Recognizing this hallmark pattern can spare unnecessary confusion, guiding the right surgical call.
The Big Picture
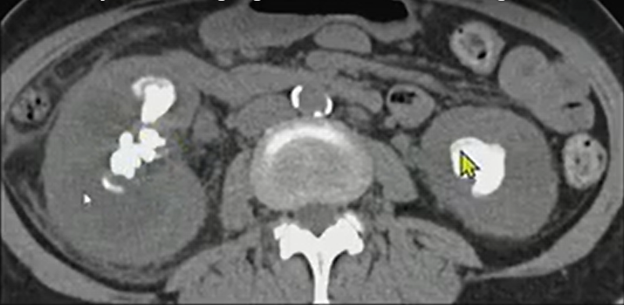
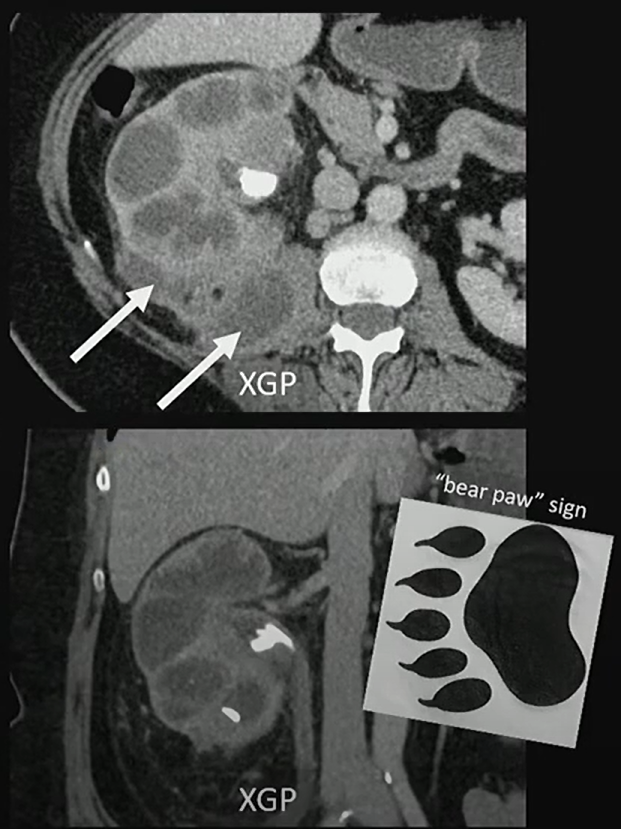
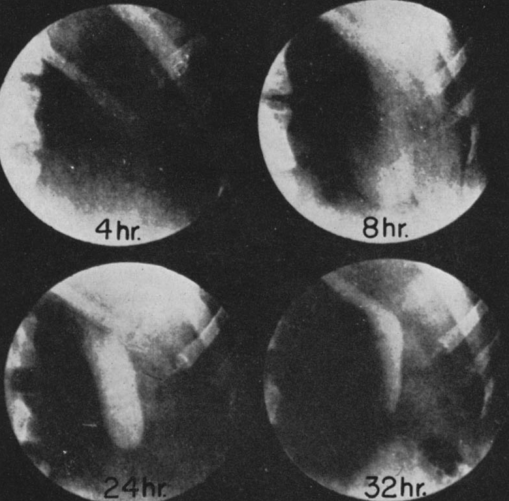
Xanthogranulomatous pyelonephritis (XGP) is a rare, destructive renal infection, most often in women with staghorn calculi. It replaces functioning parenchyma with lipid-laden macrophages and inflammatory tissue, often extending beyond the kidney.
Nine months later, we see much more exuberant inflammation—soft-tissue thickening extending out from the kidney into the retroperitoneum.
Patient underwent renal scintigraphy prior to getting a nephrectomy, and we can see that that right kidney is not contributing to the renal function.
Key Takeaways
Classic appearance: Enlarged kidney, staghorn calculi, and a contracted pelvis—the “bear paw.”
Functional loss: Renal scintigraphy often shows little or no contribution from the affected kidney . . .
Parameter
Left Kidney
Right Kidney
Peak Time
6.7 minutes
2.3 minutes
Relative Function (Integral, 1–3 min)
85%
15%
Extrarenal extension: Look for inflammation tracking into the retroperitoneum, psoas, or paraspinal muscles.
Definitive treatment: Because the kidney is typically nonfunctional, nephrectomy is the standard.
Challenges Ahead
Distinguishing XGP from renal cell carcinoma or pyonephrosis can be difficult without correlating imaging and functional data.
Awareness of extrarenal spread is crucial to surgical planning.
Early recognition can prevent unnecessary biopsy or delay in definitive management.
Presented by Anup Shetty, MD, during ‘Radiology Case Review: Genitourinary Imaging,’ part of the ARRS 2025 Annual Meeting. Watch the full session now: arrs.org/am25
Bottom Line
When you see that “bear paw” (i.e., staghorn calculus, perinephric inflammation, and an enlarged, poorly functioning kidney), think XGP!
For radiologists especially, artificial intelligence (AI) is no longer just over the horizon; it’s in the reading room, right now. This practical immediacy is precisely the premise behind the 2026 ARRS Annual Meeting Categorical Course, Clinical Artificial Intelligence in Radiology. Presented live and virtually from the David L. Lawrence Convention Center in Pittsburgh, PA, this two-day ARRS Categorical Course continues our 125-year-old legacy of forward-looking education by arming radiologists with a robust understanding of how AI is reshaping the specialty.
Dr. Shandong Wu | Cat Course Codirector
Clinical Artificial Intelligence in Radiology brings together more than 20 distinguished faculty from leading institutions across the globe, all led by Shandong Wu, PhD, founding director of the University of Pittsburgh’s Center for AI Innovation in Medical Imaging, a cross-campus initiative including more than 130 researcher and clinician members. Also a professor of radiology, biomedical informatics, bioengineering, intelligent systems, clinical and translational science, one of Dr. Wu’s ARRS Cat Course codirectors is an abdominal radiologist and director of diagnostic AI at the University of Washington, Yee Seng Ng, MD.
Dr. Shandong Wu | Cat Course Codirector
Alongside codirector and 2024 AJR Lee F. Rogers International Fellow in Radiology Journalism Hyun Soo Ko, MD (Peter MacCallum Cancer Centre, Australia), the trio is curating a curriculum of more than two dozen lectures and panels across seven thematic sections, giving registrants a comprehensive view of AI’s current and future roles in everyday practice.
SUN, APRIL 12—From Concept to Clinic: Building AI Literacy
Day one of Clinical Artificial Intelligence in Radiology kicks off with “Getting to Know AI,” a primer tailored for all levels of experience. Tessa Cook, MD, PhD (University of Pennsylvania), provides an overview of radiological progress in AI, while Dr. Ko demystifies essential concepts, such as machine learning, deep learning, radiomics, as well as generative and agentic AI.
Dr. Linda Moy | Vice Chair of AI, NYU Radiology
Up next, inaugural vice chair of AI at New York University’s radiology department, Linda Moy, MD, will provide an invaluable look into leveraging AI to improve workflow efficacy and effectiveness alike. Dr. Wu himself closes the Cat Course’s first session. The leader of Pittsburgh’s Intelligent Computing for Clinical Imaging lab will explore and explain how AI is enhancing imaging interpretation for computational insights—from screening and triage to diagnosis and prediction.
Clinical Implementation: From Regulation to Real-World Deployment
Section two of Clinical Artificial Intelligence in Radiology, “AI Clinical Implementation,” addresses legal, regulatory, and operational frameworks essential for radiologists seeking to implement or evaluate AI tools in practice. Didactic highlights will include guidance on U.S. Food and Drug Administration (FDA) regulations and performance monitoring by Melissa Davis, MD, MBA (Yale), as well as insights into distinguishing high-quality AI models from market hype.
In a uniquely insightful presentation, Julian Rivera, JD (University of Pittsburgh), will tackle the legion of legal considerations accompanying AI adoption: liabilities, ethical perspectives on signing contracts, collaborative business modes with AI companies, etc. Dr. Cook returns to share her expertise on evaluating local versus commercial solutions when measuring ROI, while a panel moderated by Dr. Moy will outline best practices and common pitfalls.
Beyond the Pixel: Multimodality and Multidimensional AI
The promise of any good AI expands significantly when paired with non-image data. The “Going Beyond Images to Multimodality” session explores emerging applications that leverage large language models, vision-language models, and foundation models. Presenters Heather Whitney, PhD (University of Chicago), and Lifeng Yu, PhD (Mayo Clinic), will delve into data curation, federated learning, and the physics of AI model performance. With Christian Bluethgen, MD (University Hospital of Zurich), having assessed multimodal data methodologies in his presentation, a panel discussion on tackling technical challenges to find opportunities rounds out day one of this ARRS Cat Course.
MON, APRIL 13—Practical Impact Across Subspecialties
AI’s reach across subspecialties is the focus on Monday. Presenters including Constance Lehman, MD, PhD (Harvard), Ali Guermazi, MD, PhD (Boston University), and 2022 ARRS Gold Medalist Edward Y. Lee, MD, MPH (Harvard) will detail AI tools in breast, musculoskeletal, pediatric imaging, respectively. Dr. Ng’s highly anticipated survey of AI and abdominal imaging will be followed by a lecture from neuroradiologist Paulo De Aguiar Kuriki, MD (UT Southwestern).
Dr. Edward Y. Lee | ARRS Gold Medalist
That’s not all either. Real-world cardiothoracic, interventional, and nuclear medicine cases will further demonstrate how AI is already reflowing imaging workloads, improving diagnostic accuracy, and personalizing care across organ systems and patient populations.
Shaping Tomorrow: Research, Education, and Ethical Engagement
Day two of Clinical Artificial Intelligence in Radiology continues with “AI Research and Education,” including a model development demonstration by Dooman Arefan, PhD (University of Pittsburgh), and an exploration of MD–PhD collaboration opportunities from Dr. Wu. Justin Peacock, MD, PhD (Uniformed Services University), will discuss educational roadmaps and training resources, addressing a key concern for attendees seeking to build or deepen their AI competencies.
This 2026 ARRS Annual Meeting Categorial Course concludes with “Humanity and AI,” a thought-provoking session covering radiologist–AI collaboration, fairness and bias, and imaging’s ever-evolving role in AI-powered services. Florence Doo, MD (University of Maryland) will help us find a foothold in our present human–AI ecosystem, followed by a warning for all the disparities AI run amok could actually exacerbate care of Judy Gichoya, MD, MS (Emory). Eduardo Mortani-Barbosa, MD, MBA (University of Pennsylvania), will then detail specific skill sets that AI-forward radiologists will need to hone in their practices and in their communities. Finally, ARRS Scholar and Gold Medalist and editor of Radiology: Artificial Intelligence Charles E. Kahn, MD (University of Pennsylvania), joins to facilitate a panel discussion on action items and what to do next.
Dr. Charles E. Kahn | Editor, Radiology: Artificial Intelligence
With each live lecture accompanied by an e-book chapter, Clinical Artificial Intelligence in Radiology will provide strategic context and tactical guidance for imagers of each practice type and at every level of training.
And as Dr. Wu tells InPractice, “AI in radiology is not just a technical shift—it’s a cultural one. This ARRS Categorical Course is about empowering radiologists to shape that future, not just react to it.”
With content spanning conceptual foundations to the most practical of pearls, the curriculum curated by Wu, Ng, Ko and colleagues this April is poised to be an essential learning experience for working radiologists looking to engage with AI at the frontlines of medical imaging care.
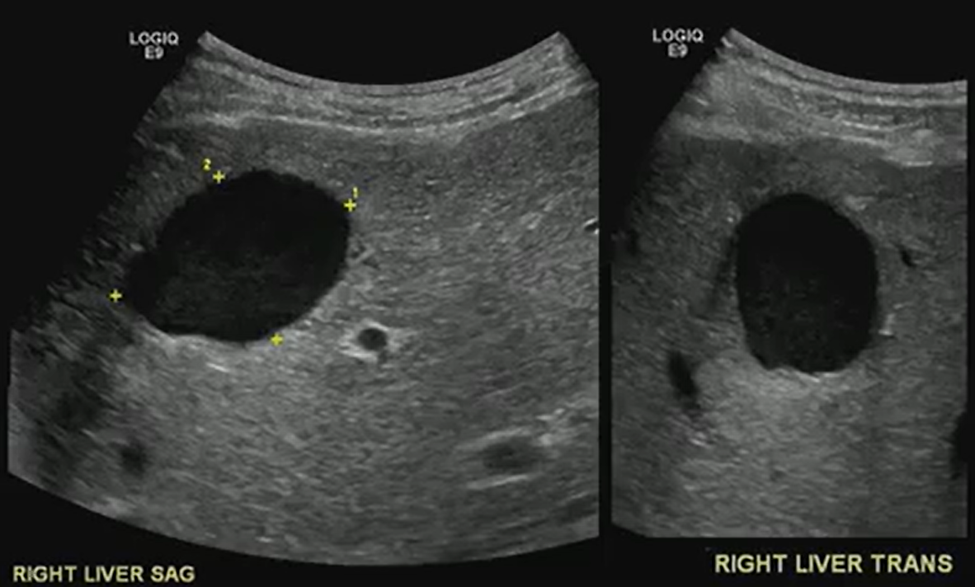
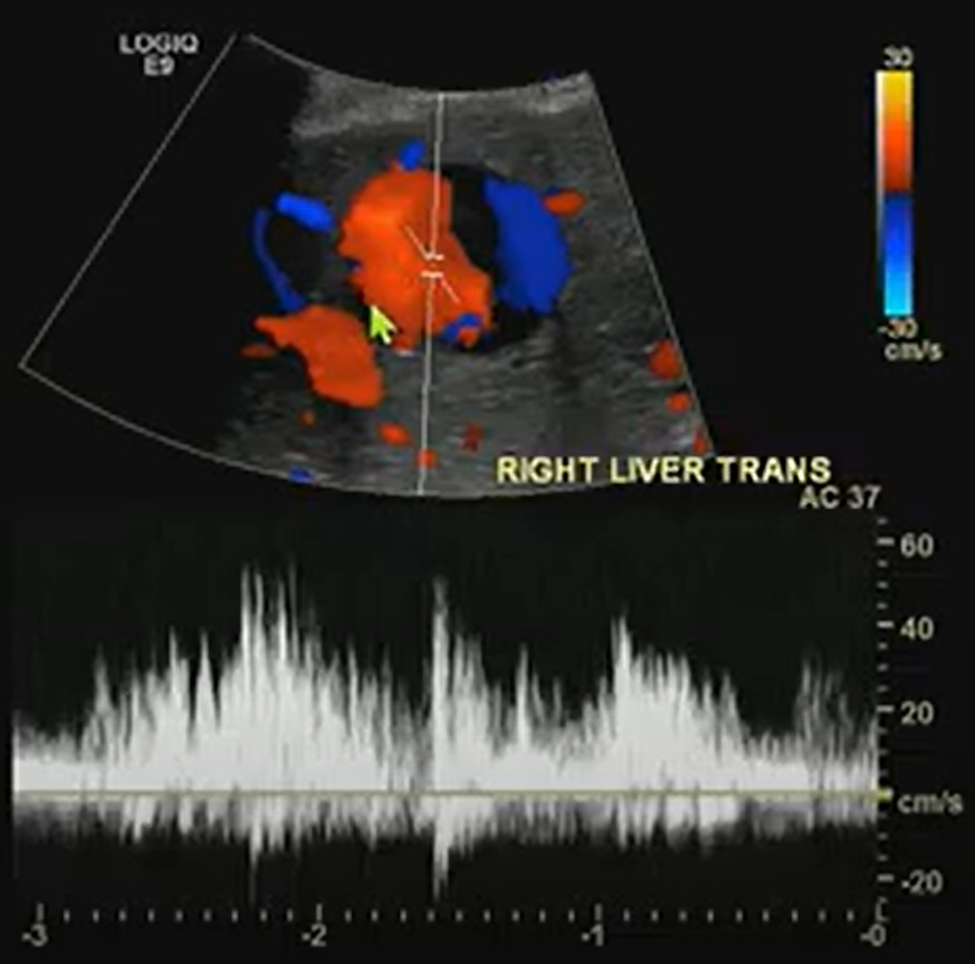
A benign-looking liver lesion turned out to be a hepatic artery pseudoaneurysm—all thanks to color Doppler.
The Big Picture
What looks like a simple hypoechoic cyst on ultrasound may hide a critical vascular pathology. In this ARRS Annual Meeting case from Kristin Rebik, DO, color Doppler proved essential for distinguishing cystic lesions from vascular anomalies like pseudoaneurysms.
Key Takeaways
Always Doppler: Even cyst-like structures require Doppler evaluation to rule out vascular causes.
Pepsi Sign: Swirling vascular flow within a lesion may signal a pseudoaneurysm.
High stakes: Hepatic artery pseudoaneurysms can mimic benign lesions but require urgent recognition and intervention.
Next steps: Interventional radiology embolization can be lifesaving.
Challenges Ahead
Differentiating pseudoaneurysms from other vascular or cystic lesions remains tricky.
Missing Doppler evaluation risks misdiagnosis and delayed treatment.
Awareness of teaching signs like the “Pepsi sign” is uneven among trainees.
Bottom Line
Never skip Doppler. The “Pepsi sign” may be the clue that transforms a benign-looking lesion into a critical vascular diagnosis.
Deborah A. Baumgarten, MD, MPH 2025-2026 ARRS President
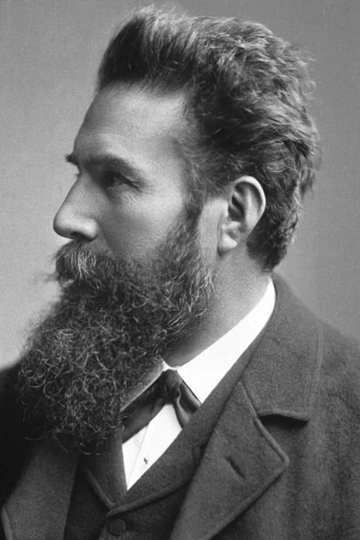
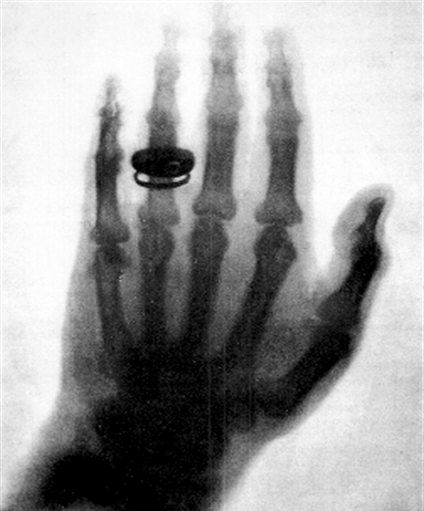
There’s no discussion about serendipity without mentioning the namesake of our society, Wilhelm Conrad Roentgen. I’m sure we all also recognize the world’s first radiograph on the right, taken on November 8, 1895. It’s an image of his wife Anna Bertha’s hand only a couple of weeks after Roentgen discovered what he termed “x-rays”—x for something unknown. Roentgen was studying cathode rays in his lab in a dark room, and he noted a glow several feet away from where he was standing. Although he was not the first to note that cathode rays could permeate thin metal sheets or light up a fluorescent screen near them, he was the first to put those pieces together. And for that, he won the first Nobel Prize in physics in 1901.
Wilhelm Roentgen (1845-1923) and the left hand of his wife, Anna Bertha Ludwig Roentgen, in 1895
I love this quotation attributed to Albert Szent-Györgyi, a Hungarian biochemist, who, among other things, aptly won a Nobel Prize in 1937 for the isolation of vitamin C: “Discovery consists of seeing what everyone else has seen and thinking what no one else has thought.” Many have called the discovery of x-rays serendipity—defined by the Oxford Dictionary as the occurrence in development of events by chance, in a happy or beneficial way, and by Merriam-Webster as a faculty or phenomenon of finding valuable or agreeable things not sought for. The term was first used in 1754 by Horace Walpole, the fourth Earl of Orford, who is remembered for a silly fairytale about three princes from the country of Serendip. Due to a series of accidents and keen mental judgment, these princes were able to discern the nature of a lost camel, of all things. But there’s another factor that lets serendipity thrive: keeping an open mind. There are many other points in the history of science and radiology where serendipity and open-mindedness played a role, and we’ll look at a few of those stories here in InPractice.
John McIntyre (1857-1928)
This is Dr. John McIntyre of Glasgow, Scotland. Although not a radiologist, he was actually the first person to in the world to set up an x-ray department in March of 1896, after lecturing on “The New Light: X-rays” a mere month after their discovery. The serendipity in his story is the chance intersection of electricity and medicine. An apprentice electrician before studying medicine, Dr. McIntyre was fascinated by the potential uses of electricity in medicine. He was named consulting medical electrician at the Glasgow Royal Infirmary in 1895, and although mainly interested in diseases of the ears, nose, and throat, Dr. McIntyre was the first to image a renal stone in vivo in April of 1896. He was also the first to show movement of a frog’s leg using cineradiography, later a beating heart, and then a bismuth meal in the stomach.
But even before the word serendipity made it into the English vernacular, the notion of serendipity existed. “The greatest part of the invention being, but a luckey bitt of chance [sic]” is attributed to English polymath Robert Hook in 1679. A man of many talents, he is credited for being the first to describe cells under a microscope. In fact, Hook designed his own compound microscope and coined the term cell. He also described the force applied to a spring and its deformation, what’s known as Hook’s law of elasticity.
Earl Osborne (1895-1960)
Our next story nicely illustrates Robert Hook’s thoughts about invention and chance. This is Dr. Earl Osborne, who was a dermatology resident at the Mayo Clinic. Dr. Osborne, along with physician and pharmacologist Leonard Rowntree, is credited with discovering that intravenous administration of sodium iodine salts for treating syphilis faintly opacified the urinary tract. Dr. Osborne is said to have serendipitously noted the opacification of the bladder in one of his patients who had an abdominal roentgenogram during treatment. When asked about this discovery, he stated, “it occurred to one of us that if in roentgenology of the urinary tract advantage could be taken of the fact that sodium iodine, after its introduction into the body is normally excreted in the urine, roentgenograms of the kidneys, ureters, and bladder might be secured without the need for catheterization.” Anybody recognize the term KUB in this statement?
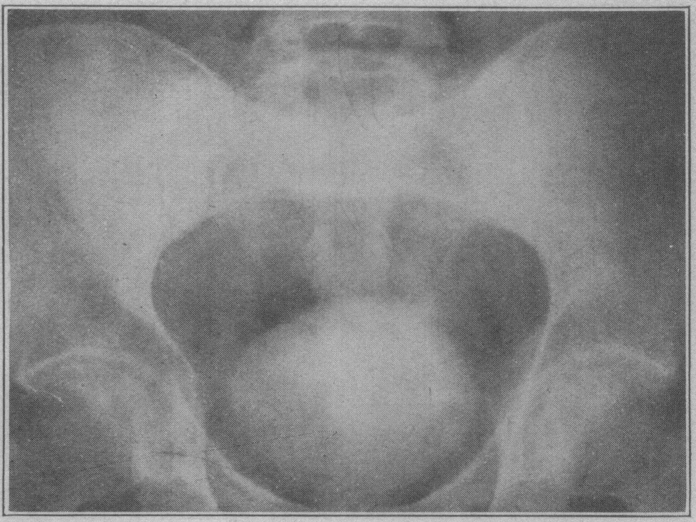
Initial investigations of sodium iodide also included a radiologist named Charles Sutherland and a urologist named Albert Scholl and were published in JAMA in February of 1923. The image on the left is from that paper, taken two hours after the administration of 200 cc of a 20% solution of sodium iodine showing opacification of the bladder. The roentgenogram on the right was taken about an hour after the administration of 100 cc of a 10% solution. You can see that the bladder is opacified, and there’s faint opacification of the kidneys, spleen, and liver. Ironically, neither Dr. Osborne nor Dr. Rowntree pursued this any further, but Dr. Osborne did go on to help found the American Board of Dermatology.
Abdominal roentgenograms with bladder—as well as kidney, spleen, and liver—opacities
Dr. Donald Cameron, a young Minnesota surgeon, is seemingly forgotten in all of the fuss about Drs. Rowntree and Osborne. He published a preliminary report about the oral and intravenous administration of sodium iodine as an opaque medium in roentgenology in JAMA in 1918, five years before Sutherland’s paper came out. Cameron published this preliminary report in case he didn’t return from World War I. He published one more article a few months later, but then never pursued this line of research any further. But he did return from WWI and established a hospital in the Midwest now called the Cameron Memorial Community Hospital that still exists today.
Like the discovery that sodium iodine opacifies the urinary tract, the origins of oral cholecystography are serendipitous, too. As the story goes, Dr. Warren Cole was working in a lab experimenting with compounds that were known to be excreted by the liver into bile. Four and a half months went by before he even ever saw a gallbladder image, until one day this image was obtained in one of the lab dogs.
Oral cholecystogram in canineOral cholecystogram in human
A new Harvey L. Neiman Health Policy Institute study, published in the American Journal of Roentgenology (AJR), investigated whether office-based providers are more likely to refer imaging to a radiologist, or to self-refer and interpret the ordered imaging studies themselves. “Self-Interpretation of Imaging Studies by Ordering Providers: Frequency and Associated Provider and Practice Characteristics” found that 43.6% of office-based studies were interpreted by the ordering provider, while 58.5% were interpreted within the ordering provider’s practice. Additionally, rates of self-interpretation varied by the specialty of the ordering provider and the imaging modality.
Self-Read Rates Vary by Modality and Specialty
Based on more than 1.6 million office-based imaging claims for Medicare fee-for-service beneficiaries in 2022 that were ordered by non-radiologists, by modality and across all specialties, this AJR Original Research manuscript by Christensen et al. found that the self-interpretation rate for office-based imaging was as follows:
50.4% for radiography and fluoroscopy
52.0% for ultrasound
39.5% for nuclear medicine
5.3% for CT
6.1% for MR
Meanwhile, self-interpretation by specialty broke down accordingly:
19.9% for primary care physicians
75.7% for orthopedic/sports medicine physicians
30.5% for non-physician practitioners
Another key determinant of self-interpretation rates was the size of the practice. Rates of self-interpretation were substantially less in the largest practices (500 or more providers) than the smallest practices (only 1-9 providers): 24.2% versus 48.9%, respectively, according to the researchers’ findings.
Access to Radiologists Could Curb Self-Reading
Eric W. Christensen, PhD
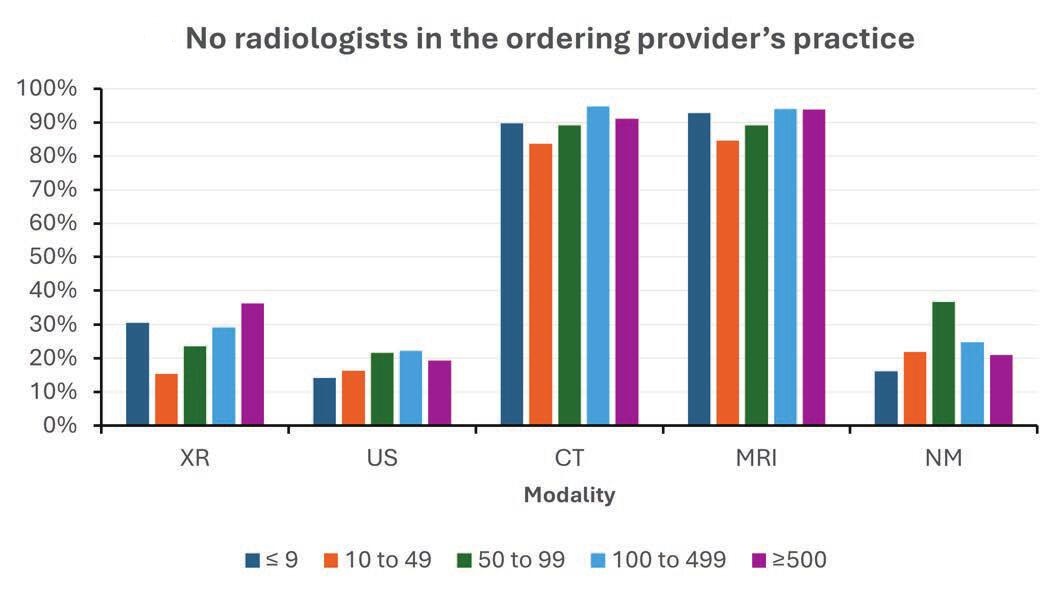
Whether or not there was a radiologist in the ordering provider’s practice was highly correlated with self-interpretation of imaging by the ordering provider (Fig. 1). “If there was a radiologist in the practice, the odds of self-interpretation were about one-half compared to practices without a radiologist on staff,” said Eric W. Christensen, PhD, research director at the Neiman Institute in Reston, VA. “Conversely, the odds of within-practice interpretation were generally 2 to 3 times higher if there was a radiologist in the practice.”
Continuing consolidation of health care—“which is creating larger, multispecialty practices,” Dr. Christensen added—could reduce imaging self-interpretation via increased access to radiologists within practice. “Such centralization of radiology services may encourage referral of imaging interpretation to the within practice radiologist, in lieu of potential self-interpretation.”
Fig. 1—Percentage of office-based diagnostic imaging studies interpreted by radiologist, stratified by modality, presence of in-practice radiologist, and ordering provider’s practice size. NM = nuclear medicine; US = ultrasound; XR = radiography and fluoroscopy.
Training Gaps, Policy Questions, and Equity Decisions Remain
Vijay M. Rao, MD
“Our results raise potential implications for quality of patient care. Nonradiologist specialties, aside from cardiology, lack the rigorous and comprehensive training in imaging interpretation that occurs during the 4 years of a radiology residency program,” said Vijay M. Rao, MD, senior vice president of enterprise radiology at Jefferson Health and professor of radiology at Thomas Jefferson University in Philadelphia, PA.
Pointing out that some specialties may provide targeted training in imaging interpretation that is narrow in scope, such as in ultrasound for emergency medicine or obstetrics/gynecology, “the large differences between radiologists and non-radiologists in interpretation training could lead to differences in diagnostic accuracy,” Dr. Rao said.
Kerry L. Thomas, MD
And as Kerry L. Thomas, MD, noted in her AJR Editorial Comment, while defined personnel qualifications—including for the interpreting physician—are clearly delineated when accrediting outpatient imaging centers, “such quality standards are lacking for the interpreting provider of in-office examinations.”
Importantly, to avoid secondary disparities related to health care quality, “images should be interpreted by providers with appropriate training for the specific examination being reviewed, agnostic of the care setting,” said Dr. Thomas from H. Lee Moffit Cancer Center and the department of diagnostic imaging and interventional radiology at University of South Florida’s Morsani College of Medicine in Tampa.
A “Stark” Surprise
Concerns of financial conflicts of interest related to self-referral contributed to the passage of the federal Stark Law in 1989. Named after U.S. House Representative Pete Stark of California, the Stark Law prohibits physician self-referral for designated health services, including radiology, under Medicare. Over time, certain exceptions (à la the in-office ancillary services rule) were added to allow necessary in-practice imaging referrals within guidelines.
Intended to curb the practice of self-referral, in reality, there remain too few restrictions on imaging interpretation by non-radiologists. And as the authors of this AJR article found, the Stark Law’s in-office ancillary exception greatly weakens its ability to restrict imaging self-referral. “Hence, our results highlight a need to revisit the in-office ancillary exception policy to impact the potential financial incentives that lead to self-referral,” Dr. Rao concluded.
Ralph Drosten, MD Professor Department of Medical Imaging University of Arizona Creighton University Medical School
The term “burnout” dates as far back as 1974. Coined by psychologist Herbert J. Freudenberger in a Journal of Social Issues article entitled “Staff Burn-out,” he described the phenomenon based upon his own experiences working with volunteers at a free clinic in New York City. Freudenberger observed that dedicated workers in this profession were becoming emotionally exhausted, cynical, and less effective—a state he dubbed “burn-out.” This publication marked one of the earliest formal discussions of burnout as a psychological syndrome, particularly among health care and social service professionals.
On May 28, 2019, burnout first appeared in the World Health Organization’s (WHO) 11th Revision of the International Classification of Diseases (ICD-11)—as an occupational phenomenon, however. Highlighting its relevance to health care workers, the ICD-11 filed burnout under “factors influencing health status or contact with health services,” but stopped short of classifying it as a disease. Although burnout is still not classified as a medical condition, in its definition of burnout as a syndrome, the ICD-11 identified three key components that contribute to chronic stress associated with work:
Specific contributors of said burnout include the following: time demands, lack of control, work planning and organization, as well as inherently difficult job situations and interpersonal relationships.
Fortunately, there are several workplace interventions for mentors to mitigate burnout with in-training physicians, such as wellness workshops, workload modifications (e.g., increased diversity of work duties), and better stress management education or appropriate emotional intelligence training.
As individuals, we have our own behavioral interventions to make: meditation, counseling, etc. Social interventions matter, too, especially when promoting our professional relationships. We can’t forget the importance of exercise and other physical activity either.
If not addressed, the risks of burnout are myriad. In addition to increased cardiovascular disease and inflammatory biomarkers, burnout elevates rates of depression and suicidal ideation. Thankfully, plans and attempts in burnout states do tend to decline with recovery.
Importantly, clinician depersonalization is associated with lower patient satisfaction and longer post discharge patient recovery time, so we must be able to identify key physical/psychological symptoms and associated elements of burnout—in ourselves and in others:
The American Roentgen Ray Society (ARRS) proudly recognizes the following four radiologists and their research projects with the 2025 ARRS Resident/Fellow in Radiology Awards:
Jordan H. Chamberlin, MD
Resident/Fellow in Radiology President’s Award “Machine Learning Based Optimization of Root Factors Associated with Image Quality of Myocardial Late Iodine Enhancement”
Shadi Ebrahimian, MD
Resident/Fellow in Radiology Executive Council Award “Evaluating AI Performance in Large Vessel Occlusion Detection: Impact on Time-to-Thrombectomy and Clinical Workflow Efficiency”
Ariel S. Kniss, MD, PhD
Resident/Fellow in Radiology Executive Council Award “Mammographic Breast Density and Its Impact on Screening Performance Metrics: An Analysis of 489,439 Screening Mammograms”
Capt. Tej Mehta, MD
Resident/Fellow in Radiology Melissa Rosado de Christenson Award “Multiparametric, Multimodal Delta-Radiomics for the Prediction of Transarterial Chemoembolization Outcomes in Hepatocellular Carcinoma”
Supported by The Roentgen Fund®, the ARRS Resident/ Fellow in Radiology Awards are available to all ARRS In-Training Members in imaging and allied sciences research to acknowledge their work and present their results during the ARRS Annual Meeting. ARRS Resident/Fellow in Radiology Awards are based on the competence and promise of the candidate in radiological research, education, or administration and the scientific merit and potential impact of the candidate’s research.
Since 1990, The Roentgen Fund has granted millions of dollars to hundreds of imaging professionals for both research pursuits and professional development. Today, through six vital scholarship and fellowship programs, the generosity of The Roentgen Fund’s donors is channeled to every corner of the globe—establishing dual foundations in innovation and leadership for a true diversity of radiology’s next generation.
Scholar Update: Derek Nguyen on Imaging-Focused Management of Architectural Distortions
According to research published in the American Journal of Roentgenology (AJR), imaging surveillance may be a safe alternative to surgical excision for architectural distortions (ADs) detected by digital breast tomosynthesis (DBT) alone with no sonographic correlate showing benign pathology without atypia on core needle biopsy (CNB). “The malignancy rate was 0% for ADs without atypia, versus 20% for ADs with atypia, on CNB,” explained first author and 2022 recipient of The Roentgen Fund’s Melissa Rosado de Christenson Award Derek L. Nguyen, MD, from the radiology department at Duke University School of Medicine in Durham, NC. Dr. Nguyen and colleagues’ AJR accepted manuscript included patients with ADs detected by DBT alone with no ultrasound correlate and nonmalignant results on stereotactic CNB with 12 vacuum-assisted 9-gauge cores from July 1, 2020 to December 31, 2023. ADs detected by DBT alone with no ultrasound correlate showing concordant benign pathology or radial scar without atypia on CNB were recommended to undergo 6-month and 12-month diagnostic imaging follow-up before returning to annual screening, whereas those showing atypia (with or without radial scar) on CNB were recommended to undergo surgical excision; however, patients could electively undergo the alternative management option. Nguyen et al. then assessed malignancy rates, considering ADs to be nonmalignant based on results of repeat CNB, surgical excision, or 12-month diagnostic imaging follow-up. Ultimately, for ADs detected by DBT alone with no ultrasound correlate and nonmalignant results on CNB obtaining 12 vacuum-assisted 9-gauge samples, malignancy rates were 0% (0/94) in the absence of atypia (with or without radial scar), versus 20% (3/15) in the presence of atypia (with or without radial scar), on CNB.
And during the 2025 ARRS Annual Meeting in San Diego, Dr. Nguyen participated in Breast Procedures: Tips, Tricks, and Updates with Tanya Moseley, MD, 2025 ARRS Distinguished Educator of the Year.
2010 Figley Fellow Dr. Jeffrey P. Kanne (far right) presented during one of the two 2025 Roentgen Fund Honorary Lectures. Sponsored by outgoing Roentgen Fund board chair Philip Costello, MD (middle left), Fundamentals of Diffuse Lung Disease honored Mark Parker, MD (middle right).
Roentgen Fund Roll Call
Dozens of prior awardees, like Dr. Nguyen, returned to present during all four days of the 2025 ARRS Annual Meeting in San Diego, CA. Congratulations to these trailblazing scholars and visionary educators—all of whom will continue to shape the future of our specialty:
Opportunities and Obligations in Imaging Patients with Alzheimer’s Disease with Tammie L.S. Benzinger, MD, 2008 ARRS Scholar
Critical Education for Safe, Ethical, and Successful AI in Radiology with Charles E. Kahn Jr., MD, MS, 1993 ARRS Scholar
Wellness Symposium – Creating a Positive Work Environment in Radiology with Christine B. Chung, MD, 2003 Figley Fellow
ARRS Scholar Presentation – Leveraging the “Art of Medicine” within Radiology: Investigation of Report Framing as a Digital Therapeutic To Mitigate Nocebo Effects with Steven A. Rothenberg, MD, BS, 2023 ARRS Scholar
ARRS Scholar Presentation – Deep Learning Tool to Eliminate Nephrographic Phase Images and Reduce Radiation Dose in CT Urography with Andrew L. Wentland, MD, PhD, 2023 ARRS Scholar
Quality and Safety in Radiology – The Unrelenting Pursuit of Excellence with Richard B. Gunderman, MD, PhD, 2011 Berlin Scholar
Cardiac Imaging in the Acute Setting with Jadranka Stojanovska, MD, 2015 Figley Fellow and Brett W. Carter, MD, 2016 Figley Fellow
Challenging Abdominal Cases with Perry J. Pickhardt, MD, 2002 Figley Fellow
Radiology Year in Review with Erin Alaia, MD, 2025 Figley Fellow and Domen Plut, MD, PhD, 2025 Rogers Fellow
Mastering Radiology: A Comprehensive Board Review for Residents and Refresher for Radiologists in Practice with Tanya Moseley, MD, 2025 Distinguished Educator
Categorical Course – Imaging in the ED Musculoskeletal Emergencies: Fractures and Infections with Sameer Raniga, MD, FRCR, 2018 Rogers Fellow
Gastrointestinal Imaging – Gastric Gliomas/Tumors, Bowel Ischemia and Bariatric Surgery with Benjamin Yeh, MD, 2006 ARRS Scholar
GI Post-treatment Imaging with Samuel Galgano, MD, 2022 Figley Fellow
Neuroradiology – CT Radiomics and Machine Learning with Suresh K. Mukherji, MD, 1998 Figley Fellow
Radiology Case Review – Musculoskeletal Imaging with Erin Alaia, MD, 2025 Figley Fellow
Award Winning Exhibits – Gastrointestinal Imaging with Benjamin Yeh, MD, 2006 ARRS Scholar
ABR Update: 2025 with John A. Kaufman, MD, 1996 Figley Fellow
Gastrointestinal Imaging – Hepatocellular Carcinoma with Claude B. Sirlin, MD, 2002 ARRS Scholar
Upper Extremity Challenging Cases with Christine B. Chung, MD, 2003 Figley Fellow
Categorical Course – Comprehensive Insights into Transplant Imaging: Bone Marrow Transplant with Meghan G. Lubner, MD, 2018 Figley Fellow
Neurovascular Disease with Achala S. Vagal, MD, 2012 ARRS Scholar
2024 Distinguished Educator David Naeger, MD (seated) presented Imaging of Lung Nodules and Lung Cancer and served as Course Director for The Roentgen Fund’s Clinician Educator Development Program on Saturday, April 26
The American Roentgen Ray Society (ARRS) proudly announces publication of the inaugural issue of its brand-new, peer-reviewed radiology journal: Roentgen Ray Review.
Marking the 125th anniversary of North America’s very first radiological society, ARRS’ Roentgen Ray Review (R3 for short) will continue to publish image-rich, clinically relevant content each week at R3journal.org.
Edited by John R. Leyendecker, MD, R3’s Pictorial Essays, Clinical Practice Challenges, Case-Based Reviews, Case Reports, and unique article formats like “Don’t Miss This” enable today’s working radiologists to integrate critical knowledge into imaging practices that continue to grow in both volume and complexity. Already, R3 is keeping busy ARRS members up to date on the latest developments in the specialty without compromising their demanding workflow routines.
Among the Volume 1, Issue 1 Roentgen Ray Review articles that our membership can access any time and anywhere are a few that exemplify ARRS’ mission:
Overview of Imaging Intracranial Infections
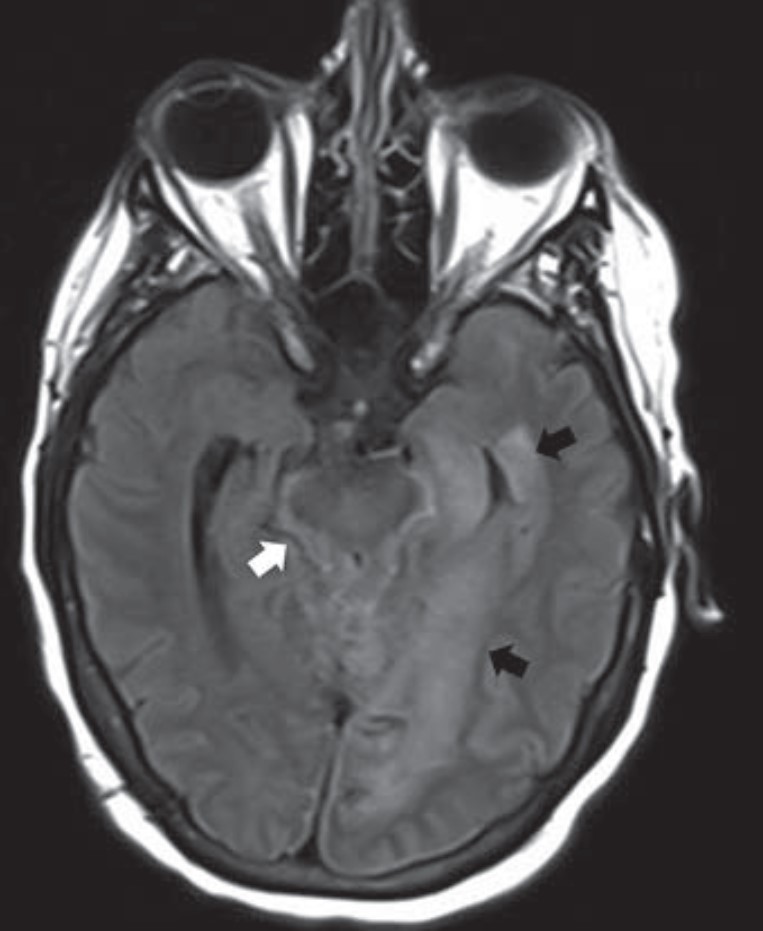
The manifestations of CNS infections are myriad, including diffuse (meningitis, encephalitis, ventriculitis), focal (abscess, empyema), and other special presentations, especially in immunocompromised patients. Diagnosing CNS infections is decidedly multidisciplinary, and as “Overview of Imaging Intracranial Infections” points out, radiology’s contribution to the clinical workup of a patient is paramount. The Roentgen Ray Review’s first entry in its Categorical Course Highlight series, this CME credit article focused on key confounders details how CT and MRI with FLAIR sequencing and DWI can focus your differential diagnosis—ultimately streamlining additional testing and management decisions by the clinical team (Fig. 1).
Fig. 1—64-year-old patient with acute myeloid leukemia and prosthetic hip infection that led to basilar meningitis due to unspeciated fungal infection. Axial FLAIR MR image shows parenchymal edema (black arrows) in left medial temporal lobe and CSF FLAIR nonsuppression (white arrow) in basal cisterns.
Approach to the Lung Cyst With Nodule
Because their imaging features can overlap with benign entities (bullae, fibrosis, bronchiectasis, etc.), lung cancers associated with cystic spaces are often diagnosed at later stages than cancers presenting as solid nodules. Compared to Lung-RADS version 1.1, Lung-RADS v2022’s updated classification and management criteria offer the potential for earlier detection and treatment of cystic cancers. This first Roentgen Ray Review Clinical Practice Challenge with CME tests readers on appropriate management of an atypical pulmonary cyst in a 66-year-old man with a 40-pack-year smoking history who had undergone right upper lobectomy for stage I lung cancer a decade earlier (Fig. 2).
Fig. 2—66-year-old man undergoing baseline lung cancer screening. Axial CT shows 29-mm pulmonary cyst in right lower lobe (arrow).
A Downward Spiral of Knee Pain and Swelling: Use of MRI to Distinguish Lyme Arthritis From Other Pediatric Arthritides
Clinical features of Lyme arthritis overlap with those of both septic arthritis and juvenile idiopathic arthritis, making the diagnosis of Lyme arthritis challenging. As “A Downward Spiral of Knee Pain and Swelling: Use of MRI to Distinguish Lyme Arthritis From Other Pediatric Arthritides” shows, MRI can help differentiate Lyme arthritis of the knee from other entities when certain imaging features, such as popliteal adenopathy, myositis, and lack of subcutaneous edema, are present. This first Roentgen Ray Review Case Report concerns a 13-year-old boy with a 1-month history of knee pain and swelling (Fig. 3).
Fig. 3—Sagittal T2-weighted fat-saturated MRI shows suprapatellar synovitis and effusion (solid black arrow), multiple enlarged popliteal lymph nodes (solid white arrows), and feathery increased popliteus muscle signal consistent with myositis (open arrow).
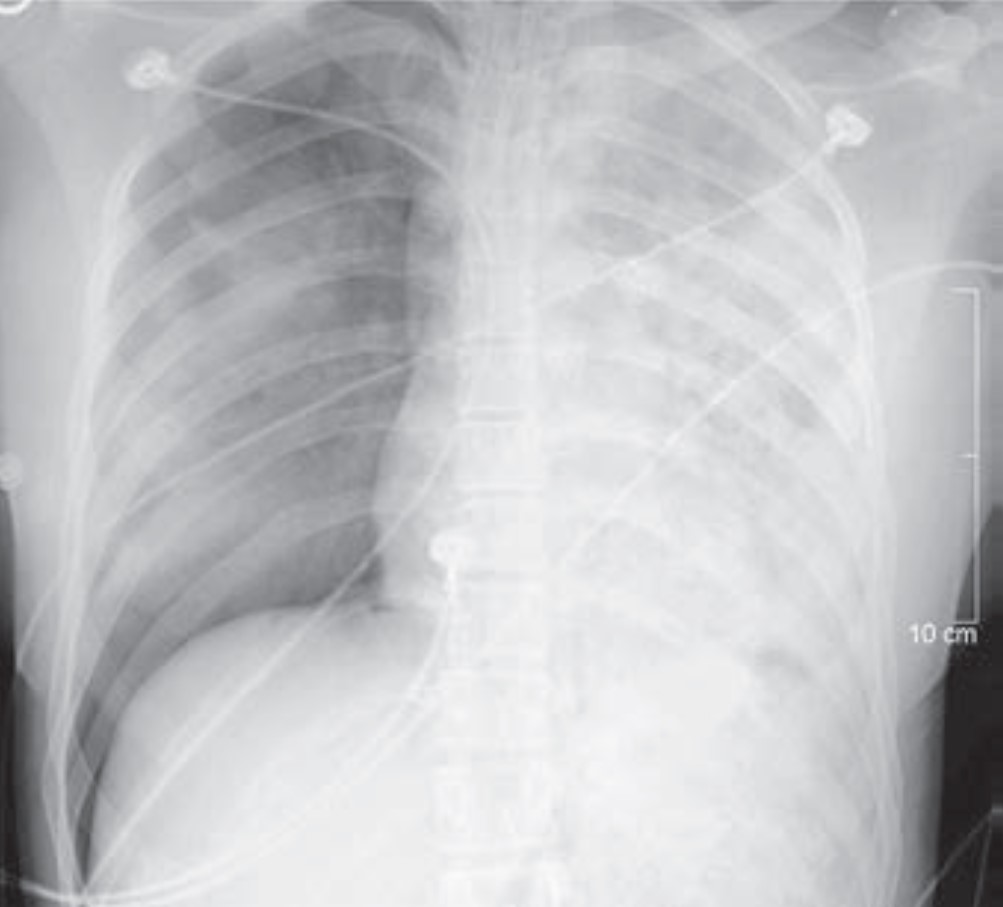
Crucial but Often Unrecognized Radiologic Signs in Thoracic Imaging
Despite its limitations, the chest radiograph is the world’s most frequently ordered and performed diagnostic imaging examination. However, accurately interpretating the chest radiograph remains challenging. “Crucial but Often Unrecognized Radiologic Signs in Thoracic Imaging” is the first of a two-part R3 Case-Based Review with credit highlighting key chest signs radiologists should recognize. Mark S. Parker, MD, presents six unknown cases of underlying abnormalities affecting the lungs, pleura, and mediastinum to help clinically steer your differential diagnosis (Fig. 4).
Fig. 4—Anteroposterior portable chest radiograph of 28-year-old man involved in high-speed motor vehicle collision.
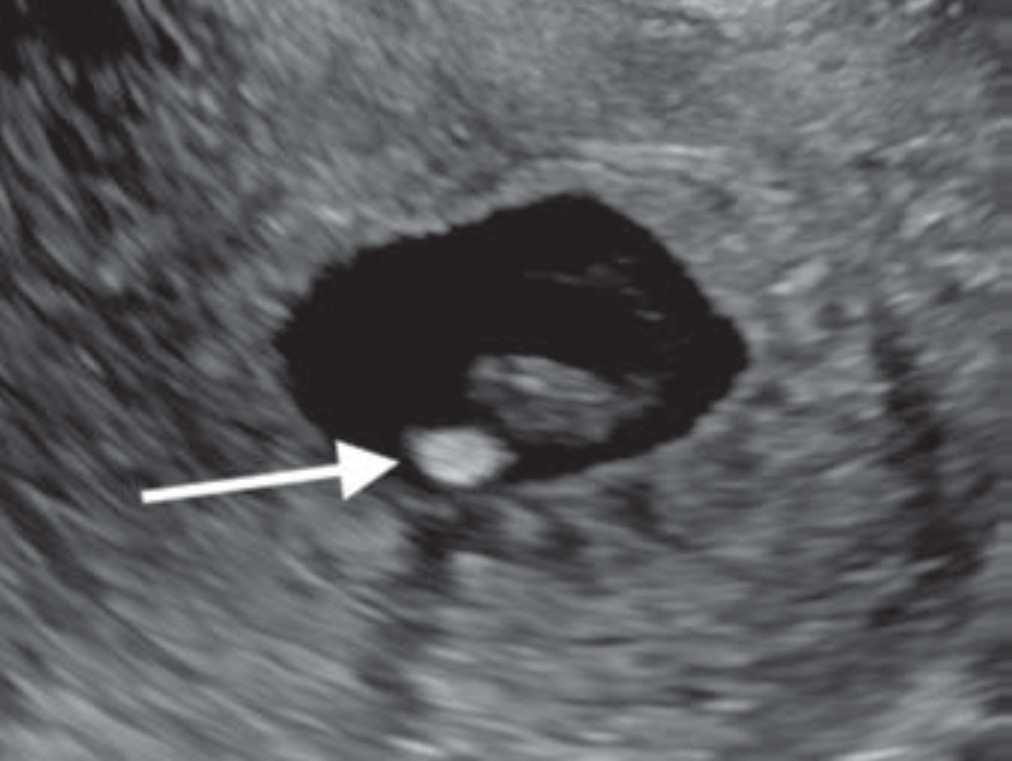
First-Trimester OB Imaging in the Emergency Setting
Radiologists play a key role in detecting early pregnancy, assessing cardiac activity and gestation location, as well as evaluating for complications in the acute setting. Knowledge of potential technical errors in image acquisition and an understanding of possible ectopic implantation locations are also necessary to optimize care of the pregnant patient in the first trimester. “First-Trimester OB Imaging in the Emergency Setting” reviews the pearls and pitfalls of first-trimester ultrasound—early pregnancy development, early pregnancy loss, intrauterine pregnancy of unknown location, ectopic pregnancy—applying the 2024 Society of Radiologists in Ultrasound Consensus Conference’s recommended lexicon throughout (Fig. 5).
Fig. 5—Calcified yolk sac in 23-yearold woman with vaginal bleeding and HCG level of 9300 mIU/mL. Transverse transvaginal ultrasound image shows calcified yolk sac (arrow).
Lateral Trochlear Osteochondritis Dissecans of the Elbow: A Rare and Subtle Finding With Important Implications for Management
Fig. 6—Frontal radiograph of 14-year-old boy with right elbow pain shows rounded lucency at lateral trochlea (arrow).
Given the overlapping ulnar anatomy and subtlety of its radiologic features, even experienced radiologists can miss lateral trochlear osteochondritis dissecans (OCD) of the elbow. As the first Don’t Miss This article in R3 notes, early identification of lateral trochlear OCD allows for appropriate activity modification, as well as timely intervention to mitigate lasting disability (Fig. 6).
Coronary Artery Displacement and Narrowing on CT in the Setting of Giant Sinus of Valsalva Aneurysms
Whereas aortic valve regurgitation and rupture are known complications of sinus of Valsalva aneurysm, this Roentgen Ray Review Case Report illustrates that cardiac ischemia can be a manifestation, too. Presenting a 54-year-old man with large aneurysms involving all three aortic sinuses, “Coronary Artery Displacement and Narrowing on CT in the Setting of Giant Sinus of Valsalva Aneurysms” also illustrates the modality’s value in complex anatomical depictions for proper surgical planning (Fig. 7).
Fig. 7—Left ventricular outflow tract view from contrastenhanced ECG-gated cardiac CT scan shows large aneurysms of right (white arrow) and noncoronary (black arrow) sinuses of Valsalva.
The American Roentgen Ray Society (ARRS) first traveled to San Diego, CA, for the 1996 ARRS Annual Meeting. Almost three decades ago, Kay H. Vydareny of Emory University Hospital in Atlanta, GA, was named this society’s first female president on Sunday, May 5. (Apropos, of the four newly elected 2025–2026 ARRS officers installed on Sunday, April 27, 2025 at the Marriott Marquis Marina, half are women.)
The latest convening of North America’s first radiological society delivered the same clinically relevant experience for which ARRS has long been heralded: radiologists of each practice type and every training level relishing world-class instruction from trusted experts spanning every subspecialty. Pioneers in asynchronous continuing education, ARRS continues to offer both inperson and virtual registrants the most flexible meeting experience in radiology. All attendees retain on-demand access to the complete program for an entire calendar year, learning and earning CME well into 2026.
And speaking of 2026, ARRS looks forward to delivering yet another singular experience in Pittsburgh, PA. This city of steel and bridges has reinvented itself as a hub of health care innovation, making David L. Lawrence Convention Center the perfect host for #ARRS26. Like the city itself, ARRS is constantly evolving— offering new education, fresh perspectives, and invaluable opportunities to connect with peers in meaningful ways. Join us to be part of a dynamic meeting where you’ll gain knowledge, build connections, and experience the energy of a city that’s shaping the future of patient care.
Dr. Deborah Baumgarten presiding over the 2025 ARRS Member Business Meeting
After ratifying an amendment to Article X of the bylaws to clarify that ARRS now publishes two radiology journals—AJR and R3—the ARRS membership officially installed Deborah A. Baumgarten, MD, MPH, of the Mayo Clinic in Jacksonville, FL, as the 125th president of ARRS. An internationally recognized leader in radiology and a steadfast advocate for education, Dr. Baumgarten assumes the presidency after years of distinguished service on the ARRS Executive Council.
Her appointment marks a new chapter in this society’s ongoing mission to advance medical imaging and patient care through expert education, cuttingedge research, and fruitful collaboration. Widely published and highly respected for her clinical expertise, instructional insights, and leadership within the imaging community at large, Dr. Baumgarten succeeds Angelisa M. Paladin, MD, who presented the ARRS presidential gavel to her successor.
Dr. Angelisa Paladin passing the gavel, as well as a gift, to Dr. Deb Baumgarten.
First, Tanya W. Moseley, MD, of the University of Mississippi Medical Center was honored as the 2025 ARRS Distinguished Educator. For more than 20 years, Dr. Moseley’s contributions to ARRS have transformed radiological education. Through her service on key educational committees and roles as casebased breast imaging chair and AJR SA-CME Consultant Editor, she has fundamentally shaped the organization’s educational direction. Her pioneering vision led to the creation of the first multi-vendor tomosynthesis certification course, demonstrating her exceptional ability to build collaborative educational programs. As architect and director of the ARRS Longitudinal Course Series, she continues to advance innovative approaches to radiology education.
Drs. Baumgarten, 2025 ARRS Distinguished Educator Tanya Moseley, and Paladin.
This society was then doubly proud to recognize two recipients of 2025 ARRS Scholarships: Matthew Lee, MD, at the University of Wisconsin School of Medicine and Public Health and Yale School of Medicine’s Luca Pasquini, MD, PhD. Provided by The Roentgen Fund, ARRS Scholarships support early-career faculty members pursuing radiological research that promises to change how medical imaging is practiced. A two-year grant totaling $180,000, the ARRS Scholarship aims to advance emerging scholars, as well as prepare them for positions of leadership.
Drs. Luca Pasquini and Matthew Lee, 2025 ARRS Scholars.
The biggest laurel of the morning, the ARRS Gold Medal, went to Ruth C. Carlos, MD, MS, FACR. Installed as president of ARRS during the 2019 Annual Meeting in Honolulu, HI, presently, Dr. Carlos is a professor at Columbia University Irving Medical Center and associate chair of research faculty development for the radiology department. And as fellow past ARRS president and longtime Michigan colleague N. Reed Dunnick introduced her: “Ruth Carlos isn’t just a superstar. I’d argue that she’s an entire galaxy!” Indeed, having served 11 years on our Executive Committee, as well as 11 ARRS committees prior, Dr. Carlos remains a fixture in our universe. There’s no one more deserving of the highest merit bestowed by this society, which has been honoring distinguished service to radiology for more than four decades.
Dr. Ruth Carlos receives her 2025 ARRS Gold Medal from Paladin.
Service Over Self: Longtime ARRS ED Receives New Lifetime Award
The entirety of the ARRS was eager to give the first-ever ARRS Lifetime Service Award to its former executive director Susan B. Cappitelli, MBA, CAE. “For many of us who have been attending the ARRS Annual Meeting for many years,” Dr. Paladin remarked, “you’ve seen a huge growth in our programming and our services.” Well, that growth started with Susan way back in 1991, when ARRS recruited her to bring every aspect of producing the world’s longest published general radiology journal, AJR, in house. Needing a home for all the talented and dedicated professionals Susan herself was recruiting, six years later, she helped ARRS secure its own office building in Leesburg, VA. The society would go on to use every inch of space, of course, because during Susan’s historic tenure as executive director, ARRS membership increased more than 155%. Meanwhile, the society’s net assets ballooned from just $5 million to over $30 million. Having steered the membership and organization through everything from RVUs to COVID and beyond, “Susan always led with grace,” Dr. Paladin added, “and she will never, ever be forgotten.”
“Innovation is bound to flourish, and innovating is fun. I believe that the society’s commitment to continually learning and improving is why ARRS has grown and produced far beyond its size.”—Susan Cappitelli | ARRS Executive Director, 1999-2024
Welcome to 2025 Honorary ARRS Member, Salvador Amézquita Pérez
Dr. Salvador Amézquita Pérez, president of Sociedad Mexicana de Radiología e Imagen (Mexican Society of Radiology and Imaging), received his honorary ARRS membership on day one, and he and his colleagues were welcomed to the 2025 ARRS Annual Meeting in San Diego as part of the Global Exchange Featuring Mexico. The ARRS-SMRI Sunday Featured Course, “Advances in Cardiac Imaging,” focused on techniques and considerations for evaluating structural heart conditions and coronary artery anomalies. This session addressed non-atherosclerotic coronary artery narrowing, CT’s role in transcatheter mitral valve replacement and adult congenital heart disease, CT perfusion and FFR-CT for myocardial ischemia, as well as CT in TAVR before and after surgery.
Drs. Paladin, Salvador Amézquita Pérez, and Baumgarten.
The mission of the ARRS Global Partner Society Program is to build long-standing relationships with key leaders and organizations in the worldwide imaging community—increasing awareness of our society’s services in specific nations, while raising the stature of Global Partner Societies among ARRS members. Every year, the ARRS Annual Meeting Global Exchange incorporates one partner society into the educational and social fabric of our meeting. ARRS members then reciprocate at the partner society’s meeting that same year. Our 2026 Annual Meeting Global Exchange will welcome a delegation from the Royal Australian New Zealand College of Radiologists to Pittsburgh, PA.
AJR Luncheon Recognizes 2025 Figley and Rogers Journalism Fellows
During the American Journal of Roentgenology (AJR) Luncheon on Monday afternoon, Erin Alaia, MD, of NYU Langone Health in New York City was honored as the 2025 Melvin M. Figley Fellow in Radiology Journalism. Domen Plut, MD, PhD, from Slovenia’s University Medical Centre Ljubljana was recognized as the 2025 Lee F. Rogers International Fellow in Radiology Journalism.
Drs. Domen Plut, AJR Editor in Chief Andrew Rosenkrantz, and Erin Alaia.
Named for two distinguished Editors Emeriti of AJR, the Melvin Figley and Lee Rogers Fellowships offer practicing radiologists an unparalleled opportunity to learn the tenets of medical publishing via “the yellow journal”—the world’s longest continuously published radiology journal. Through hands-on experience with ARRS staff and AJR personnel—as well as personal apprenticeship with AJR’s 13th Editor of Chief, Andrew B. Rosenkrantz— Drs. Alaia and Plut will receive expert instruction in scientific writing and communication, manuscript preparation and editing, peer review processes, journalism ethics, and digital production and publication.
With Distinction: Award-Winning Scientific Research Presented in San Diego
The 2025 ARRS Annual Meeting hosted hundreds of electronic exhibits and abstracts presenting leading-edge research. Below are but a few highlights from our award-winning Scientific Program posters.
Mitigating Disparities in MASLD—Advancing Early Image Detection and Management
According to the Summa Cum Laude Award-Winning Online Poster presented during the 2025 ARRS Annual Meeting, patients with metabolic risk factors and an image diagnosis of steatosis— but without a recognized diagnosis of metabolic-associated steatotic liver disease (MASLD)—were more likely to experience significant complications of chronic liver disease, including cirrhosis and hepatocellular carcinoma (HCC), when compared to patients with a formal MASLD diagnosis. A public health crisis with significant morbidity and mortality implications, “MASLD affects approximately one-fourth of the global population, making it the most chronic liver disease worldwide,” noted lead investigator Emmanuel Mgboji of the University of Michigan Medical School. Using data from his institution’s EMR, Mgboji and fellow Michigan researcher Jessica Fried, MD, identified a cohort of 10,280 subjects with a formal diagnosis of MASLD and 5,103 subjects without a formal MASLD diagnosis but with MRI evidence of hepatic steatosis and metabolic risk factors. After demographic extraction and comparison, Mgboji and Fried monitored each cohort for progression of disease-related outcomes from 2018 to 2023, including HCC, cirrhosis, myocardial infarction (MI), chronic kidney disease (CKD), coronary artery disease (CAD), and type 2 diabetes mellitus (T2DM). Then, after comparing the incident rate and relative risk for each cohort, subjects were stratified by race (n = MASLD Dx; n = Image Dx cohort), including Caucasian Americans (CAs) (n = 8,548; n = 4,227), African Americans (AAs) (n = 580; n = 399), Asian American (ASAs) (n = 599; n = 229), and Hispanic Americans (HA) (n = 433; n = 169). “Comparing incidence rates between the MASLD Dx and Image Dx cohorts (no MASLD Dx cohort),” Mgboji said, “we found a significant relative risk of 2.185 (95% CI: 1.6822–2.8395, p < 0.0001) for a diagnosis of HCC in the Image Dx cohort. Additionally, the relative risk of developing cirrhosis in the Image Dx cohort was 1.459 (95% CI: 1.2934–1.6461, p < 0.0001).” Mgboji and Fried also assessed the risk of being diagnosed with MI, CKD, CAD, and T2DM in the Image Dx cohort, with a relative risk of 1.236 (p = 0.0496), 1.240 (p = 0.0002), 1.346 (p < 0.0001), and 1.259 (p < 0.0001), respectively. “Further significant differences were observed when patients were stratified by racial groups,” added Mgboji. For developing HCC, the relative risk was 2.465 (p < 0.0001) in CAs, 3.488 (p = 0.0180) in AAs, 1.962 (p = 0.375) in ASAs, and 4.270 (p = 0.0451) in HAs. For cirrhosis, relative risk values were 1.590 (p < 0.0001) for CAs, 1.817 (p = 0.0248) for AAs, 1.933 (p = 0.0336) for ASAs, and 2.795 (p = 0.0003) for HAs.
BI-RADS 3 “Report Card” Decreases the Rate of Usage
In the Magna Cum Laude Award- Winning Online Poster at this year’s Annual Meeting, anonymous, peer comparison BI-RADS 3 “report cards” proved to be an effective method of rate reduction, particularly at community hospitals where preintervention rates were higher than at academic sites. Reserved for “probably benign” breast imaging abnormalities that have a low (< 2%) risk of being malignant, in practice, the actual use of ACR’s BI-RADS category 3 assessment varies among radiologists— often overutilized to equivocate a finding. Giving radiologists a recommended target rate of less than 12% as a benchmark, head presenter Bonmyong “Bora” Lee, MD, and her team of researchers from UPenn’s Perelman School of Medicine sent quarterly BI-RADS 3 report cards to each breast imaging radiologist via automated emails. This report card included personal BIRADS category 3 rates for each modality, as well as cumulative rates for the radiologist’s covering site and hospital. Each radiologist was blinded to others’ individual rates, participation was voluntary, and Lee et al. offered neither rewards nor punitive measures for performance. Noting that radiologists were not monitored for review compliance either, “after 4 cycles, we reviewed the data to determine if there were changes in the rate of BI-RADS 3 assessment among radiologists and across the institution using paired t-tests,” Lee said. Over Lee et al.’s 17-month assessment period, 38 radiologists issued BI-RADS 3 in 4,289 total patients: 1,171 diagnostic mammograms, 1,281 screening mammograms, 658 MRI, and 1,179 ultrasound examinations. After Lee and colleagues’ intervention, the average BI-RADS 3 rate decreased (all sites: p < 0.01; community sites: p < 0.01; academic sites: p = 0.07). Radiologists with preintervention BI-RADS 3 rates that were greater than the group median had larger reductions in BI-RADS 3 rates post-intervention (p < 0.05).
Significance of Nonspecific 18F-DCFPyL Rib Uptake on PET/CT in Prostate Cancer Patients
The Cum Laude Award-Winning Online Poster concluded that evaluating increased rib uptake on 18F-DCFPyL PET/CT may be challenging, even resulting in false-positive findings. “In patients without osseous metastasis, the uptake is often low (less than the mean liver SUV), stable, and likely represents benign etiologies, such as fibrous dysplasia, fibrous cortical defect, traumatic fractures, and hemangiomas. Thus, further evaluation is usually not required,” said presenter Aisha Alam, DO, from the Icahn School of Medicine at Mount Sinai in New York, NY. Dr. Alam and her all-Icahn School team performed a retrospective review of patients with prostate cancer who underwent PET/CT scans with radiotracer fluorine-18 2-(3-{1-carboxy-5-[(6-18F]fluoro-pyridine- 3-carbonyl)-amino]-pentyl}-ureido)-pentanedioic acid (18F-DCFPyL) at a single academic center from June 2021 to April 2024. Alam and colleagues’ EHR search identified patients with increased radiotracer rib uptake. The team excluded patients with imaged evidence of osseous metastasis at other sites or with CT suggestive of alternate diagnoses, then analyzed Gleason scores, most recent serum PSA levels, maximum standardized uptake values (SUVmax) in the rib foci, and mean liver SUV. Finally, for confirmation of benignity, follow-up evaluation included stability on 18F-DCFPyL PET/CT and/or imaging modalities such as CT, bone scan, or MRI. With 204 total 18F-DCFPyL PET/CT scans showing solitary or multiple foci of increased rib uptake without CT correlation and imaging evidence of osseous metastatic disease, the mean age was 68 years old, mean Gleason score was 7, mean PSA was 7.9 ng/mL (range: undetectable–50.2 ng/mL), mean SUVmax for rib uptake was 3.8 (range: 1.4–9.8), and mean liver SUV was 5.7 (range: 2.7–10.9). “Of the 204 scans,” Alam noted, “31 studies belonged to 13 patients who underwent follow-up 18F-DCFPyL PET/CT for restaging.” For patients with redemonstrated rib uptake, mean SUVmax was 3.5 and mean SUVmax percent change on subsequent scans was 15.1% (range: 0–46.4%). And for patients with multiple PET/CT scans, the SUVmax for each foci of rib uptake was less than the mean liver SUV (mean: 6.1, range: 4.0–8.8). Of the 23 single-scan PET/CT patients who had a rib uptake greater than the liver mean, 14 of those had a PSA less than 10 ng/mL. “Larger studies evaluating similar findings with histologic correlation and follow-up imaging are needed to improve diagnostic certainty,” added Alam et al.
Analysis of Breast Radiation Therapy and Breast Arterial Calcifications on Screening Mammography
Findings from a Certificate of Merit Online Poster presented during ARRS 2025 suggest that breast radiation therapy exposure does not impact the prevalence of mammographic breast arterial calcification— therefore, not impacting its utility as an imaging biomarker of cardiovascular disease risk. “Our study is the first retrospective analysis of the association between breast cancer radiation therapy exposure and the presence of breast arterial calcification on screening mammography,” noted presenter Jessica Rubino, MD, from Dartmouth Hitchcock Medical Center in Lebanon, NH. Rubino et al. performed an electronic health database query to identify women ages 40–75 years who had a screening mammogram between January 1, 2011 and December 31, 2012. After a chart review to extract data regarding breast cancer radiation therapy history, two breast imaging radiologists then reviewed mammograms for the presence of breast arterial calcification. The researchers used multivariate logistic regression to examine the association between breast radiation therapy exposure and breast arterial calcification, adjusting for age, BMI, smoking status, hypertension, type 2 diabetes, as well as use of statin and antihypertensive medication. Of the 1,155 women included in this analysis, 222 (19.2%) had mammographic evidence of breast arterial calcification, 122 (10.6%) had a history of radiation therapy exposure, and 39 (32%) women with radiation therapy exposure had breast arterial calcification on the index mammogram obtained at least 2 years after completing radiation therapy. Compared to women without radiotherapy, women with a history of breast radiation therapy exposure had higher odds of breast arterial calcification (OR: 2.18, 95% CI: 1.43–3.28; p = 0.0008). After multivariable adjustment, however, this association became nonsignificant, with the maximally adjusted model demonstrating an OR of 1.52 (0.95–2.40; p = 0.07).
Ruben Rajah, MD Comedian and friendly neighborhood radiologist
It is a wet mid-November night in 2022, and I am trudging to an open mic in Manhattan’s lower east side. Apple maps told me the bar was around the corner. It wasn’t. Instead, I found four cop cars boxing in a suspect on a trash-strewn street. I had just moved from Seattle to Jersey City, partly to relaunch my stand-up comedy career. Becoming a comedian is a nocturnal, unglamorous process best pursued by those who are comfortable being ignored and living in the dark—perfect for a radiologist.
I signed up for four lessons in stand-up comedy in the winter of 2007 while working as a nuclear medicine resident in Seattle. The last lesson was a “bringer” gig, meaning we had to invite our friends to watch us perform a five-minute “set” at a comedy club. Radiologists are often understated, but I’m also a comedian…I rocked the house! I blame it on gamma rays altering my neurochemistry (but unlike Bruce Banner, I transformed into a comedian instead of The Hulk). I went on to perform in and around Seattle for two years before the demands of private practice ended my nascent comedy career.
During a vacation in New York City in 2022, I stepped onto a grimy stage at a Manhattan open mic and delivered an old five-minute set. As I walked off the stage, a disheveled figure emerged from the rear of the club. It was the club booker, who told me he liked the set and invited me to perform at Industry Night, as long as I brought five people. I’d been discovered! Reality check: Industry Night books 20 new comics every week. I was just another hopeful among the thousands stepping onto New York stages every night, chasing stardom.
Now, I live two lives—teleradiologist by day and comedian by night. At 3:00 pm, I swap the workstation for a stage. I compete for stage time with people young enough to be my kid. They joke about their sad dating lives, and I make them chuckle with my thoughts on married life and radiology. Three years after that fateful open mic, my wife and I produce Hi Brow Comedy, with shows in Manhattan and Jersey City.
Radiologists are not meant to be humorous. It’s hard to be funny when the public don’t know even know we exist. Just surgeons and ER docs appear in medical dramas. We only have ourselves to blame; we look at black-and-white pictures of organs and talk to ourselves in the dark, like a bunch of color-blind serial killers. I think it’s time the wider world knows that radiologists are real and can be funny. In a way, stand-up can be like radiology. One stares into a spotlight and delivers a monologue. The difference is that the comedian gets rewarded with laughter. As physicians, our profession is about helping and healing, and I believe that laughter is indeed the best medicine. So, maybe we should step out of the dark and into the spotlight.
I am an abdominal radiologist in the abdominal and ultrasound divisions at Mayo Clinic Rochester. Being a radiologist, I have found much of my source of unwellness and burnout tends to be psychological, rather than physical. There is a lot of mental burden, and it is no surprise that radiology is the most mentally demanding physician specialty with increasing workload contributing to burnout [1].
Music is something I have always enjoyed, so I’ve added my three tunes to the ARRS Wellness Playlist on YouTube—songs curated for those mentally tougher days in the reading room, including “Rise Up” by Andra Day, “Fight Song” by Rachel Platten, and “Hero” by Mariah Carey.
Music has been found to improve mood and decrease anxiety and cortisol levels [2], even improving depression [3]. Physiologically, music can decrease blood pressure, heart rate, and respiratory rate [2]. In particular, listening to peaceful and low tempo music has been found to decrease heart rate [4].
There are times in the reading room where I fi nd it useful to have relaxing music to help decrease anxiety and irritation, as well as calm down. However, there are days where I want and need to get pumped up to help tackle a rougher day, just like getting pumped up at the gym for a workout. In fact, motivational music has been shown to combat cognitive and physical performance decline caused by exercise fatigue in sports [5].
The other factor in this study by Bentouati et al. that showed to combat cognitive and physical decline was a 30-minute nap. This also showcases the importance and power of sleep, which we are all very aware of in mitigating burnout and unwellness. Since we are on the topic of sleep, listening to relaxing music has been found to be as effective as diazepam in reducing anxiety [6], and thus benefi cial for aiding sleep. Music can lower our blood pressure, heart rate, and respiratory rate to help us fall asleep and achieve quality sleep, further boosting our wellness.
Build a Community of Belonging During ARRS’ Wellness Symposium in San Diego
Helping us move forward in the wellbeing space during the ARRS Annual Meeting, our 2025 Radiology Wellness Symposium in San Diego, CA will lay out a lot of the hard work done by many imaging centers to shift the narrative in our working environments. The widespread shortage of radiologists, combined with higher volumes and the prevalence of burnout, has been challenging radiology practices of all types.
Focused on hard-won practical solutions for workforce belonging and overall positivity, multi-generational leaders in radiology education, operations, and informatics will tackle the differing approaches for schedule optimization, multiple strategies to help those trainees who are unwell, better incorporation of international medical graduates, and the many benefi ts of proper coaching and mentoring.
As with all ARRS Annual Meeting sessions, live and virtual audience interaction remains welcome, especially during our question-and-answer portions, so I hope to see you in San Diego or online for the 2025 ARRS Wellness Symposium!
References
Harry E, Sinsky C, Dyrbye, LN, et al. Physician task load and the risk of burnout among US physicians in a national survey. Joint Commission Journal on Quality and Patient Safety 2021; 47:76–85. doi.org/10.1016/j.jcjq.2020.09.011
Fancourt D, Ockelford A, Belai, A. The psychoneuroimmunological effects of music: a systematic review and a new model. Brain Behav Immun 2014; 36:15–26. doi.org/10.1016/j.bbi.2013.10.014
Daykin N, Mansfi eld L, Meads C, et al. What works for wellbeing? A systematic review of wellbeing outcomes for music and singing in adults. Perspect Public Health 2018; 138:39–46. doi.org/10.1177/1757913917740391
Sandstrom, GM, Russo, FA. Music hath charms: The effects of valence and arousal on recovery following an acute stressor. Sage Publications 2010. doi.org/10.1177/1943862110371486
Bentouati E, Romdhani M, Abid R, et al. The combined effects of napping and self-selected motivation music during warming up on cognitive and physical performance of karate athletes. Front Physiol 2023; 14:1214504. doi.org/10.3389/fphys.2023.1214504
Berbel P, Moix J, Quintana S. [Music versus diazepam to reduce preoperative anxiety: a randomized controlled clinical trial]. Rev Esp Anestesiol Reanim 2007; 54:355-358. (Estudio comparativo de la efi cacia de la música frente al diazepam para disminuir la ansiedad prequirúirgica: un ensayo clínico controlado y aleatorizado.) doi.org/10.3389/fphys.2023.1214504
Mentors in both private and academic settings are invaluable, providing guidance, support, and expertise that foster professional growth and a sense of belonging. However, based on my experience, mentorship programs can be challenging to implement effectively due to factors such as time constraints, mismatched expectations, and the difficulty of pairing the right mentors with mentees. Despite these challenges, when mentorship programs are well-structured and supported by departmental leadership, they can significantly enhance the development of both trainees and faculty while improving overall job satisfaction.
In our university-based program, all first-year residents are paired with both faculty and upper-level peer mentors. Faculty advisors assist with research projects, while peer mentors provide additional support and guidance. Additionally, junior faculty collaborate with senior faculty to navigate the promotion process successfully. In private practices, many groups focus on integrating new team members and conducting regular check-ins, which are vital for professional development. Team building—especially in the post-COVID era—has become even more critical, and leaders should prioritize creating strong, cohesive teams. Research shows that the most successful work environments thrive when they cultivate a supportive, family-like culture. For example, our department has experienced great success with a monthly departmental walk/run that fosters camaraderie. Additionally, we offer imaging services at an annual clinic for the underserved in Seattle, where faculty, residents, and fellows can volunteer. These events provide valuable opportunities for everyone to connect and engage with each other outside of work.
As leaders, we must focus on ensuring that our trainees and faculty feel valued and that their work matters. Some important questions to consider include: How do we engage our departments in decision-making? How do we ensure equity and transparency, foster a culture of gratitude, and align faculty and trainees with the department’s mission?
In a healthy work environment, the ability to give feedback is essential. It allows team members to voice concerns, suggest improvements, and contribute to the overall health of the department, ultimately improving patient care. I’m fortunate to have a section head who conducts daily rounds, and I can’t overstate how meaningful this is to me. Every day I’m on service, he stops by to check in: “How are you doing? Is there anything you need?” It’s a simple gesture, but it makes me feel valued to have someone actively seek my feedback.
Equity remains a cornerstone of happiness at work. For example, transparency around scheduling, such as publishing call schedules and vacation blocks, is vital to ensuring fairness. Interestingly, I’ve recently heard from more colleagues across the country that their departments are appointing chiefs of wellness. During a visit to Wisconsin, I learned that they have a director of communications and wellness. This trend reflects a growing recognition of the importance of wellness in the workplace. Many departments are now creating newsletters to keep colleagues informed about personal milestones and professional achievements. Like many of us, I enjoy knowing when my colleagues have a birthday, when they publish new research, or when they receive awards. These types of communications help to create a more supportive work environment.
Fig. 1—The five essentials for workplace mental health and wellbeing help organizations develop, institutionalize, and update policies, processes, and practices that best support the mental health and wellbeing of all workers.
In conclusion, the U.S. Surgeon General’s Framework for Workplace Mental Health and Well Being (Fig. 1) is an invaluable resource for launching a wellness initiative within your departments. Ultimately, I hope I’ve demonstrated that happiness is vital to the future of health care. We must show individuals that they matter, that their work holds meaning, and provide the necessary support for them to thrive. By doing so, we will cultivate a resilient community and build a more productive, successful workplace.