screening with MRI. J Clin Oncol 2014; 32:2304–2310
Comstock CE, Gatsonis C, Newstead GM, et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening. JAMA 2020; 323:746–756
Baxter GC, Selamoglu A, Mackay JW, Bond S, Gray E, Gilbert FJ. A meta-analysis comparing the diagnostic performance of abbreviated MRI and a full diagnostic protocol in breast cancer. Clin Radiol 2021; 76:154
Hernández ML, Osorio S, Florez K, Ospino A, Diaz GM. Abbreviated magnetic resonance imaging in breast cancer: a systematic review of literature. Eur J Radiol Open 2020; 8:100307
Geach R, Jones LI, Harding SA, et al. The potential utility of abbreviated breast MRI (FAST MRI) as a tool for breast cancer screening: a systematic review and meta-analysis. Clin Radiol 2021; 76:154.e11–154.e22
Weinstein SP, Korhonen K, Cirelli C, et al. Abbreviated breast magnetic resonance imaging for supplemental screening of women with dense breasts and average risk. J Clin Oncol 2020; 38:3874–3882
Sung JS, Stamler S, Brooks J, et al. Breast cancers detected at screening MR imaging and mammography in patients at high risk: method of detection reflects tumor histopathologic results. Radiology 2016; 280:716–722
Marshall H, Pham R, Sieck L, Plecha D. Implementing abbreviated MRI screening into a breast imaging practice. AJR 2019; 213:234–237
Monticciolo DL, Newell MS, Moy L, Niell B, Monsees B, Sickles EA. Breast cancer screening in women at higher-than-average risk: recommendations from the ACR. J Am Coll Radiol 2018; 15:408–414
Mori N, Sheth D, Abe H. Nonmass enhancement breast lesions: diagnostic performance of kinetic assessment on ultrafast and standard dynamic contrast-enhanced MRI in comparison with morphologic evaluation. AJR 2020; 215:511–518
Heacock L, Melsaether AN, Heller SL, et al. Evaluation of a known breast cancer using an abbreviated breast MRI protocol: correlation of imaging characteristics and pathology with lesion detection and conspicuity. Eur J Radiol 2016; 85:815–823
Heacock L, Lewin AA, Toth HK, Moy L, Reig B. Abbreviated MR imaging for breast cancer. Radiol Clin North Am 2021; 59:99–111
Harvey SC, Di Carlo PA, Lee B, Obadina E, Sippo D, Mullen L. An abbreviated protocol for high-risk screening breast MRI saves time and resources. J Am Coll Radiol 2016; 13:R74–R80
DeMartini WB, Liu F, Peacock S, Eby PR, Gutierrez RL, Lehman CD. Background parenchymal enhancement on breast MRI: impact on diagnostic performance. AJR 2012; 198:[web]W373–W380
Ray KM, Kerlikowske K, Lobach IV, et al. Effect of background parenchymal enhancement on breast MR imaging interpretive performance in community-based practices. Radiology 2018; 286:822–829
Giess CS, Yeh ED, Raza S, Birdwell RL. Background parenchymal enhancement at breast MR imaging: normal patterns, diagnostic challenges, and potential for false-positive and false-negative interpretation. RadioGraphics 2014; 34:234–247
Li J, Dershaw DD, Lee CH, Joo S, Morris EA. Breast MRI after conservation therapy: usual findings in routine follow-up examinations. AJR 2010; 195:799–807 [Erratum in AJR 2010; 195:1043]
Ha R, Sung J, Lee C, Comstock C, Wynn R, Morris E. Characteristics and outcome of enhancing foci followed on breast MRI with management implications. Clin Radiol 2014; 69:715–720
Grimm LJ, Enslow M, Ghate SV. Solitary, well-circumscribed, T2 hyperintense masses on MRI have very low malignancy rates. J Breast Imaging 2019; 1:37–42
Ikeda DM, Hylton NM, Kuhl CK, et al. BI-RADS: magnetic resonance imaging, 1st ed. In: D’Orsi CJ, Mendelson EB, Ikeda DM, et al. Breast Imaging Reporting and Data System: ACR BI-RADS—breast imaging atlas. Reston, VA: American College of Radiology, 2003
Marshall HN, Plecha DM. Setting up an abbreviated breast MRI program: our two-year implementation experience. J Breast Imaging 2020; 2:603–608
Lee JM, Ichikawa L, Valencia E, et al. Performance benchmarks for screening breast MR imaging in community practice. Radiology 2017; 285:44–52
Berg WA, Rafferty EA, Friedewald SM, Hruska CB, Rahbar H. Screening algorithms in dense breasts: AJR expert panel narrative review. AJR 2021; 216:275–294
Borthakur A, Weinstein SP, Schnall MD, Conant EF. Comparison of study activity times for “full” versus “fast MRI” for breast cancer screening. J Am Coll Radiol 2019; 16:1046–1051
Miller MM, Repich K, Patrie JT, Anderson RT, Harvey JA. Preferences and attitudes regarding adjunct breast cancer screening among patients with dense breasts. J Breast Imaging 2021; 2:119–124
Miller MM, Repich K, Patrie JT, Anderson RT, Har- vey JA. Patient characteristics associated with patient-reported deterrents to adjunct breast cancer screening among patients with dense breasts. AJR 2021;217: 1069–1079
Mango VL, Goel A, Mema E, Kwak E, Ha R. Breast MRI screening for average-risk women: a Monte Carlo simulation cost-benefit analysis. J Magn Reson Imaging 2019; 49:e216–e221
Kuhl CK, Strobel K, Bieling H, Leutner C, Schild HH, Schrading S. Supplemental breast MR imaging screening of women with average risk of breast cancer. Radiology 2017; 283:361–370
van Zelst JCM, Vreemann S, Witt HJ, et al. Multireader study on the diagnostic accuracy of ultra- fast breast magnetic resonance imaging for breast cancer screening. Invest Radiol 2018; 53:579–586
Goto M, Sakai K, Yokota H, et al. Diagnostic performance of initial enhancement analysis using ultra- fast dynamic contrast-enhanced MRI for breast lesions. Eur Radiol 2019; 29:1164–1174
Milon A, Vande Perre S, Poujol J, et al. Abbreviated breast MRI combining FAST protocol and high temporal resolution (HTR) dynamic contrast enhanced (DCE) sequence. Eur J Radiol 2019; 117:199–208
Mann RM, Mus RD, van Zelst J, Geppert C, Karssemeijer N, Platel B. A novel approach to contrast- enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest Radiol 2014; 49:579–585
Abe H, Mori N, Tsuchiya K, et al. Kinetic analysis of benign and malignant breast lesions with ultrafast dynamic contrast-enhanced MRI: comparison with standard kinetic assessment. AJR 2016; 207:1159– 1166
Runge VM. Critical questions regarding gadolinium deposition in the brain and body after injections of the gadolinium-based contrast agents, safety, and clinical recommendations in consideration of the EMA’s Pharmacovigilance and Risk Assessment Committee recommendation for suspension of the marketing authorizations for 4 linear agents. Invest Radiol 2017; 52:317–323
Bickelhaupt S, Laun FB, Tesdorff J, et al. Fast and noninvasive characterization of suspicious lesions detected at breast cancer x-ray screening: capability of diffusion-weighted MR imaging with MIPs. Radiology 2016; 278:689–697
Chen SQ, Huang M, Shen YY, Liu CL, Xu CX. Abbreviated MRI protocols for detecting breast cancer in women with dense breasts. Korean J Radiol 2017; 18:470–475